
Abstract
Breast cancer survivors often report internal sensations of discomfort that influence body image or the subjective representation of one’s appearance, which can cause a disconnection between body and personal identity. 12 breast cancer survivors were involved in a group psychological intervention which focused on the management of autobiographical memories related to their own body after breast cancer. Three open questions related to their body autobiographical memories were administered pre, post and 1 month later after the intervention. Autobiographical memories were analyzed with a qualitative methodology to explore the transformative process at three time points. Findings highlight three main themes: (1) narratives of cancer-related memories (2) narratives of emotion towards the body after cancer (3) narratives of memories of internal reflections. This innovative psychological group intervention appears to support breast cancer survivors in re-taking control of their own autobiographical memories related to the body and their related emotions.
Introduction
Narrative and autobiographical memories
Since Conway’s (1996) definition, autobiographical memories are commonly understood as personal interpretation of events, rather than the accurate records of what happened. They contain multiple but sometimes biased and/or distorted renderings of previous experiences. Significant autobiographical memories refer to individuals’ central themes and conflicts, yielding simultaneously salient imagery and metaphors as touchstones in the course of intervention (Singer and Blagov, 2004; Singer and Bonalume, 2008). Traumatic events, such as breast cancer diagnosis and its related treatments, are strongly registered in the individuals’ autobiographic memories. Given the reciprocal interconnection between autobiographical memories and self-representations that has been conceptualized as the Self-Memory System (SMS) (Conway et al., 2005), breast cancer survivors may experience intrusive autobiographic memories linked to illness that lead to a disconnect between certain negative self-representations and a healthier holistic sense of self. These assaults on the self by traumatic memory may have long-lasting effects on attitudes, behaviors, mood states, and meaning-making of life events (Martino et al., 2023, 2024). Alternatively, addressing memory narratives as a dynamic source of role-play rather than fixed veridical recollections can encourage insight and behavioral change. According to classic studies by Sullivan (1954), participants can reach a greater understanding and awareness of themselves, minimizing negative emotions and promoting positive emotions. In his book “The Interpersonal Theory of Psychiatry” (2013), Sullivan explored the role of emotions in interpersonal dynamics, highlighting the close ties between awareness of one’s feelings and interpersonal relationships. In this regard, “interpersonal anxiety” (Sullivan, 2013) can limit emotional awareness as individuals may avoid recognizing emotions that threaten their relational security.
Individuals reconstruct the personal past, perceive the present, and anticipate the future in terms of an internalized and evolving self-story, an integrative narrative of the self that provides a sense of unity and purpose to an individual’s life (McAdams, 2008). This process leads not only to the organization of events in a coherent way but also to remembering these events from an integrative perspective. The autobiographical narrative is not a simple externalization of autobiographical memory in which life events, maintained in memory, are mechanically reported to others in the form of a story; this action of externalization entails an important transformation process that draws on the imposition of a narrative structure on to memory. Furthermore, the act of storytelling occurs in social relationships, which are culturally established, so the shift from the autobiographical memory to the autobiographical narrative takes one from the intrapsychic to the interpersonal realm. They are constructed through the lens of the present (hic et nunc), that is, in the perspective of the context of remembering and narrating the past. So, narratives are told to someone and/or to oneself. Consequently, they are constrained by the context of narrating and by whatever the emotional trigger is that activates the process of retrieval and recollection (Nelson and Fivush, 2004). Between memories and the narratives of memories, there is a circular and dynamic relationship of transformation of meanings over time (Freda et al., 2023; Martino et al., 2022) through the re-emergence of autobiographical material and its structuring into a narrative; people can benefit from cognitive and affective information, but also convert their memories into learning opportunities from experience, extrapolating from memory an integrative meaning that can represent a life lesson or insight (Singer and Blagov, 2004b). Studies show that memories of autobiographical narratives are crucial in successful problem-solving, coping processes, and pursuing personal goals (Conway and Pleydell-Pearce, 2000). These kinds of memories serve important directive functions: they inform, guide, motivate, and inspire; they support social relationships and promote self-functions, such as self-continuity (diachronic integration), and they can sustain positive self-regard (Bluck, 2003; Martino et al., 2023). Autobiographical memories, recalled to the level of awareness, reflect the needs of the self. On the one hand, they can engender and regulate emotional processes; on the other, they can play an essential role in protecting and preserving a tolerable self-image.
Narrative autobiographical memories in breast cancer survivors and body image
Autobiographical memories after cancer can strongly influence Body Image (BI), defined as the internal representation of one’s appearance (Thompson et al., 1999). Breast Cancer Survivors (BCS) may continue to confront emotional issues due to relevant changes in their bodies, even after 5 years since the end of oncological treatments and intervention. Specifically, BI involves the mental representation of the body, related emotions, and the overall sense of the bodily self (Lewis-Smith et al., 2018; Sebri et al., 2022) in terms of perceptual (i.e., the accuracy of estimated body size), affective (i.e., sensations and emotions), attitudinal (i.e., subjective satisfaction about one’s own body), cognitive (i.e., appearance beliefs about the body), and behavioral dimensions (i.e., compensatory behaviors such as dieting and physical activity) (Cash and Smolak, 2011). Changes in the body are also strongly associated with damaged aspects of femininity and sexuality (Maass et al., 2015; Sherman et al., 2018). Mastectomy surgery or conservation, for example, may threaten overall self-satisfaction and evoke multiple changes in body perception mediated by sensations within the breast and chest never experienced before (Falbjork et al., 2013; Paterson et al., 2015). Particularly, BCS expressed that their self-image as a woman is disrupted by surgery, highlighting the importance of breasts to a feminine appearance. Treatments constitute much more than the loss of a body part because they have profoundly affected the sense of identity and, as a consequence, the women’s self-esteem and social relationships (Durosini et al., 2021; Fang et al., 2016; Trusson et al., 2016). On an emotional level, the discrepancy between breast cancer survivors’ own current and desired self-representations leads to feelings of dissatisfaction and emotional distress (see the Self Discrepancy Theory by Higgins, 1987). As a result, the subjective changed experience within one’s own BI and related emotions influence social relationships too (Dua et al., 2015), due to increased worries about physical appearance and the development of the belief that others observe and evaluate bodies continually (Hunter, 2015). At the same time, cognitive impairments due to the side-effects of oncological treatments can strongly impact emotional well-being (Sebri et al., 2019). Following the constructionist theory of emotions, being aware of one’s inner sensations is important to regulate one’s internal body state and to maintain physical and emotional well-being by reducing somatic symptoms (Herbert et al., 2012) and attending to subjective emotional feelings (Craig, 2004; Damasio, 1994, 2010; Fustos et al., 2013; James, 1884) that contribute to the representation of an agentic self, that is continuous and consistent over time (Craig, 2010).
Psychological interventions can introduce and manage self-talk aiming to introduce changes in dysfunctional emotional and behavioral patterns. Positive self-talk is a cognitive psychological technique used to counteract negative thoughts that can lead to anxiety, depression, and pessimism, potentially interfering with functioning and performance (Meichenbaum& Deffenbacher, 1988). Athletes often utilize this strategy to maintain focus, enhance motivation, and manage negative thoughts, emotions, and events. In a study by Hamilton and colleagues (2011), the effectiveness of a positive self-talk intervention was demonstrated in improving coping skills and psychological well-being among breast cancer survivors. The psychological intervention involved a 2-h in-person group workshop on positive self-talk, followed by a 10-min “booster” session conducted by telephone. However, to the best of our knowledge, no previous research has examined the management of autobiographical memories related to the BCS’s body. Therefore, in light of survivors’ ongoing bodily issues, well-being, and concern with BI, we considered and analyzed a psychological intervention to narrow this gap in the literature. In particular, the present online psychological intervention for a survivor group addressed autobiographical memories associated with the breast cancer journey (from diagnosis to the end of oncological treatments) and its impact on the BCS’s own body. To elicit memories that would be particularly essential to themes of identity and body image, we employed a prompt to activate “self-defining memories,” a particular type of autobiographical memory that is associated with strong emotion, vivid recall, repetitive rehearsal, a network of similar memories, and is linked to enduring themes and/or conflicts in the individual’s life (Singer and Bonalume, 2010; Singer et al., 2007; Blagov et al., 2022; Singer and Salovey, 1993).
This study aimed to explore themes and highlight transformative processes, in terms of specificity and differences, in the narratives of self-defining memories connected to the body before, at the end and 1 month after the group psychological intervention that targeted women who survived the experience of breast cancer.
Materials and Methods
Institutional review board statement
This study was performed in line with the principles of the Declaration of Helsinki and approved by The Ethics Committee of University of Milan (n45/23, 18th April, 2023).
Participants
12 women with a breast cancer diagnosis in the past (7 years ago, on average) agreed to participate in a psychological research-intervention group focused on the management of self-defining memories about cancer-related issues towards the body. The psychological intervention was carried out in February and March 2023. Participants met the inclusion criteria, as follows: (1) women who are 18 and older years old, (2) people with a diagnosis of breast cancer (at least 5 years ago), (3) absence of oncological treatment ongoing, and (4) understanding and speaking of Italian language. Otherwise, exclusion criteria were related to cognitive impairment, inability to sign the informed consent, and/or mental disorders that prohibited their participation in the study (e.g., women who did not understand the study). Physical and psychological impairments as exclusion criteria have been clarified in the invitation to participate in this study. Lastly, women who showed the development of metastasis elsewhere in the body were excluded. A total of 19 women responded to open questions at the beginning, at the end of the psychological intervention, and 1 month later (age range: 35-61; M age = 49.73; SD age = 7.99). The majority of participants had obtained a bachelor’s degree (63%), lived in the North of Italy (68%), and worked as white-collar employees (94%). Additionally, more than half had received individual psychological therapy in the past (47%), had a partner (58%) and had one or more children (68%).
The bodily traumatic memories program (BTMP): A new group psychological intervention
The psychological intervention consisted of six online weekly sessions. Each session lasted 2 hours and was conducted by an expert psycho-oncologist with extensive professional experience in BI issues. The content of the psychological intervention was based on previous studies focused on body compassion (see below). Starting from psychological theories and validated group interventions using self-defining memories among different populations (Nieto et al., 2019; Raucher-Chéné et al., 2021), the main goal was the promotion of a positive BI after oncological treatments. Particularly, the psychological program explored and reframed the self-defining memories connected to the body parts, especially those affected by breast cancer. The groups promoted the integration and transformation of self-defining memories linked to the breast cancer journey (from diagnosis to treatment and the end of oncological interventions), drawing on the power of the membership dynamics. Overall, the main objective was to increase positive interoceptive sensations and re-appraisal of the overall relationship with the body and its related emotions and behaviors by elaborating and managing self-defining memories associated with breast cancer. The present psychological intervention aimed to help survivors: (1) reframe self-defining memories related to bodily awareness after breast cancer. Specifically, breast cancer survivors may seek to reframe self-defining memories linked to their own body, with a specific focus on bodily parts affected by breast cancer; (2) draw on the reframing of self-defining memories related to one’s own body after breast cancer to promote self-coherence and enhance psychological well-being by reducing the negative emotions associated with the body in participants’ self-defining memories and coping body image issues following cancer.
Procedure
The project was conducted between March and June 2023. The invitation to participate in the online programs was posted on social networks and sent via a commercial mailing list. First, a self-selection method was applied to recruit participants interested in the present research-intervention group project. They received an email with the information sheet and were briefed about the contents of the psychological interventions, how the sessions were organized, and the request to respond to three open questions at three different points in time. After agreeing to participate in the study and confirming their eligibility, women were asked to sign a consent form. Particularly, the signed consent was scanned and returned to researchers online. Then, they participated in six online psychological sessions in a group conducted by a psychologist with expertise in psycho-oncological issues (Figure 1). Procedure and timing.
A week before starting the psychological intervention, all participants filled out a questionnaire consisting of three open questions, focusing on memories related to the body, the associated emotions and cognitions, as follows: (1) To date, how would you describe the memories related to your body? Are they usually positive or negative? Try to give examples; (2) To date, what emotions do you feel when you feel sensations in your body? And when don’t you feel them? (3) To date, what do you think about when you feel sensations in your body? And when you don’t feel them? Subsequently, participants participated in the group psychological intervention. At the end and 1 month later, all participants responded to the same questions as before the intervention. All the answers were completed individually by each participant in written form. Personal information was deleted to guarantee anonymity. All the textual answers were collected through a Qualtrics platform and analyzed by the research team involved in this study.
The contents of the psychological intervention were as follows: - Session 1: The psychologist explained the procedures to the group. Then, a brief group “icebreaker” in which the women introduced themselves and their reasons for attending the program were exchanged. The psychologist introduced some theoretical background on BI; subsequently, participants discussed their definition of BI and their thoughts, emotions, and behaviors. Specifically, maladaptive cognitive, emotional, and behavioral attributes associated with BI before and after diagnosis and oncological treatments were described and reflections were shared with the group. Finally, an exploration of individual expectations was shared, enabling each participant to define their specific goals for the sessions. - Session 2: The psychologist shared an oral narrative prompt with the group (i.e., women listened to the voice of the researcher who encouraged them to recall their breast ‘cancer traumatic memories; soft music was played in the background). This prompt activated their storytelling of autobiographical memories related to their bodies after breast cancer. Specifically, women were invited to recall three self-defining memories related to their breast cancer journey. Then, the psychologist assisted the participants in elaborating on these self-defining memories associated with their experience of breast cancer, aiding them to provide as many details as possible. The psychologist asked them to select and describe some specific events connected to their breast cancer journey (e.g., at diagnosis time, during oncological treatments, and relationships with others during this time). They were encouraged to engage in a reappraisal process of their self-defining memories and, as a consequence, generate more affirming and resilient perspectives on these memories. Women were invited to share their memories and related emotions with the group. - Session 3: In the third session, participants discussed their own body, starting from the question “How do I see/perceive my body before and after cancer?”. First, they wrote about barriers and affirming factors in their daily relationship with their body, addressing what predisposes them to a negative BI individually. Then, they shared their thoughts and emotions with the other members of the group. During this process, the psychologist helped participants regulate coping behaviors (e.g., avoidance, checking), which worsened BI distress in the longer term. To achieve coping behavior regulation, the facilitator assisted the women in identifying their primary coping strategies, emphasizing their benefits and limitations. By addressing any dysfunctions, participants were guided in finding effective strategies tailored to their specific issues. Moreover, on an emotional level, women were free to share their feelings associated with their body perceptions. Women had the possibility to share their emotions, especially if related to fear of cancer and frustration. It was a highly evocative session on an emotional level, allowing for expressing feelings and emotions that had never been expressed before. In the end, specific behavioral strategies for improving positive behaviors towards their body were provided. - Session 4: Women discussed how they perceive their own body, while assessing others’ points of view. First, they reflected on the relevant bodily attributes in their social and intimate relationships. Then, they shared their thoughts and emotions with the group’s others. In the third session, the psychologist introduced functional coping behaviors and cognitive distortions in autobiographical memories and, particularly, self-defining memories. Women were guided to identify dysfunctional BI-related schema (e.g., cognitive errors) and replace faulty self-talk with new positive self-expressions. Additionally, the psycho-oncologist focused on emotional expression as the present topic of interest. For instance, participants were asked to describe if and how they usually share emotions with others, family, and friends. - Session 5: In the fifth session, the participants presented the self-defining memories related to their own bodies after breast cancer that had emerged in the first meeting. Moreover, they provided a name to the memories, highlighting changes after intervention. They actively explored and defined new meanings related to these evolving autobiographic memories. Accordingly, women changed the endings of their original memory descriptions, as well as changed their attitudes toward some phases of their breast cancer experience. They employed an imagery technique to reframe or reorient their understand of the memory narrative.
As a definition, the imagery technique is a type of mind-body intervention commonly used in clinical practice. It encourages individuals to adopt alternative perspectives, thoughts, or behaviors that enhance one’s coping skills and reduce stress (Sebri et al., 2024). This technique involves giving verbal instructions to direct the participant’s focus toward visual or auditory sensations that elicit a positive psychological response. Instructions can be delivered directly by someone or through media (e.g., an audio-recorded voice). Particularly for breast cancer survivors, a review and meta-analysis published by Shina and colleagues (2021) stated that the imagery technique was effective in decreasing stress and anxiety, improving Quality of Life. Accordingly, in the present study, each woman was free to manage their self-defining memories as she preferred, aiming at elaborating on traumatic events and defining new meanings related to breast cancer and its impact on the body. Finally, the psychologist promoted the integration of autobiographical memories into the overall self to avoid self-fragmentation. Women were instructed to stay in contact with their inner sensations daily, to incorporate memory restructuring exercises, and to reinforce the emotional and behavioral positive consequences of these changes in their memory narratives. - Session 6: Finally, women reviewed their goals before and at the end of the intervention and received feedback about attained changes from the group facilitator. They reflected on what vulnerabilities were activated and unfolded in day-to-day thoughts, emotions, and behaviors and how they learned to stop negative self-perpetuating cycles. Finally, goals for further needed changes were set.
Method of data analysis
According to the study aims, the analytical process identified the more frequent words the participants used to speak about their memories related to the body, before, at the end of the intervention, and 1 month later. A total of 60 answers were analyzed, with 20 sentences examined each time. Specifically, we conducted a qualitative thematic analysis with a bottom-up approach (Braun and Clarke, 2006), allowing for the analysis of the patients’ experiences and feelings. Adopting an inductive approach, we did not try to fit the data into a pre-existing frame, but, starting from three main themes (i.e., relationship, emotions, and thoughts towards their body), subthemes were identified through a “bottom-up” process (Clarke et al., 2015). In other words, the three main categories were grouped after collecting and analyzing patients’ responses. It is fundamental for our study to focus on the themes emerging from the participants’ experiences rather than trying to fit the obtained results into a pre-existing coding frame. As described by Braun and Clarke (2006), the analytical process employed the main phases of qualitative thematic analysis. Researchers were involved in data collection and interpretation in different ways, as follows: first, two authors (V.S. and M.L.) read each text many times to familiarize themselves with and understand the contents. Then, an initial coding was applied to the data to identify segments of the textual reports (semantic content). This way, researchers considered a single segment containing one main bodily relationship/emotion/thought. Third, the different codes were categorized into potential main themes and sub-themes. Fourth, the thematic map was reviewed by two authors (V.S. and M.L.) and possible discrepancies were resolved through discussion. Finally, the sub-themes were labeled. This provided an explicit and defined clarification of the contents, which allowed us to complete the thematic analysis. One author (G.P.), who did not participate in the previous analysis phases, reviewed the coding process and the identified sub-themes to validate the thematic map further. This way, results obtained from the present thematic analysis highlighted the participants’ experiences and feelings, providing data that could explain their opinions and behaviors in an explicitly way.
Findings
The present study collected answers of a heterogeneous length, ranging from a few-word statements to a paragraph of almost 60 words. To explore possible differences in the self-defining memories and their related emotions after psychological intervention, a Thematic Analysis was conducted on the whole data. Possible group transformations were assessed in three times; before, at the end, and 1 month after the intervention.
Main Themes and sub-themes related to narrative of body memories.
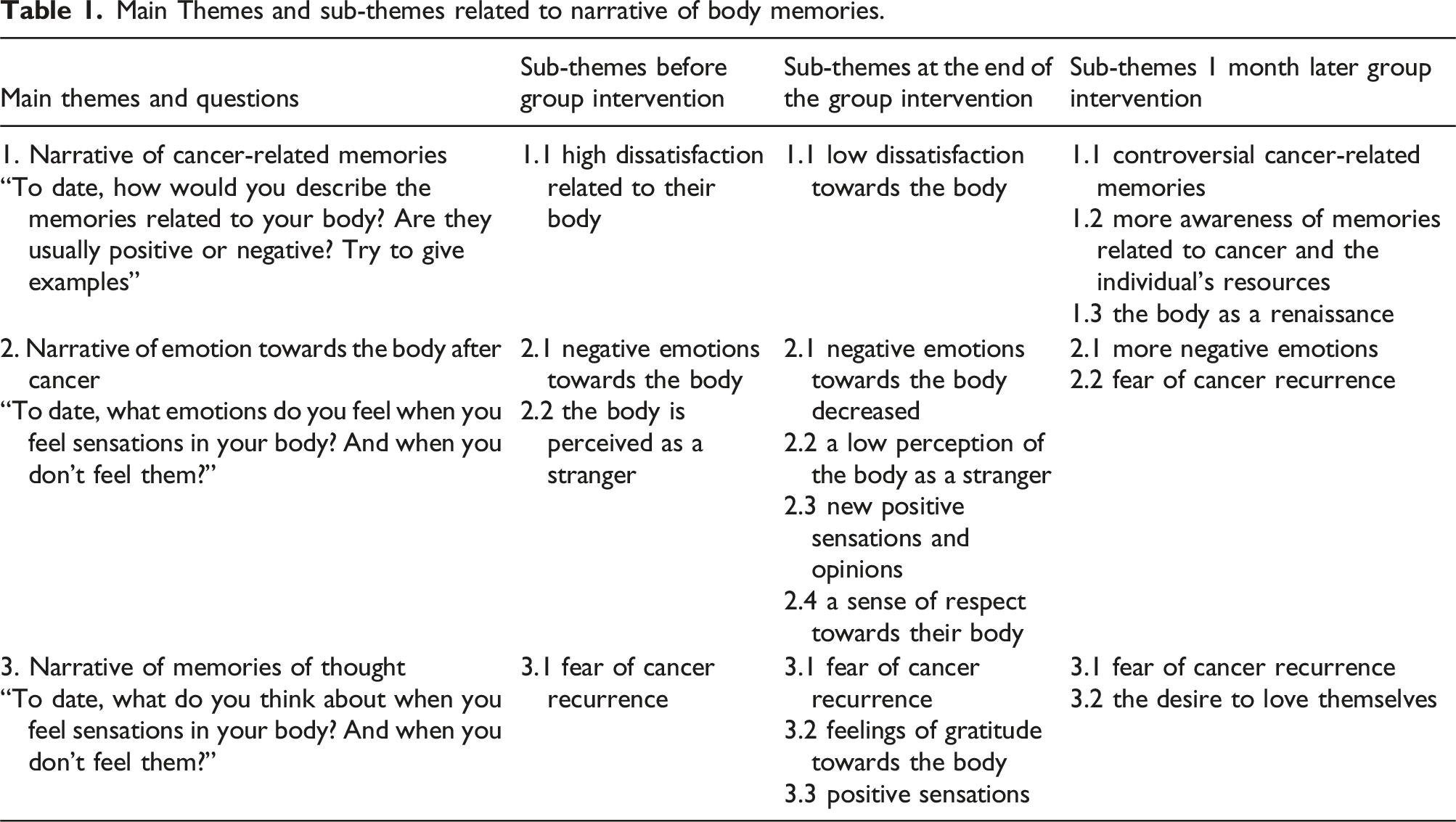
Main theme: Narrative of cancer-related memories
Regarding narratives of cancer-related memories, before the group intervention many women reported dissatisfaction related to their body. For example, one woman reported that her dissatisfaction related to her body is related to her expectations: “Speaking about my body, I am not really positive, I try not to pay attention to it but I am not satisfied. The asymmetry of the two breasts is not the biggest problem, I mean...I have a hard time accepting the weight gain of the last few years” (ID5). Another reported dissatisfaction concerning the inability to recognize herself, due to her body changes: “The memories of my body are positive before the tumor, but today I don’t recognize myself anymore, I have fat on my back, shoulder blades, thighs, big butt, double chin. I don’t like myself and I don’t recognize myself” (ID7). Moreover, another one emphasized her physical capacities are compromised: “My memories are negative compared to the past, but even now I am no longer the same both aesthetically and in terms of physical and mental endurance. I can’t resist fatigue and I can’t concentrate on my studies, and I get tired easily” (ID19).
At the end of the group intervention
After 1 month from the group intervention, cancer-related memories were more nuanced; at the same time, women reported being more conscious of them and more aware of their resources to struggle with body-related problems. Specifically, a woman cited: “I still have negative illness-related memories. Nonetheless, currently I think that my body reacts well to the ‘shocks’ of life” (ID4) and “If I try to focus on memories related to the body, I realize that I am reminded of episodes in which I have been injured. A fall, a sprained ankle, etc.” (ID12). This is in line with improvements in self-esteem and self-appreciation, which is the second main theme that emerged: “I feel much more of a woman, and I look in the mirror and like myself more than before and feel greater self-esteem” (ID8). Furthermore, breast cancer survivors reported thinking of their body as engaged in a renaissance. Particularly, they stated: “My scars are a sign of rebirth” (ID16). However, some breast cancer survivors still reported negative memories 1 month later. “Memories are not very positive, the scar on my breast is very present!” (ID3) and “Memories of my body before the tumor are very positive, I was a beautiful girl admired and sought after. Now I am ugly, fat, unwatchable” (ID6), which highlight their difficulties in positively dealing with bodily memories in the long run.
To sum up, the main theme related to the narrative of cancer-related memories evidenced that many women reported dissatisfaction with their bodies due to changes caused by cancer. After psychological intervention, participants noticed a noticeable improvement in body appreciation. Their perceptions of their bodies became more nuanced and less negative, with some expressing a more positive and complex view of their bodies as repositories of personal stories and emotions. One month later, women reported greater self-awareness and recognition of their body’s resilience, viewing their scars as symbols of renewal. However, some continued to have negative memories related to their bodies.
Main Theme: Narrative of emotion towards the body after cancer
Before the group intervention, participants reported memories significantly associated with negative emotions. In particular, the breast cancer survivors reported sadness as one of their most common emotions in contemplating their bodies. Interestingly, a participant reported a high level of sadness, which is part of an overall perception of negative emotions, as follows: “”I feel sadness, so much sadness, I have only negative feelings” (ID9). Thinking of negative emotions, a participant specifically made an association between bad sensations and feelings and the inability to perceive sensitivity in their breasts. In this regard, a breast cancer survivor indicated: “Thinking of my body, I feel bad feelings due to less sensitivity in the breasts and laterally following bilateral mastectomy” (ID7). Participants also reported that negative emotions are linked to the perception of their body as a stranger, as in the following sentences: “I feel sadness, so much sadness, I have only negative feelings. I have the feeling that my body does not belong to me, that is, I am living in the body of another. It is a stranger to me” (ID17) and “I have the feeling that my body does not belong to me, that is, I am living in the body of another” (ID9)”. Interestingly, perceiving the body as a stranger could increase the tendency to “create distance” from their bodies and breasts. For instance, a participant expressed that: “Sometimes I wanted to pull my breasts off because I feel them as a foreign part of my body. I can’t touch my scars!” (ID7).
A few participants continued to report negative emotions at the end of the group intervention. In contrast, more participants indicated their emotions changed strongly, providing space to experience more positive sensations and fostering attempts to improve relaxation. For instance, a participant stated: “Thinking of my body after cancer, I feel a little fear but generally I try to relax so as not to get anxious” (ID4). At the same time, virtually no participants reported the perception of a stranger’s body at the end of the intervention. Only one participant said “When I have pain, I feel sad because this greatly limits my daily life. The rare occasions when I don’t have pain all over my body I am disoriented. In general, I do not recognize my body at all” (ID13). In contrast, for many of the group participants, new sensations and opinions emerged at the end of the intervention, as in the following sentences: “For my body I always feel great respect, I love my body with all its flaws” (ID5) and “As of today, I am more aware of my body, the feelings have changed, I am no longer ashamed of them, I like myself much more even with all the flaws that are now more obvious, even with the scars, with the spots, with age” (ID15). Thus, women reported new perceptions related to a sense of respect towards their body and a better awareness of it and its sensations.
Negative emotions were also reported one month after group intervention, as in the following sentences: “My body sensations are always related to the pain I feel, lately the most frequent emotion is tiredness” (ID3), “I feel fear if I hear anything...even slight abnormal...and false alarms...I experience them all as tragedies” (ID6), and “Sometimes I get nervous and feel demoralized and powerless. I don't feel physical issues when I distract myself” (ID9). In particular, a participant highlighted the perception of fear: “Today, I feel fear and only fear. When I don't hear them, I stay quiet” (ID5)”, while another one provided evidence of trouble in her relationship with her body, as follows: “I often fear that my body will never be the same again” (ID14). Negative emotions were sometimes associated with the fear of cancer recurrence, even some years after oncological interventions: “Sometimes I am afraid the cancer is back” (ID5), “Sometimes I am afraid of the disease, that it will recur” (ID7), and “I feel concern. I only pay attention to my body's sensations when they are discomfort or small pains. From cancer experience my alertness threshold is a little lower” (ID10).
In this second theme, women predominantly reported negative emotions related to their BI. Many breast cancer survivors expressed significant sadness and discomfort due to a loss of sensitivity in their breasts and a sense of estrangement from their bodies, increasing the distance between themselves and their physical appearance. By the end of the group intervention, fewer participants reported negative emotions, and there was a notable shift towards more positive feelings and attempts to relax. Most participants no longer felt estranged from their bodies and began to express greater respect and acceptance towards themselves, including their flaws and scars. However, some participants still experienced negative emotions and fears about their health, such as pain, tiredness, and anxiety about potential cancer recurrence. This ongoing fear and concern, rooted in their cancer experiences, occasionally led to heightened sensitivity to bodily sensations and discomfort.
Main theme: Narrative of memories about cancer-related thoughts
The third theme was related to the fear of cancer recurrence, which is reported as recurrent and persistent in data collection before, after intervention, and 1 month later. Indeed, no significant differences before, at the end of the group intervention, and 1 month later were observed. At the same time, after the intervention and 1 month later, the participants indicated a determination to think more positively about their bodies despite the lingering fear of relapse.
In this regard, before intervention, a participant affirmed that: “Every day I fear that the disease may return” (ID3). In this case, thoughts of fear of cancer recurrence are daily and persistent, in reflective ways. More specifically, another breast cancer survivor stated: “I have a permanent sensation of fear, especially when I feel strange sensations (burning etc.)” (ID10). Accordingly, thoughts of fear of cancer recurrence can be associated with the sensations of a body as a stranger, in line with narrative memories in reference to emotions towards the body. This way, perceiving bodily sensations could increase ruminative thinking related to the fear of cancer recurrence. Inner sensations are sometimes perceived as a source of danger and fear, being associated with cancer symptoms.
As mentioned above, sentences regarding the fear of cancer recurrence did not change significantly at the end of the group intervention: “Every new physical sensation arouses my attention and the thought that there may be something wrong. If I don't feel anything, it means to me that everything is fine”, highlighting that “do not feel anything” is the only one way to be well. Some women reported feelings of gratitude towards their body and positive sensations, as follows: “When I think of my body as it was, I feel gratitude, because it gave me a lot. But deep down, my body, as it is now, is also a great ally” (ID14) and “I feel joy when I think that I am alive and considering that my diagnosis came after a screening checkup without which I would not be here right now and considering that I had performed a breast examination five months earlier. I am grateful to be here.” (ID9).
One month after the group intervention
The third and last theme encompassed the persistent fear of cancer recurrence, which remained a consistent concern throughout the intervention phases. In addition, many participants frequently expressed daily and ruminative fears about cancer returning, sometimes exacerbated by perceiving their bodies as foreign or unfamiliar. After the intervention and 1 month later, participants reported increased gratitude towards their bodies and positive sensations. They began to appreciate their bodies for their resilience and expressed a renewed focus on gratitude and self-love. Despite ongoing fears and challenges, they acknowledged their body’s strengths and committed to nurturing a positive body image.
Discussion
The analysis of autobiographical memories of breast cancer survivors with regard to the experience of cancer-related emotions and thoughts related to the body offers the possibility to investigate the trajectory of the transformative processes mediated by a group intervention over three data collection points (before, at the end of the intervention, and the follow-up).
First, referring to memories related to the experience of cancer, the present qualitative analysis shows that the body during the experience of illness is remembered in association with physical damages and mutilations (e.g., mastectomy and scars) at the baseline (Sebri et al., 2023a; Martino et al., 2021). The body is usually defined as a ‘broken shell’ and something that is broken, in line with the “Injured Self” construct (Sebri et al., 2021). In other words, participants reported a change of bodily identity, with several consequences for perceived beauty, self-efficacy, and performance. Specifically, women often reported their perception of being “patients” or “women at risk”, and not people, leading to rethinking goals and future expectations with a focus on their health management, even several years after the end of oncological treatments (Sebri et al., 2023a, 2023b). The narration of these memories seems to highlight, as established in the literature (Brockmeier, 2009; Frank, 1998), a gap between an ideal and current bodily representation. This gap exacerbates negative emotions due to the impossibility of regaining one’s aesthetic appearance before breast cancer.
Before group intervention, these memories held the potential to be transformed from depictions of the body as a “broken” and injured, and instead emerge as a symbolic container inhabited by more positive reframing and associated thoughts that can ground a more positive sense of self. One must first acknowledge that these bodily memory narratives encompass a history of negative and high-impact experiences that endured over months and, in some cases, years. The lingering bodily consequences of the cancer experience due to invasive therapies are associated with the fear of cancer recurrence, leading to persisting anxiety and distress (Cash et al., 2011). However, some women reported that bodily signs can also have also the role of “teaching something” to the self, highlighting how they were brave and resilient in managing the illness and its related symptoms (McAdams, 2001).
This process of narrative modification and integration of one’s cancer story related to the body finds its turning point 1 month later after group intervention where the autobiographical memories are more incorporated into the continuity of the self and contextualized into a healthier and strengths-based self-conception (Habermas et al., 2015). Negative and dysfunctional bodily memories are not only a watershed that highlights a discontinuity between patients’ lives before and after breast cancer but also an experience of learning about oneself and a catalyst for post-traumatic growth (Tedeschi and Calhoun, 2004). This attributional shift toward growth is fundamental because some memories remain fixated on losing of bodily efficiency and perfection. Therefore, positive mediation of the memory narrative can support an integrated and overall bodily identity, reducing negative ideation and associated negative emotions before, during, and after breast cancer.
Regarding the emotions related to the bodily memories following the cancer, in the present study findings did not show a reduction in negative emotions. On the contrary, the memories and related negative bodily emotions reappear as significant and dysfunctional 1 month later. Bodily signals may trigger negative emotions over time, activating the retrieval of traumatic and intrusive memories regarding the onset of the disease and their related oncological treatments (Dalgleish et al., 2008). In line with the literature, perceptions of a damaged and ill bodily image can evoke the perception of weakness and loss of control even some years later (McGinty et al., 2016). The body retains the traumatic memory of disruption and invasion. On the other hand, psychological intervention can encourage the interpretation of these sensations and emotions as they emerge, leading to healthier and more adaptive meaning frameworks related to acceptance and self-love. Nevertheless, the salience of bodily sensations associated with the trauma and their intrusiveness can re-emerge (Dalgleish et al., 2008). Thus, it is relevant to propose consistent and longitudinal psychological interventio to manage negative emotions in the long run and to construct an enduring reframing (Samide and Ritchey, 2021). It seems conceivable that the level of emotions linked to the sensations evoked by the body is one of the most complex and hard-to-treat factors in health psychology. The value of internalized strategies that survivors can practice independently, such as guided imagery and mindfulness, cannot be overestimated.
In line with this, memories of thoughts linked to the sensations of one’s body are usually recurrent and intrusive memories connected to the fear of the return of the disease. The power of embodied reminders (Sebri et al., 2023c) and the memory of bodily sensations that the mind has archived as dangerous are fundamental to be considered. However, at the end of the intervention, memories emerged, and these thoughts were often linked to the cognitive representation of one’s own body as a great ally. Participants expressed pride that their bodies had managed to survive. They shared the desire to trust and love their bodies again. Accordingly, previous literature and the current study have demonstrated that psychological interventions can be helpful to learn how to manage negative bodily sensations and their related dysfunctional emotions, supporting the possibility of a renewed and healthy relationship with one’s body (Sebri et al., 2023c).
Conclusion
The present study points to the possibility of expanding the process of acceptance and integration of the breast cancer experience in long-term survival through a focus on modifying important self-defining memories related to the experience. As study limitations, we have to consider the low number of participants as well as the absence of a control group. Additionally, delivering the intervention online rather than in person could be a limitation for those with difficulties with online devices, such as older individuals. However, although further studies will be needed to assess the effectiveness of such an intervention from a psychological-clinical point of view, this pilot study suggests a promising trajectory of work to promote well-being and quality of life in a breast cancer survivor setting. The BTMP, as illustrated in this article, provides the possibility to develop better psychological interventions and related protocols that can increasingly support women’s needs during and after the disease. The findings of this study highlight how autobiographical memories can generate valuable insights into women’s functioning, their coping mechanisms, and overall styles of illness adaptation. Autobiographical memories offered a meaningful insight into women’s narrative identity by revealing the continuity of the illness experience across the lifespan. From a psychological perspective, the knowledge of how individuals have internalized their relationship with illness, the treatments they underwent, and their resulting body image, can aid in understanding the recovery processes that women are undergoing and their resilience in response to their illness and its aftermath. While reframing body-related memories linked to the illness experience can promote positive self-growth, a current and complex challenge for breast cancer survivors is associated with emotions and feelings related to the signals of their own bodies. Bodily signals can evoke distress on several levels. Although the accompanying thoughts could support a narrative reappraisal process, emotions and sensations related to body signals can still evoke anguish and fear over years. They can persist despite thoughtful efforts at cognitive restructuring. Therefore, as clinical implications, we believe that addressing and managing autobiographical memories is fundamental not only over the long-term survival period, but from an early stage of the disease in order to support a functional sense of coherence and positive meanings. Lastly, BTPM seems to have allowed women to be able to explicate aspects of themselves related to their bodies and feelings in a protected context within a space and time frame chosen by each woman. In other words, online meetings can represent a place to care for oneself by retracing memories of one’s history and connecting them with the present In some cases, participants could also discover other points of view from their peers and the facilitator, which was helpful in defining their emotions and behaviors better. Similarly, it enabled them to normalize their understandable fragilities, recognizing the same fears and feelings in other women’s stories.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Federico II University of Naples; San Paolo Company Foundation FRA PROJECT, MEMO-PRO.