
Abstract
Care for individuals with dementia, predominantly provided by family members, was associated with significant physical and emotional stress. Existing guidelines for supporting caregivers were frequently based on limited evidence. A cross-sectional clinical study involving 104 pairs of caregivers and individuals with dementia was conducted. The study evaluated psychological stress, anxiety, and depression levels among family caregivers, alongside the severity of dementia and challenges with daily activities faced by the individuals with dementia. The findings demonstrated that the severity of dementia in patients had a statistically significant impact on the psychological stress experienced by family caregivers, as did the challenges associated with daily activities. Furthermore, caregiver anxiety was shown to exacerbate their psychological burden, an effect amplified by greater difficulties in daily activities and higher dementia severity. Additionally, it was observed that caregivers’ psychological stress increased in correlation with heightened levels of depression, irrespective of the severity of dementia or the patient’s difficulties with daily activities.
Keywords
Introduction
Age-related neurodegenerative diseases are a significant social problem that has recently become particularly acute, primarily in developed countries, given the marked increase in human life expectancy. Dementia is one of the most challenging healthcare issues, not only for patients but also for their families. The number of people with dementia (PWD) is growing worldwide, and forecasts generally suggest a significant increase in overall prevalence as the population ages. According to the World Health Organization, the number of people living with dementia is estimated to be 55.2 million in 2019, rising to 78 million by 2030 and 139 million by 2050. (The Lancet Public Health, 2021).
The global population is ageing, which is increasing the number of dementia cases. The prevalence and mortality rates of dementia among the elderly in the United States have increased significantly during the last 30 years. Between 1990 and 2019, the number of dementia cases among the elderly in the United States increased by over 1.37 million. Forecasts for 2030 predict roughly 4 million instances of dementia and 160,000 related deaths, with a significant increase in frequency and mortality among individuals aged 80 to 89 years (Cao et al., 2024). The most common among them are Alzheimer’s disease (AD) and Parkinson’s disease (PD), which affect 1-4% of the total elderly population. Age-related cognitive impairment is a growing global challenge, especially in Ukraine (Aborode et al., 2022b; Shkodina et al., 2022).
Caring for a person with dementia is a challenging experience that leads to physical and emotional exhaustion. Behavioural and mental symptoms of dementia are associated with caregiver distress, depending on the type of relationship with the patient. Family caregivers are primarily responsible for caring for PWD. Unfortunately, this can lead to high physical and emotional stress levels, particularly for those caring for loved ones with dementia. Addressing this pressing issue is critical to improving the quality of care for these patients. There is a potential risk of strain and psychological distress caused by changes in the mental state of PWD. Daily care requires the maximum involvement of caregivers’ adaptation processes and the activation of psychosocial resources (Hogan et al., 2022; Zhang et al., 2023).
Family caregivers often have to provide most of the care for their loved ones with dementia due to the insufficient availability of professional dementia care services. Caregivers of PWD often have poor mental, physical, and social health. A high frequency of depressive and anxiety symptoms, as well as grief, has been reported among caregivers of PWD. Caregivers of dementia patients grieve the loss long before the death of their relative due to the loss of personality and intelligence, which is reflected in the popular culture description of the anticipatory grief (Basu and Mukhopadhyay, 2021).
In recent decades, several global guidelines have been proposed to help caregivers of PWD improve their well-being. Unfortunately, many guidelines have been found to be based on insufficient evidence. Research in the UK found that 9% of adults quit their jobs or reduced their working hours to care for a relative with dementia, leading to loneliness, depression and financial difficulties (Gao et al., 2022).
With the rising number of people affected by dementia worldwide, the existing healthcare system is struggling to offer the best possible medical care to all patients. Putting more pressure on healthcare institutions means additional costs and forcing them to explore scientifically proven, efficient alternative healthcare models that involve family and community care while keeping patients in their familiar surroundings (Aborode et al., 2022a; Zhdan et al., 2018).
Studies focus on the impact of the severity of dementia and the daily activities of the person being cared for on the caregiver burden. However, we suggest that the carer’s psychological state, including anxiety and depression, is an equally important factor influencing the caregivers’ distress and may combine with the effect of the patient’s condition.
The aim of the study was to analyse the impact of the interaction between patient factors of PWD and the mental state of their family caregivers on the level of psychological distress in caregivers.
Methods and materials
Study design and settings
We conducted a cross-sectional clinical study to analyse the mental well-being of family caregivers of PWD, which was conducted in November 2021-January 2022 in Ukraine. Recruitment of participants was terminated due to the Russian-Ukrainian war, which directly affected the mental health of the Ukrainian population and could act as a factor in modifying the study parameters. The study and its protocol amendments were approved by the local bioethics committee.
The study was conducted among caregivers whose relatives were hospitalized for palliative care in the municipal enterprise “Regional Psychiatric Care Institution of [Poltava Regional Council]”. Caregivers and PWD were recruited in the study on the first day of hospitalization. After the study procedures were explained to them, they could take home a questionnaire and a consent form to read. The next day, after giving informed consent, the caregivers underwent sociodemographic, clinical, psychopathological and psychodiagnostic tests and received the necessary outpatient care. A clinical assessment of the severity of the underlying disorder and its symptoms was carried out on the first day of the PWD’s hospitalization in an inpatient unit.
Participants
The study included 104 pairs of family caregivers and their PWD. The inclusion criteria for family caregivers were: informed consent of the caregiver, age of 25 years and older, care of a single patient with a previous clinical diagnosis of dementia (regardless of its genesis), first-line family relationship with PWD they care for, and living in the same family as the patient.
Exclusion criteria: - HIV-associated dementia in the patient; - inability of the caregiver to stay with the patient with dementia (at least 5 times a week, at least 4 hours a day); - incapacitated persons; - less than 9 years of patient’s education; - oncological diseases of any location in the caregiver or patient, - somatic and neurological diseases in the acute or decompensation stage in the caregiver, for instance heart failure, migraine, history of stroke, chronic pain, postoperative period, etc. - pregnancy of the caregiver, - alcohol or drug addiction of the caregiver.
Variables
For the study, we interviewed both family caregivers and PWD for whom they cared. We assessed the severity of dementia and difficulties with activity of daily living (DADL) of PWD and the level of psychological stress, anxiety, and depression of their family caregivers.
Data measurement
The level of psychological stress experienced by family caregivers was assessed using the 25-item version of the Psychological Stress Measure (PSM-25) (Cronbach’s α for Ukrainian translation is 0.86). This tool aims to evaluate stress-related feelings based on somatic, behavioural, and emotional indicators. The integral indicator of psychological stress is determined by calculating the sum of all answers. A higher score indicates a more significant level of psychological stress. If the score is more than 155 points, it means the respondent is experiencing a high level of stress, which could result in mental discomfort and maladjustment. To manage this, they may need to explore different methods to reduce neuropsychological tension, find relief, and alter their way of thinking and living. Scoring between 154 and 100 points indicates an average stress level, while a score of under 100 points indicates that they are psychologically adjusted to their workload (Lemyre et al., 1990).
The level of anxiety in family caregivers was measured by assessing the results of the Beck Anxiety Inventory (BAI). The test is designed to be self-administered and provides a quantitative measure of anxiety. It has 21 questions that help identify emotional, physical, and cognitive symptoms of anxiety. To determine the level of anxiety, add up the scores for all items on the scale. A score of 0 to 7 means there is minimal anxiety, 8 to 15 suggests mild anxiety, 16 to 25 indicates moderate anxiety and a score of 26 to 63 indicates severe anxiety (Boiko et al., 2023).
The level of depression was assessed using the Beck Depression Inventory (BDI-II), which consists of 21 items, each of which contains several options for statements. The presence of depression is established if the subject scored more than 25 points in total. A score of 0 to 9 points indicates the absence of depressive tendencies and a good emotional state. A score of 10 to 13 points indicates minimal symptoms of depression, 14 to 19 points is mild depression, 20 to 28 points corresponds to moderate depression, and 29 to 63 points corresponds to severe depression (Boiko et al., 2021).
The study assessed the symptoms of PWD that may be factors of increased psychological stress in family caregivers. To this end, patients were assessed for the severity of dementia using the Mini-Mental State Examination. The MMSE is the most commonly used brief screening and assessment scale for cognitive impairment, which includes simple questions and tasks in several areas: time and place of the test, repetitive word lists, arithmetic, such as serial subtraction of seven, language use and understanding, and basic motor skills. The maximum total score is 30. A score of more than 23 corresponds to normal values, 13 to 23 to mild dementia, 5 to 12 to moderate dementia, and less than 5 to severe dementia (Kim et al., 2021).
We also analysed the level of dependency on the daily functioning of PWD according to the Bristol Activities of Daily Living Scale (BADLS). The BADLS was developed specifically for PWD and consists of 20 daily activities (questions). This questionnaire is aimed at identifying the daily abilities of people who have certain memory problems (Boyd et al., 2018).
Grouping
Caregivers of PWD were divided into groups depending on the level of psychological stress according to the PSM-25 questionnaire to analyse the severity of affective syndromes: Group 1 (n = 33) - caregivers with a low level of stress; Group 2 (n = 38) - caregivers with an average level of stress; Group 3 (n = 33) - caregivers with a high level of stress.
Statistical methods
Statistical analysis was performed using EZR Statistics v.1.13 and Microsoft Office Excel 2019. Qualitative variables were presented as absolute values (abs) and relative values (r). The χ2-Pearson test with Yates’ correction was used to compare qualitative data. Quantitative variables are presented as arithmetic mean (M) and standard deviation (SD) or standard error (SE). Comparative analysis of quantitative variables between the 3 groups was performed using one-way analysis of variance (ANOVA) with Bonferroni correction. Correlation analysis was performed using Pearson’s correlation criterion. The influence of qualitative attributes on the quantitative variable considering their interaction, was carried out by multi-way ANOVA. Results were considered statistically significant at p < .05.
Results
Social and demographic parameters of the studied caregivers.

Characteristics of the psycho-emotional state of family caregivers and their patients with dementia, M ± SD.
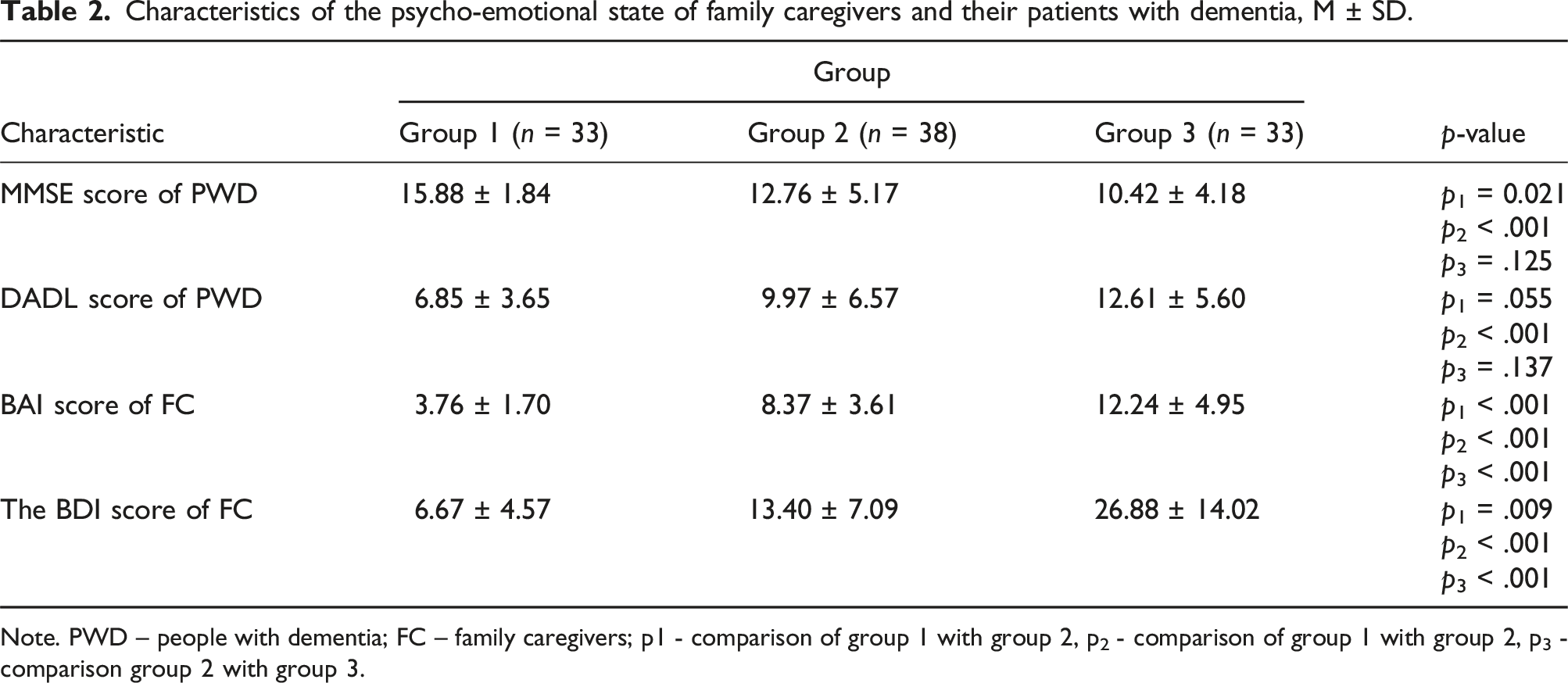
Note. PWD – people with dementia; FC – family caregivers; p1 - comparison of group 1 with group 2, p2 - comparison of group 1 with group 2, p3 - comparison group 2 with group 3.
Among family caregivers in group 1, the severity of cognitive impairment in the person being cared for was statistically significantly lower compared to group 2 and group 3. At the same time, DADL of PWD were more expressed in family caregivers of group 3 compared to group 1, but no significant differences were found between groups 1 and 2, as well as between groups 2 and 3. The severity of anxiety and depression was higher in group 3 compared to groups 1 and 2 and higher in group 2 compared to group 1.
To assess the degree of association between the severity of psychological stress and the studied indicators, we conducted a correlation analysis, which demonstrated a direct correlation between the family caregiver’s score on the PSM-25 scale and score on the BAI scale (r = 0.679, p < .001), BDI-II scale (r = 0.583, p < .001), the score of the PWD on the BADLS scale (r = 0.335, p = .001) and the score of PWD on the MMSE scale (r = −0.338, p < .001).
To assess the impact of PWD characteristics on the level of psychological stress of their family caregivers, we analysed the influence of factors and their interaction, as shown in Figure 1. The analysis demonstrated that the severity of dementia in a patient has a statistically significant effect on the level of psychological stress of their family caregiver (F = 14.96, p < .001), as well as the occurrence of DADL (F = 14.56, p < .001). However, the interaction of these factors was not statistically significant (F = 1.79, p = .172), indicating the independent influence of dementia severity (η2 = 0.234) and DADL (η2 = 0.129), which together account for about 37% of the variance in the dependent variable (R2adj = 0.371). The severity of psychological stress of family caregivers depends on the severity of cognitive disorders and difficulties with activities of daily living of people with dementia, M ± SE.
Among family caregivers of PWD without DADL, the level of psychological stress was 103.28 ± 6.02 points in mild dementia, 96.61 ± 5.33 points in moderate dementia and 135.64 ± 7.71 points in severe dementia. At the same time, when comparing family caregivers whose patients had DADL, the level of psychological stress was found to be 116.5 ± 8.08 points in mild dementia, 130.17 ± 6.02 points in moderate dementia and 149.54 ± 5.22 points in severe dementia. The obtained indicators indicate that in the absence of DADL in PWD, the level of psychological stress of his/her family caregiver is higher in severe dementia compared to caregivers of persons with mild and moderate dementia. At the same time, no differences were found between the former. When a PWD have DADL, the level of psychological stress of the caregiver is statistically significantly higher in severe and moderate dementia compared to caregivers whose patients had mild dementia. No statistically significant differences were found between family caregivers of people with moderate and severe dementia and those with DADL.
When adding the factor of family caregivers’ anxiety, a statistically significant effect was found on the level of psychological stress of this factor alone (F = 21.01, p < .001), its interaction with the occurrence of DADL (F = 2.77, p = .047) and its interaction with DADL and the severity of dementia of the person being cared for (F = 3.33, p = .014), as shown in Figure 2. The severity of psychological stress in different levels of anxiety in the family caregiver depends on the different severity of cognitive disorders and difficulties with activities of daily living of the people with dementia, M ± SE. (A – the absence of difficulties in daily activities, B - the presence of difficulties in daily activities).
This suggests an isolated effect of family caregiver anxiety on their level of psychological stress (η2 = 0.435), which may also interact with the occurrence of DADL (η2 = 0.092) and have a variety of effects in different severity of dementia (η2 = 0.140). The model of interaction of the assessed patient factors with the caregivers’ anxiety level explained almost 69% of the total variance in the dependent variable (R2adj = 0.686).
Among caregivers of PWD without DADL, a low level of psychological stress was found regardless of the severity of dementia in the absence of anxiety in the caregiver (93.91 ± 5.44 points for mild dementia, 80.17 ± 4.51 points for moderate dementia and 85.00 ± 12.76 points in severe dementia) and a moderate level of psychological stress in the occurrence of mild or moderate anxiety (116.17 ± 7.36 points and 129.00 ± 18.04 points, respectively, in mild dementia, 131.67 ± 10.41 points and 136.00 ± 9.02 points, respectively, in moderate dementia, and 131.00 ± 12.76 and 148.4 ± 8.07 points, respectively, in severe dementia). Severe anxiety was observed only in caregivers whose PWD had severe dementia without DADL. In these caregivers, the mean value of the level of psychological stress corresponded to a high degree and was 159.00 ± 12.76.
Among family caregivers of PWD who had DADL, a low level of psychological stress was determined in the absence of caregiver anxiety and mild dementia, which was 84.75 ± 9.02 points. A high level of psychological stress was identified in family caregivers with a high level of anxiety in people with mild dementia and DADL, the mean value of which was 170.00 ± 18.04. In other cases, family caregivers of PWD with DADL had a moderate level of stress; namely, caregivers of people with mild dementia and DADL had a mean score of 113.00 ± 10.41 for mild anxiety and 158.50 ± 12.76 for moderate anxiety. Family caregivers of people with moderate dementia had a score of 103.50 ± 12.76 points for no caregiver anxiety, 129.50 ± 7.36 points for mild caregiver anxiety, 133.56 ± 6.01 points for moderate anxiety, and 157.00 ± 18.04 points for severe anxiety. Among caregivers of people with severe dementia and DADL, the scores were 157.00 ± 12.76 points for no anxiety in the caregiver, 138.00 ± 12.76 points for mild anxiety, 147.60 ± 4.67 points for moderate anxiety, and 157.00 ± 8.07 points for severe anxiety.
Thus, there is a tendency to potentiate the development of psychological stress in the presence of anxiety in family caregivers in response to the severity of dementia and DADL in the PWD being cared for.
When adding the factor of the level of depression in family caregivers, a statistically significant effect on the level of psychological stress was found for this factor alone (F = 7.65, p < .001), as shown in Figure 3. The severity of psychological stress in different levels of depression in the family caregiver depends on the different severity of cognitive disorders and difficulties with activities of daily living of the people with dementia, M ± SE. (A - the absence of difficulties in daily activities, B - the presence of difficulties in daily activities).
However, the influence of other factors and their interactions were not statistically significant. Thus, we demonstrated an isolated effect of the severity of family caregiver depression on their level of psychological stress (η2 = 0.221), which is not related to the condition of the PWD. The model for assessing the influence of patient’s condition factors, considering the level of caregiver’s depression, describes almost 49% of the total variance of the dependent variable (R2adj = 0.488).
We have identified a tendency for the level of psychological stress to increase with the severity of depression of family caregivers of PWD without a statistically significant association with the severity of dementia or DADL. Among caregivers of people with mild dementia without DADL, the level of psychological stress was 102.20 ± 24.75 points in the absence of depression in the caregiver, 115.50 ± 27.57 points in the mild degree, and 95 points in 1 person with a moderate degree of depression. In the presence of DADL in people with mild dementia, their family caregivers scored 96.33 ± 25.18 points in the absence of depression, 100 points in 1 person with mild depression, 158 points in 1 person with moderate depression and 164.50 ± 7.71 points in severe depression. Caregivers of people with moderate dementia without DADL showed a stress level of 90.11 ± 28.69 points in the absence of depression. 125.00 ± 7.07 points in mild depression, 136 points in 1 person with moderate depression and 124 points in 1 person with severe depression, and with the presence of DADL is 123.0 ± 24.61 points, 129.50 ± 7.07 points, 150.67 ± 16.44 points and 130 points in 1 person, respectively, in the absence, mild, moderate and severe depression. In family caregivers of people with severe dementia, in the absence of DADL, the level of psychological stress was found to be 107.00 ± 42.15 points in the absence of depression, 132.75 ± 18, 95 points in mild depression, 161.00 ± 2.83 points in moderate depression, 159.00 ± 2.83 points in severe depression, and in the presence of DADL is 141.67 ± 26.63 points, 149.80 ± 13.51 points, 149.78 ± 14.78 points and 152.43 ± 11.46 points, respectively.
Discussion
Dementia is common in older people worldwide, and several studies have been conducted to investigate this issue. In most countries, the age-standardized prevalence of dementia is between 5% and 7% (Lopez and Kuller, 2019). Caregiving is so well suited to the chronic stress paradigm that it has been used as a model for studying the effects of chronic stress on health. Family caregivers of the elderly, in particular, have reported health problems such as fatigue and accidents because of caring for elderly parents. Institutionalization may even be chosen as a way out of the caregiving role in case of high burden. This has significant health consequences for both care recipients and caregivers as it reduces the quality of care and the ability to age well (Cheng, 2017; Vitaliano et al., 2003).
Caregiving has some advantageous psychological consequences, but it also has numerous negative impacts, such as high levels of stress, tiredness, anxiety, and depression. According to a recent meta-analysis, about half of caregivers of PWD report burden (Collins and Kishita, 2020). Caregivers experience uncertainty just as much as patients do. The most prevalent sources of stress are the severity of symptoms, lack of personal boundaries, repetitious and aggressive behaviour, and the need for ongoing care (Unson et al., 2015). As the population ages, the prevalence of dementia is expected to increase exponentially. This is associated with an increase in the number of family caregivers for PWD. To develop appropriate interventions, it is essential to identify factors related to caregivers’ mental health.
In our study, we discovered an association between the levels of psychological stress experienced by family caregivers and the severity of dementia and the DADL of the patient under care. Although one earlier study revealed that higher symptom severity was connected with better mental health of the family caregiver, it is worth mentioning that similar findings in that study were associated with lower emotional severity of the caregiver and better family functioning (Altamirano and Weisman De Mamani, 2021).
The analysis showed that the severity of the patient’s dementia has a statistically significant effect on the level of psychological stress of the family caregiver, as well as the presence of DADL. At the same time, there was no significant interaction between these factors. It is worth noting that the daily activity in PWD is not always correlated with the severity of cognitive decline. However, it could also be a result of coexisting somatic diseases. Previous research has found correlations between the caregivers’ functional daytime activities and caregiver burden and psychological distress (Razani et al., 2007). On the other hand, cognitive function and the number of care hours were directly related to the caregiver burden. Social support, family functioning, and caregiving experience may moderate the relationship between patient factors and caregiver burden (Yu et al., 2015). Social maladjustment has an important role to play in the treatment of various diseases, such as schizophrenia (Boiko et al., 2017) and dementia (De Vugt and Dröes, 2017). At the same time, it may be significant for caregivers’ quality of life (Morrison et al., 2020).
Caregivers of PWD are also affected by contextual, social and cultural factors that contribute to changes in their mental state (Messina et al., 2022). Therefore, our study examined the depression and anxiety of the caregiver as factors influencing psychological burden. We found that anxiety in caregivers increases their psychological burden. At the same time, the presence of DADL and a higher severity of dementia potentiate this effect.
Depression is more common in caregivers of PWD in the general population. The reason for depression among caregivers is multifaceted, although it is assumed to be related to care for patients (Huang, 2022). Regardless of the severity of the dementia or the patients’ DADL, our study found that caregivers’ psychological stress increased as the amount of depression increased. Prolonged psychological stress has long-term harmful consequences for health. It is known that oxidative stress, which occurs as a result of immunological changes caused by psychosocial stress, plays an essential role in the development of depression and vice versa. In addition, oxidative stress is crucial in numerous metabolic and neurological diseases (Boiko et al., 2022).
Family caregivers of PWD need adequate psychological support because they are exposed to many factors that cause psychological stress. Our findings highlight the importance of considering the mental well-being of caregivers when developing support strategies. This includes identifying levels of anxiety and depression, which can exacerbate psychological stress, as well as considering the patient’s dementia severity and activity of daily living.
Our study has revealed that the mental stress experienced by caregivers is greatly intensified by both cognitive dysfunction and disruptions in daily activities, and is further compounded by the complex interplay between the two. These findings highlight the necessity for specific interventions that target the various challenges faced by caregivers, and emphasize the urgent need for increased support and resources to help them cope with the demands of their role.
It should be noted that our study had limitations. Although many studies show that women are more active in informal care than men, most caregivers in our study were men. For example, data from different countries suggest that women account for between 57 and 81% of all caregivers of older people (del-Pino-Casado et al., 2012; Iwuagwu et al., 2022). At the same time, men may have some differences in emotional reactions compared with women (Zhyvotovska et al., 2020). We also did not examine other dementia symptoms, such as apathy or psychosis, or its clinical forms, such as Alzheimer’s disease, dementia with Levy bodies, or frontotemporal lobe dementia, which might have an impact on caregivers’ mental health (Cheng, 2017; Tsai et al., 2022). Although our study did not cover time spent caring, it has been demonstrated in other studies that a considerable number of PWD caregivers have a high degree of stress, which rises over time (Connors et al., 2020). Researchers are currently exploring methods to positively impact the caregiver and PWD dyad and enhance their quality of life. While there is evidence that joint activities and positive experiences can be beneficial, the exact mechanism of this impact is not yet fully understood (Sideman et al., 2023).
Understanding the factors that affect the mental health of caregivers of PWD may prevent early admission to nursing homes and reduce adverse health outcomes. Developing a health strategy that includes psychological support for these caregivers is essential. Our research suggests that in addition to the severity of the patient’s dementia and their functional ability, caregivers’ levels of anxiety and depression should be considered as risk factors for caregiver stress that will help improve the quality of care.
Footnotes
Author contributions
Conceptualization: Olha V. Orlova, Dmytro I. Boiko, Liliia V. Zhyvotovska; Data curation: Olha V. Orlova, Formal analysis and investigation: Olha V. Orlova, Dmytro I. Boiko; Methodology: Dmytro I. Boiko, Lesya A. Bodnar; Supervision: Liliia V. Zhyvotovska, Visualization: Dmytro I. Boiko, Writing - original draft: Olha V. Orlova, Lesya A. Bodnar; Writing - review and editing: Dmytro I. Boiko, Liliia V. Zhyvotovska.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Poltava State Medical University (project state registration number 0121U108235).