
Abstract
Health-related worries can be either self-directed or occur in close relationships by proxy (e.g., among parents, couples, or pet owners). Our aim was to test the feasibility of assessing health anxiety by proxy in parents and to examine the relationship of health anxiety with family well-being. Health anxiety by proxy was measured between parent-child and parent-partner relationships with adapted versions of the modified Short Health Anxiety Inventory. Parents reported significantly higher levels of health anxiety by proxy regarding their child than for themselves, t (585) = −3.61, p < .001. Exploratory factor analysis showed that each health anxiety questionnaire formed a distinct latent factor. Parenting stress and poorer family functioning had small associations with health anxiety towards one’s self, child, and partner (r = 0.15 to r = 0.20). Further research is needed to determine clinical relevance and its impact on health behaviors and functioning within the family unit.
Introduction
Health anxiety is characterized by disproportionate concerns about one’s own health and a preoccupation with having or acquiring a serious disease accompanied by high levels of stress or misinterpretation of bodily symptoms as threatful (Asmundson et al., 2010; Rask et al., 2020). Severe health anxiety is associated with increased health care utilization and negative well-being outcomes. Epidemiological studies suggest that health anxiety concerns approximately 2.1 to 13.1% of the general population (Weck et al., 2014). Affected individuals exhibit dysfunctional health behaviors, ranging from maladaptive coping strategies like avoidance of health consultations to excessive contact with health services, which has an impact on health care system costs (Fink et al., 2010). Elevated health anxiety is associated with more functional impairment, disability, lower quality of life and higher risk for psychiatric treatment (Bleichhard and Hiller, 2007; Sunderland et al., 2013; Horenstein and Heimberg, 2020).
Recent research has expanded the study of health anxiety beyond one’s own health. Health anxiety that relates to another individual has been described as health anxiety by proxy and has been mainly examined among parent-child dyads (Aziz et al., 2018; Lockhart, 2016; Thorgaard et al., 2017a) and among expectant mothers (Harpel, 2008; Reiser and Wright, 2019). Affected parents show dysfunctional cognitive, behavioral, and emotional outcomes such as negative illness perceptions, frequent presentation of the child to the doctor and elevated worrying about their child’s health (Aziz et al., 2018; Lockhart, 2016; Thorgaard et al., 2017a). A qualitative study by Ingeman and colleagues (2024) explored parents’ perceptions and found three core themes: 1. Feelings of distress, which can include fear, shame and guilt. 2. Mistrust in others, including doubts about the child’s ability to report symptoms accurately, concerns about their partner’s decision-making ability regarding the child’s health, and uncertainties about healthcare professionals' opinions. 3. Making sense of their worries with ambivalence in relation to worrying and rationalization of those sorrows. Health anxiety by proxy has already been discussed for pet owners (Nakano et al., 2019; Oxley and Kogan, 2018), but to our knowledge has not been considered for any other relationship types than the ones described above (parents or expectant mothers).
Health anxiety by proxy is not part of any diagnostic system although it has been considered for potential relevance (Rask et al., 2020). One current gap is that validated measures of health anxiety by proxy are lacking. Ingeman et al. (2021) newly introduced the Health Anxiety by Proxy Scale (HAPYS) with 26 items on parental worries on children’s health. So far, adapted versions of existing anxiety inventories have been used for assessing health anxiety by proxy in parent-child constellations, including the Illness Attitude Scale (Kellner, 1987) in the study by Thorgaard et al. (2017a) and the Short Health Anxiety Inventory (SHAI, Salkovskis et al., 2002) in Reiser and Wright’s study (2019). Other assessment approaches have been used for subtypes such as pregnancy-related anxiety (Bayrampour et al., 2016; Hadfield et al., 2022) or parental distress caused by web searches related to a child’s medical condition (Barke and Doering, 2020). To the best of our knowledge, there was no study to date that has assessed different relationship constellations of health anxiety by proxy simultaneously. It is unclear whether certain relationship types have elevated levels compared to other types and whether elevated proxy anxiety co-occurs across different types of relationships within the family.
Another important consideration is how health anxiety by proxy relates to family functioning and processes within the family unit (e.g., couple satisfaction, parental stress, and family functioning). Family Systems Theory describes the link between family well-being and general anxiety in the family (Kerr and Bowen, 1988). We extend this approach to examine indicators of family relationships (couple satisfaction, parental stress, and family functioning) and their association with health anxiety by proxy among parents. Since anxiety disorders tend to aggregate in families (Lawrence et al., 2019; Shimada-Sugimoto et al., 2015; Telman et al., 2018), we expect a degree of co-occurrence in health anxiety across ties (i.e. parent-child, parent-parent) along with impairment in family well-being.
Our aim was first to compare the health anxiety and health anxiety by proxy inventories – a partner-to-partner version and a parent-to-child version by examining mean and item level differences in anxiety. We hypothesized the highest level of health anxiety in relation to one’s own child when compared to self or partner. A second aim was to verify the factor structure of the health anxiety by proxy inventories. We assumed that each of the three questionnaires would form distinct factors. The third aim was to examine the relationship between health anxiety, health anxiety by proxy and family well-being. We expected strong positive correlations among the different health anxiety types. Furthermore, small to medium positive associations of health anxiety by proxy with couple dissatisfaction and poor family functioning were hypothesized based on past literature which documents associations between general anxiety and family constructs.
Method
Procedure
An online survey was conducted after ethical approval was obtained by the Ethics Council of the University on June 21st, 2020 (approval number: 2018-116). Recruitment lasted during a 6-week period between June 29th to August 9th, 2020. The study took place during the SARS-CoV-2 pandemic, a time characterized by globally heightened prevalence of anxiety symptoms (da Silva et al., 2021). At the time of data collection, Germany and Austria experienced relative stability, with regulations being relaxed and low infection numbers (Austrian Agency for Health and Food Safety, 2024; Robert Koch Institute, 2020).
Facebook groups and message boards with topics related to parenting, leisure activities or lifestyle were targeted for recruitment. In addition, we advertised on Instagram and Facebook for German-speaking parents between the age of 18 to 40 years as the target. Analysis of the HTTP referer revealed that 52.04% (n = 305) of the participants in the final sample reached the survey via Facebook. We also emailed more than 4000 kindergartens in Germany, Austria and Switzerland, asking them to share our call for participation.
Informed consent was obtained before data were collected. For eligibility, participants had to be at least 18 years old, parent of at least one child between the age of 0 and 6 years and had to be in an intimate relationship. The inclusion of parents with children between 0 and 6 years is based on the understanding that caregivers’ level of health anxiety may vary as children reach the developmental stage where they can effectively communicate their health complaints in a more detailed manner. To ensure that pre-existing illnesses do not influence the health anxiety levels under investigation, we implemented exclusion criteria that involved individuals, their partners, and their children having either chronic or acute diseases. By employing these criteria, we aimed to eliminate any potential confounding factors associated with existing health conditions. As an incentive, we offered the chance to receive one of 10 gift vouchers.
Participants
Sociodemographic characteristics of participants.
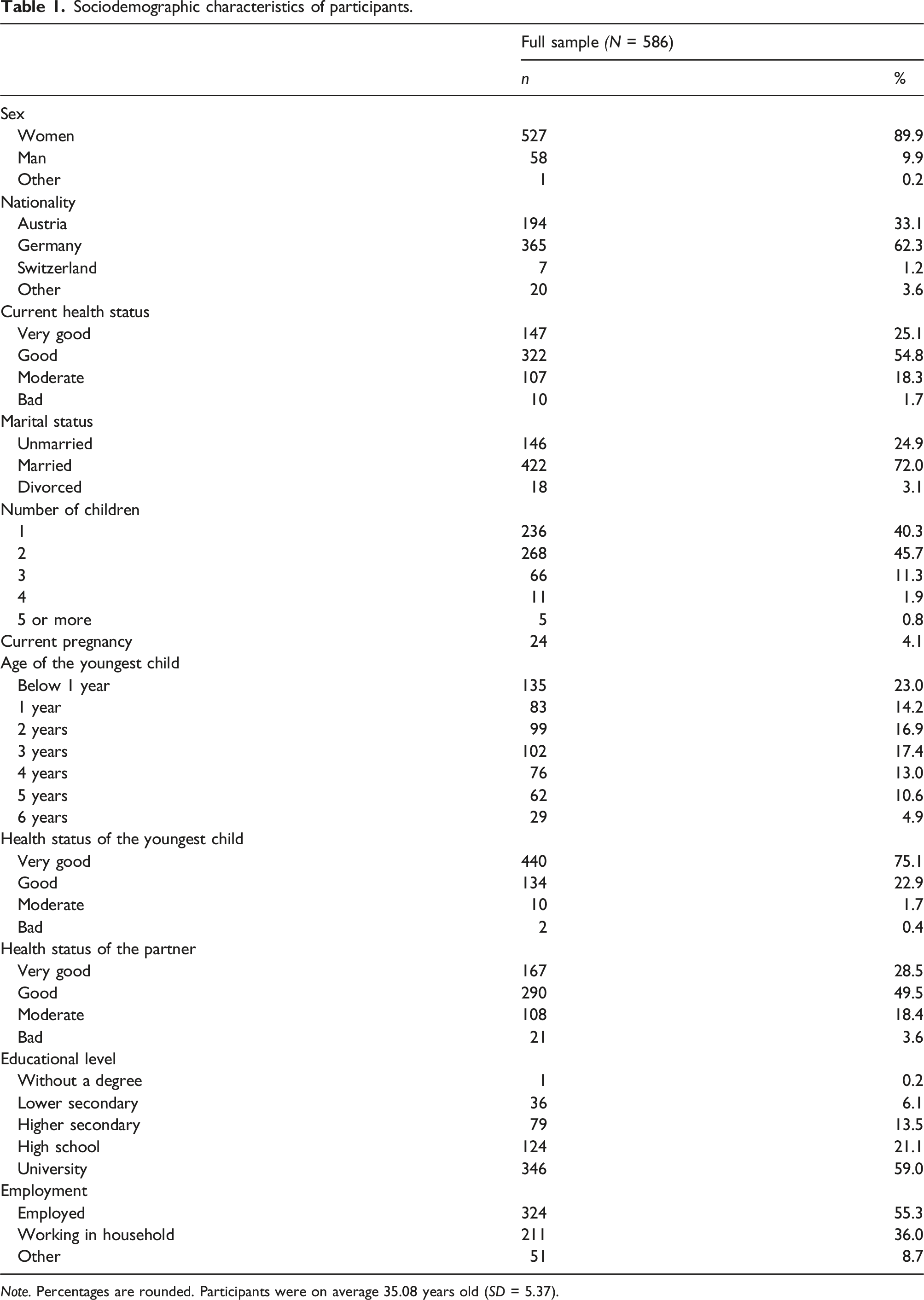
Note. Percentages are rounded. Participants were on average 35.08 years old (SD = 5.37).
Data cleaning
The data set of 1526 entries was cleaned in four waves. First, 718 participants were excluded because they provided only demographic data, but did not continue the survey. Second, 128 participants dropped out because the information on at least one of the three anxiety questionnaires was missing. Third, 92 participants were excluded because they did not have a child between 0 and 6. Lastly, two participants were excluded because the response pattern did not seem plausible (e.g., all items endorsed at the extreme end or no items endorsed). This resulted in a sample of 586 eligible parents.
Measures
Demographics
The demographic characteristics of the participants that were collected included gender, age, nationality, occupation, marital status, health status and education. Further, we assessed length of relationship in years, age of the youngest child (categorized into below 1 year, 1 year, 2 years, 3 years, 4 years, 5 years, 6 years), sex of the youngest child, health status of the child, household size, total number of children, current pregnancy and health status of the partner.
The modified Short Health Anxiety Inventory
The German translation of the Modified Short Health Anxiety Inventory (mSHAI) by Bailer and colleagues (2013) is a self-rating scale of health anxiety and includes 14 items, each rated on 0 to 4. The inventory was originally published by Salkovskis et al. (2002) as Short Health Anxiety Inventory (SHAI) with a more elaborated response format and an additional subscale on perceived negative consequences. Individuals rate their level of trait health anxiety according to the past 6 months. Total scores range between 0 and 56. A higher score indicates higher levels of health anxiety. The scale is intended to measure health anxiety as a one-factor and continuous trait (Bailer and Witthöft, 2006). A meta-analysis has shown that the SHAI is a psychometrically strong instrument for assessing health anxiety (Alberts et al., 2013). In this sample, Cronbach’s α of the mSHAI was excellent (α = 0.94).
The modified Short Health Anxiety Inventory for Child
The modified Short Health Anxiety by Proxy Inventory for Child (mSHAI-Child) was designed to assess health anxiety by proxy regarding the own child. Each of the 14 original items of the mSHAI by Bailer et al. (2013) was reformulated to comply with the parent-child situation. For example, “I spend much of my time worrying about my health” was reformulated to “I spend much of my time worrying about my child’s health”. Answers were scored from 0 to four resulting in a score range of 0 to 56. Higher scores indicate higher levels of health anxiety by proxy towards the child. The mSHAI-Child showed excellent internal consistency in our sample (α = 0.93).
The modified Short Health Anxiety by Proxy Inventory for Partner
The modified Short Health Anxiety by Proxy Inventory for Partner (mSHAI-Partner) is derived from the 14 items of mSHAI by Bailer et al. (2013) to measure health anxiety by proxy concerning the intimate partner. Items were adapted to relate to partner’s health instead, for example “My family/friends would say I worry too much about my health” was reformulated to “My family/friends would say I worry too much about my partner’s health”. Possible scoring within 0 to 56 points, with higher scores reflecting higher levels of health anxiety by proxy towards the intimate partner. The internal consistency in the current sample was excellent (α = 0.94).
Couple Satisfaction Inventory
The Couple Satisfaction Inventory (CSI) by Funk and Rogge (2007) is a self-report measure for assessing relationship satisfaction in couples. The original version consists of 32 items, however, a shorter version with 16 items (CSI-16) demonstrated similar psychometric properties (Funk and Rogge, 2007). We used the German translation by Treffner and Foran (2017). Participants can score between the range 0 to 81. Higher scores indicated higher couple satisfaction. Scoring below 51.5 indicates substantial relationship dissatisfaction. The inventory was found to be highly reliable in our sample (α = .97).
Parenting Stress Scale
The Parental Stress Scale (PSS) by Berry and Jones (1995) is an assessment for measuring stress that results from having a child. Parents rate on 18 items different aspects of the parent-child relationship (e.g. satisfaction of being a parent). Scores can range from 18 to 90. A higher score indicates a higher level of parental stress. Cronbach’s coefficient of the PSS in this study was good (α = 0.86).
General Functioning Scale
The General Functioning Scale (GFS, Byles et al., 1988) is an extracted 12-item subscale of the McMaster Family Assessment Device (FAD, Epstein et al., 1983) to assess overall functioning in families. Each item is evaluated on a four-point Likert scale with scoring from one to 4. The sum of scores is divided by the number of items for calculating the average score. A score of one indicates healthy family functioning, while four represents extremely poor family functioning. In our sample, the GFS demonstrated good internal consistency (α = 0.87).
Data analytic strategy
IBM SPSS version 25 was used for data analysis. For hypothesis 1, nonparametric Friedman tests were carried out to compare the three health anxiety conditions at the overall and individual item level. Additionally, an independent sample t test was conducted for comparison between health anxiety towards self and health anxiety towards child. Regarding hypothesis 2, the factor structure of the mSHAI, mSHAI-Child and mSHAI-Partner was analyzed with an exploratory factor analysis (EFA). For hypothesis 3, correlations between health anxiety inventories and family variables (i.e. family functioning, couple satisfaction, parental stress) were examined.
Results
Preliminary analysis
Descriptives for health anxiety inventories and family functioning scales.

Note. N = 586. mSHAI = modified Short Health Anxiety Inventory; mSHAI-Child = modified Short Health Anxiety Inventory For Child; mSHAI-Partner = modified Short Health Anxiety Inventory For Partner; CSI-16 = Couple Satisfaction Index; PSS = Parenting Stress Scale; GFS = General Functioning Scale.
Individual item comparison for each health anxiety scale.

Note. N = 586. * Friedman test. mSHAI = modified Short Health Anxiety Inventory; mSHAI-C = modified Short Health Anxiety Inventory For Child; mSHAI-P = modified Short Health Anxiety Inventory For Partner.
Mothers scored significantly higher on health anxiety (mSHAI) than fathers (Welch’s t-test, t (85.21) = 2.70, p = .008). There were no statistically significant differences between mothers and fathers for health anxiety regarding the child, (t (583) = 1.00, p = .31) or for health anxiety towards the partner, (t (583) = 0.74, p = .45). Further, we asked parents with more than one child (n = 350) whether they would have answered the questions about the mSHAI-Child differently if it were not related to their youngest only but to all children. Only 12.1% (41/340) stated that they would have answered differently.
Factor structure of the mSHAI, mSHAI-Child and mSHAI-Partner
Exploratory factor analysis of health anxiety items.
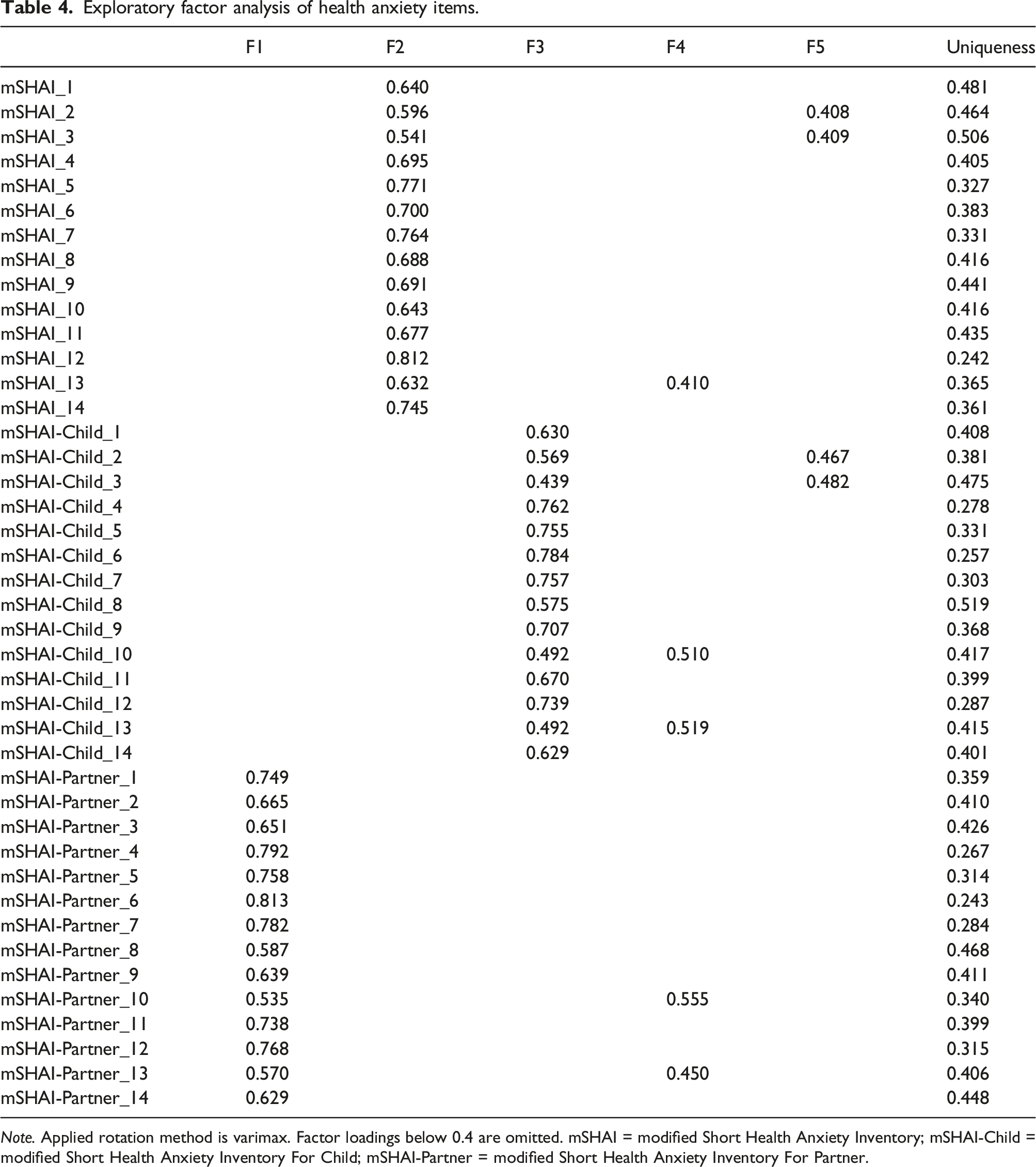
Note. Applied rotation method is varimax. Factor loadings below 0.4 are omitted. mSHAI = modified Short Health Anxiety Inventory; mSHAI-Child = modified Short Health Anxiety Inventory For Child; mSHAI-Partner = modified Short Health Anxiety Inventory For Partner.
Each item of the respective questionnaires (mSHAI, mSHAI-C, mSHAI-P) loaded sufficiently on a separate factor without cross loadings (>0.40), resulting in three definable factors. However, all items in relation to bodily sensations had cross-loadings on factor 4 or factor 5. This includes noticing aches/pain (item two in mSHAI and mSHAI-C), attention to bodily sensations (item three in mSHAI and mSHAI-C), wonder what bodily changes mean (item 10 in mSHAI-C and mSHAI-P) and unexplained bodily sensations (item 13 in mSHAI, mSHAI-C and mSHAI-P).
Correlations of health anxiety with family variables
Correlations for health anxiety measures, family variables and stress inventories.

Note. Pearson-Correlation for all variables, except age of youngest child with Spearman’s ρ. mSHAI = modified Short Health Anxiety Inventory; mSHAI-Child = modified Short Health Anxiety Inventory For Child; mSHAI-Partner = modified Short Health Anxiety Inventory For Partner; CSI-16 = Couple Satisfaction Index; PSS = Parenting Stress Scale; GFS = General Functioning Scale.
*p < .05,
**p < .01.
Further, small negative associations with relationship duration were found for all health anxiety inventories (r = −.12 to r = −0.15), indicating lower levels of health anxiety in longer existing relationships. Parenting stress and family functioning had small positive correlations with all health anxiety inventories (r = 0.15 to r = 0.20). Couple satisfaction was negatively correlated with mSHAI (r = −0.14, p < .001) and mSHAI-Child (r = −0.13, p = .003) but did not reach significance towards mSHAI-Partner (r = −0.08, p = .05).
Discussion
Based on our findings, we found support that health anxiety and health anxiety by proxy should be assessed independently and evaluated further to understand health anxiety in relation to family processes. There were significant mean differences between the inventories. Despite women having significantly higher health anxiety scores for themselves, there were no gender differences in the health anxiety by proxy conditions.
Health anxiety, its relation to health anxiety by proxy and its measurement
Our results confirm previous findings on the strong relationship between health anxiety and health anxiety by proxy (Thorgaard et al., 2017a; Reiser and Wright, 2019), suggesting closeness between both constructs. However, we found noteworthy differences between health anxiety for self and by proxy. We observed distinct latent factors in the exploratory factor analysis for health anxiety regarding self, child and partner. Established screening instruments like the Health Anxiety Inventory (HAI) or Whiteley-Index (WI) may not be suitable to presort or screen those who may be affected by health anxiety by proxy. Further questions of conceptualization of the measurement approach arise between the general conditions (health anxiety vs health anxiety by proxy) as well as within the several health anxiety questionnaires (mSHAI vs mSHAI-C vs mSHAI-P). Especially the factor structure of both introduced health anxiety by proxy measures should be investigated in future studies due to inconsistent results in past research with the original SHAI/mSHAI. While the German mSHAI is intended as one-dimensional (Bailer et al., 2013), the rarely used 14 item version of the SHAI was found to be two-dimensional (Alberts et al., 2011). Of note, the comparable validation study of the health anxiety by proxy measure for pregnant women by Reiser and Wright (2019) proposed their adaption of the SHAI as a unitary scale; however, their EFA resulted in a two-factor solution with “illness likelihood” and “body vigilance”. Therefore, the present study may add further evidence that health anxiety by proxy cannot be measured unidimensional with the adapted mSHAI questionnaires and that further validation studies are necessary to elucidate the factor structure.
In addition, the level of health anxiety regarding the child was significantly higher than parental health anxiety indicating the importance of health anxiety for the child as an area for further study. Research is also needed to understand first the clinical relevance of elevated health anxiety and its persistence through different conditions (i.e. towards self, child and partner) and second, the mutual impact in individuals with one elevated condition and the relevance of increase or onset of further health anxiety conditions.
Associations of health anxiety by proxy with family variables
A recent review by Thorgaard and colleagues (2018) found that little research has been done on the influence of family factors on health anxiety. In our sample, parenting stress, couple dissatisfaction and poor family functioning had small correlations with health anxiety and proxy conditions. This is similar with findings in the literature on anxiety symptoms and family quality measures (Hughes et al., 2008; Rapee, 2012; Whisman et al., 2004) and indicates that worse family functioning covaries with anxiety. Further research is needed to evaluate the dynamics of family functioning and health anxiety across family forms.
Surprisingly, the number of children was not correlated with the mSHAI-Child, but lower age of the youngest child correlated with higher health anxiety by proxy as assessed with the mSHAI-Child. It may support the fact, that uncertainty plays a major role in maintaining health-related worries towards the child (Carleton 2012; Fergus and Bardeen, 2013), while gained experience has less impact (e.g., experiences with various health conditions of older siblings). On the contrary, only 12.1% of parents with more than one child stated that they would have answered differently in mSHAI-Child items if they would be related to another (i.e. older) child. Thus, there may be greater variability in parental health anxiety by proxy, but this could be examined further in subsequent studies.
Health anxiety by proxy in the family system
Considerable research has shown that anxiety disorders tend to aggregate in families (Lawrence et al., 2019; Shimada-Sugimoto et al., 2015; Telman et al., 2018). We recommend aligning parental health anxiety by proxy as a process within the family system rather than to individual’s impairment for the following reasons. First, health anxiety by proxy is based on relational interaction between at least two subjects and includes inevitably a significant other. According to social network theory (Smith and Christakis, 2008; Valente 2010), the health between two or more socially strongly tied individuals is interconnected and characterized by mutual impact on health-related variables. In contrast, health anxiety is defined as disproportionate concerns about one’s own health (American Psychiatric Association, 2013) without attention to health concerns for others specifically. Since several family members can be significantly involved in this dysfunctional health behavior, couple or family interventions should be considered. Second, health anxiety by proxy can have an impact on health and well-being outcomes of others (i.e. family members). Children of mothers with severe health anxiety were presented more often to the doctor (Thorgaard et al., 2017a, 2017b) and confronted with more negative illness perceptions (Thorgaard et al., 2017a), and thus at potential risk for developing unrealistic health beliefs.
In contrast to previous research, we extend the consideration of health anxiety by proxy towards the intimate partner. Elevated health anxiety by proxy was hypothesized to impair relationship quality and partnership based on past studies on anxiety disorders rather than health anxiety specifically (Kasalova et al., 2017; McLeod, 1994; Pankiewicz et al., 2012). In the current study, levels of health anxiety towards the partner were significantly lower than towards the child. We attribute the significant difference in our sample mainly to higher uncertainty tolerance (Strout et al., 2018) and less perceived responsibility for the partner’s health situation than for the child’s. Health anxiety towards the partner may play a much bigger role in later life when the partner’s health deteriorates or in a caring situation. High rates of anxiety were found among family caregivers across a variety of diseases or impairments (Denno et al., 2013; Mahoney et al., 2005; Sklenarova et al., 2015) and where, among others, fear of deterioration of partner’s health status was reported. This work on health anxiety by proxy adds to related work that borders in conceptualizations such as on caregiver anxiety or burden (Novack et al., 1991; Mahoney et al., 2005; Nabors et al., 2013), death anxiety (Adelbratt and Strang, 2000), interdependent anxiety (Segrin et al., 2007) and general anxiety. Consistent use of a common term could help in the future to better examine health anxiety by proxy.
Accordingly, we encourage researchers to investigate the dyadic interaction of parental health anxiety on the child, respectively the triad with mutual repercussions on health anxiety by proxy between mother, father, and child. Connecting to family systems theory (Kerr and Bowen, 1988), perceived anxiety can worsen emotional processes within the family unit, including relationship quality, communication, and stress. Consequently, health anxiety should not be treated as an isolated individual construct but relevant for models of families and health. Further work could also investigate the role of various forms of anxiety (health anxiety, health anxiety by proxy, generalized anxiety, etc.) and how they interact in combination on family functioning. This research could shed light on which types and severities of anxiety disorders are most detrimental to family climate and children’s development.
Implications for clinical practice and public health
Health-related anxiety disorders are often associated with intensive healthcare utilization, and thus, at high-cost for health care systems (Barsky et al., 2001; Fink et al., 2010). In the case of health anxiety by proxy, similar dysfunctional behavior patterns may occur, and result in increased need for health care utilization. Clinicians should take into general consideration that health anxiety by proxy can be a relevant issue for some groups such as parents and caregivers that are seen in clinical practice and health psychology settings and that high levels of health anxiety by proxy can occur regardless of one’s own health anxiety.
In the long term, treating parental anxiety by proxy could possibly prevent later developed anxiety disorder in the offspring, but this should be examined in future studies (Eley et al., 2015; Ramchandani et al., 2011; Thorgaard et al., 2017). Parents may play a major role in transgenerational transmission of health anxiety through maladaptive health beliefs and excessive reinforcement of health-related behaviors (Marshall et al., 2007; Köteles et al., 2015; Wright et al., 2017; Thorgaard et al., 2018). Therefore, additional assessment of not only general health anxiety but anxiety by proxy could be informative.
Implications for researchers
The findings on health anxiety by proxy are based on only a few empirical studies. To enhance the evidence, researchers should further investigate the connection between health anxiety and health anxiety by proxy. This can be achieved by cross-validating with other anxiety-related questionnaires, for example, general anxiety disorder, nosophobia, cyberchondria, or depression. Additionally, using questionnaires to assess maladaptive health-related behaviors would be beneficial in understanding the transition from typical parental concerns to harmful health anxiety by proxy. Moreover, it is plausible that essential core elements for assessing health anxiety by proxy have been inadvertently neglected during the adaptation of the mSHAI. To address this, researchers could consider conducting a comparative analysis with the recently published Health Anxiety by Proxy Scale developed by Ingeman et al. (2021). Future studies should also consider other potential vulnerable relationships for health anxiety by proxy, especially non-parent relationships, like pet owners, informal caregivers, or close friends.
Limitations
There are several limitations to mention. Our study was cross-sectional and thus, we cannot make any statements about causality. The questionnaires were tested and validated in a German-speaking sample. Cultural differences on socially accepted health-related behavior regarding child or partner could impact on total scoring. Although the survey took place during a steady phase of the COVID-19 pandemic in central Europe, influences on the level of health anxiety cannot be excluded. As a result, it is plausible that the average levels of health anxiety inventories in the sample may exhibit higher values than would typically be expected. Another limitation of our study relates to the potential presence of selection bias resulting from our recruitment strategy. Participants were primarily recruited from online parenting groups and may differ from individuals that are not active online; although the majority of parents now fall into the group of active online users. Additionally, the majority of the participants were high-educated mothers; therefore, further validation work with fathers and educationally disadvantaged individuals is necessary.
Conclusion
Our results suggest that health anxiety by proxy is worthy of further investigation and may be relevant for working with families. The mSHAI-Child and mSHAI-Partner seemed to be promising inventories for assessing health anxiety by proxy, and thus should be considered in future work. Studies are needed to evaluate the prevalence in the general population among different relationship types and further examine clinical relevance. In this study, health anxiety by proxy was associated with family well-being, which may be relevant for family interventions and psychoeducation addressing anxiety in families and health problems. These relationships should be explored further in prospective studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Office of Academic Affairs, University of Klagenfurt.
Availability of questionnaires
The questionnaires utilized in this study are available upon request from the corresponding author.