
Abstract
Disease severity, illness intrusiveness, and health locus of control (HLC) each contribute to psychosocial wellbeing in patients with congestive heart failure (CHF). To better understand the relationships between these variables regarding anxiety symptoms, we analyzed data from 116 adult male veterans with comorbid CHF and anxiety. Results suggested that illness intrusiveness significantly mediated the relation of CHF severity to anxiety symptom severity, and that the illness intrusiveness domains of physical well-being/diet, work/finances, and other aspects of life (religious/spirituality, community/civic, self-improvement/expression) were also significant mediators of that relationship. The relation of illness intrusiveness to anxiety was not moderated by internal HLC. Findings highlight the importance of assessing and treating various aspects of illness intrusiveness to manage anxiety symptoms in CHF patients.
Introduction
According to the American Heart Association, congestive heart failure (CHF) affects approximately 6.2 million adults in the United States and was mentioned on 379, 800 death certificates in 2018 (Virani et al., 2020). CHF occurs when one’s heart muscle does not pump blood as well as it should, causing fatigue, shortness of breath, and swelling in legs, ankles, and feet (Mayo Foundation for Medical Education and Research, 2013). In addition to healthcare burden, these symptoms affect physical functioning and mobility, and ultimately, patients’ mental health by reducing their quality of life and participation in daily life activities (Cully, et al., 2009a; MacMahon and Lip, 2002; Paukert et al., 2009).
Among patients with CHF, anxiety and depressive disorders are the most common psychiatric conditions, which often lead to further negative health and cardiovascular outcomes. (Celano et al., 2018). Approximately 13% of CHF patients meet diagnostic criteria for a formal anxiety disorder and almost 30% of patients endorse clinically significant levels of anxiety (Celano et al., 2018). Earlier studies have suggested that the prevalence of anxiety may be as high as 63%, depending on the CHF subgroup studied (Konstam et al., 2005). In patients with CHF, anxiety disorders are associated with adverse outcomes such as hospital readmission, greater health services use, and poorer health-related quality of life (Cully et al., 2009b; Volz et al., 2009).
Illness intrusiveness has been deemed a major influencing factor on quality of life in patients with chronic disease (Devins et al., 1994). Illness intrusiveness refers to the extent to which the person perceives that disease and treatment related factors interfere with engagement in daily life, including work and leisure activities. Research findings have shown that the intensity of illness symptoms and treatment effects are positively associated with psychological distress and reduced quality of life (Devins, 2010; MacMahon and Lip, 2002). However, among adults with chronic diseases, illness intrusiveness was positively associated with anxiety symptoms when controlling for illness severity, illness uncertainty, and social support (Bieling et al., 2001; Dancey and Friend, 2008; Paukert et al., 2009).
Theoretical models have proposed that the relation of disease (e.g., pain, fatigue, disability, etc.) and treatment factors (e.g., time required, amelioration of symptoms) to psychological wellbeing is mediated by illness intrusiveness (Devins et al., 2009; Roessler, 2004). It is hypothesized that illness intrusiveness produces negative psychological effects by reducing individuals’ ability to carry out valued experiences and activities and avoid negative ones. As described in this model, what directly affects individuals’ quality of life may not be the disease per se, but the sense of loss and lack of positive reinforcement that stems from the inability to participate in meaningful activities because of the disease. In addition, the illness intrusiveness framework suggests that personality, social, and contextual factors may moderate the relation between illness intrusiveness and subjective wellbeing (Devins et al., 2006; Synder et al., 2013).
Research findings have provided support for the mediating role of illness intrusiveness in the relation of disease factors and quality of life across a wide range of medical and psychiatric conditions (e.g., breast cancer, rheumatoid arthritis, multiple sclerosis, systemic lupus erythematous, hyperhidrosis, end-stage renal disease, laryngectomy, and sleep disorders) (Bettazzoni et al., 2008; Dancey and Friend, 2008; Devins et al., 1993a, 1993b, 1994; Paukert et al., 2009). However, the patient’s sense of personal control, or internal locus of control (LOC), is an important construct in the illness intrusiveness model that has not been widely studied.
LOC has been defined as the degree to which individuals typically expect that either their behaviors or factors outside of their control will lead to various outcomes (Ryon and Gleason, 2014). LOC captures a relatively stable personality predisposition of individuals to attribute events to either their own actions (internal LOC) or to factors outside of their control (e.g. fate, luck, or other people) (external LOC). An internal health locus of control (HLC) refers to individuals’ predisposing beliefs regarding the extent to which they are able to perform health-related behaviors (e.g. identify and select treatment options, manage symptoms, etc.) that will influence the course of their illness (Asadi-Pooya et al., 2007). For example, patients who believe that they can control aspects of their health are more likely to follow potentially demanding and complex medical recommendations; whereas patients who believe external factors control their health, are less likely to adhere to medical recommendations (Luszczynska and Schwarzer, 2005).
LOC also has been associated with mental health outcomes. In recent cross-sectional and longitudinal studies with adults, internal LOC was negatively associated with anxiety (Krampe et al., 2021; Sigurvinsdottir et al., 2020) and with general mental distress (Alat et al., 2021; Hovenkamp-Hermelink, 2019). Furthermore, early studies indicated that higher levels of internal LOC (Sandler and Lakey, 1982) and internal HLC (Hunter et al., 1984) buffered the association of negative life events to anxiety and psychological distress symptoms, respectively. More recently, Krampe et al. (2021) reported that during the early months of the COVID-19 pandemic, higher levels of internal LOC buffered the relationship between COVID-19 stress and general mental distress among community adults. Taken together, these findings suggest that HLC, conceptualized as a personality predisposition, may moderate the relationship between illness intrusiveness and anxiety symptom severity.
In summary, research findings suggest that in general disease severity, illness intrusiveness, and HLC, each contributes to overall psychosocial wellbeing in CHF patients (Bieling, et al., 2001; Cully et al., 2009a; Cully et al., 2009b; Dancey and Friend, 2008; Devins, 1991; Devins et al., 2006; Paukert et al., 2009; Poochikian-Sarkissan et al., 2008; Talbot et al., 1999). However, none of these studies examined the role of internal LOC in the illness intrusiveness model specific to Veterans diagnosed with comorbid CHF and anxiety. Additionally, to our knowledge, research that examines the association of each of the five illness intrusiveness domains (e.g., physical well-being/diet, work/finances, marriage/family, social/recreational, and other aspects of life including religious/spiritual, community/civic, or self-improvement/expression activities) to medical conditions is scarce. Understanding how each variable in this model relates specifically to anxiety can help clinicians further refine interventions to reduce illness intrusiveness and anxiety symptoms in patients with CHF and other chronic conditions. Therefore, the purpose of the current study was to examine among Veterans experiencing CHF: a) illness intrusiveness as a mediator of the relation between CHF severity and anxiety symptom severity, b) whether specific sub-constructs of illness intrusiveness are important in explaining the mediation effect, and c) to what extent higher levels of internal HLC buffered the relation between illness intrusiveness and anxiety symptom severity.
Methods
Participants
Participants were 116 adult male with CHF diagnoses from two US Veterans Affairs (VA) hospitals in the south-central United States (please see “Demographics” section below for further detail). Data for the current study were collected as a baseline screening for an ongoing trial of brief cognitive behavioral therapy (bCBT) for Veterans with CHF, chronic obstructive pulmonary disease (COPD), or both, and clinically significant symptoms of depression and/or anxiety (Cully et al., 2012). For the purposes of this study, only data from Veterans with comorbid CHF and anxiety was used. The parent’s study procedures were approved by the Baylor College of Medicine Institutional Review Board (H-27,082) and the VA Research and Development review committee. All participants provided informed consent including publication permission. The analysis and publication of the retrospectively obtained and anonymized data for this non-interventional study was approved by the University of Houston Institutional Review Board (15,208-EX - 5705).
Measures
Illness intrusiveness
The Heart Failure Illness Intrusiveness Rating Scale (HF IIRS; Devins et al., 1983; Devins, 2010) is a 13-item, self-report scale that measures patients’ perceptions regarding the extent to which CHF currently intrudes upon meaningful life activities (Cully et al., 2012; Devins et al., 1983). Example items include, “How much does your HF and/or its treatment interfere with your relationship and social activities with your family?” and “How much does your HF and/or its treatment interfere with your religious or spiritual activities?”). Respondents rated illness intrusiveness in a seven-point scale with higher scores indicating higher levels of illness intrusiveness. This measure includes the following domains: Physical Well-Being and Diet; Work and Finances; Marital, Sexual, and Family Relations; Recreation and Social Relationships; and Other Aspects of Life. The IIRS has demonstrated good to excellent internal consistency reliability, good test–retest reliability, and high construct and discriminant validity (Devins, 2010; Devins et al., 1990, 2006). In the current sample, the internal consistency score in the scale was good (0.87).
Disease severity
The Kansas City Cardiomyopathy Questionnaire-Physical Limitation Subscale (KCCQ-PLS) is a well-validated, disease-specific quality of life inventory that closely resembles the New York Heart Association (NYHA) classification system concepts (Green et al., 2000; Hejjaji et al., 2021). The PLS captures the physical deficits associated with CHF and its symptoms of fatigue and shortness of breath. The KCCQ-PLS includes six questions asking about activity limitations related to CHF symptoms (e.g., dressing oneself) over the previous 2 weeks. Items are rated on a scale (ranging from one to either six or 7) and are consistent with semi-structured interviews used to determine NYHA classification. Scores in the KCCQ- PLS are scaled from 0 to 100, with 0 denoting the worst and 100 the best possible health status. Therefore, higher scores in the PLS indicated lower heart disease severity. It has convergent validity with the NYHA classification system and the 6-min walk test (Green et al., 2000). Internal consistency reliability for scores in the KCCQ-PLS has been reported to be 0.84 (Creber et al., 2012). In this study, scores in the KCCQ-PLS demonstrated good internal consistency reliability (0.79).
Anxiety
The Beck Anxiety Inventory (BAI; Beck and Steer, 1990) is a 21-item measure of the severity of self-reported anxiety symptoms over the past week (ranging from 0 (not at all bothered) to 3 (severely bothered)), with total scores ranging from 0 to 63. Scores between 0 and 7 indicate minimal anxiety, scores between 8 and 15 indicate mild anxiety, scores between 16 and 25 indicate moderate anxiety, and scores ≥26 indicate severe anxiety. In the initial development of the scale, BAI scores showed excellent internal consistency and adequate test-retest reliability estimates of 0.92 and 0.75, respectively (Beck and Steer, 1990). However, based on current studies, coefficient alphas range from 0.83 to 0.95 and test-retest reliability estimates ranged from 0.35 to 0.83 (Ayala et al., 2005). In this study, the BAI demonstrated good internal consistency reliability (0.88).
Health locus of control
The internal HLC subscale of the Multidimensional Health Locus of Control, Form C (MHLC; Wallston et al., 1994) consists of six items, with scores ranging from 6 to 36 with higher scores indicating stronger internal control beliefs. Example items included: “If my condition worsens, it is my own behavior which determines how soon I will feel better again” and “The main thing which affects my condition is what I myself do.” The MHLC demonstrates adequate internal consistency reliability, test-retest reliability, and construct validity (Wallston et al., 1994). Generally, the scales are moderately reliable, with Cronbach alphas ranging from 0.60 to 0.75 and test-retest stability coefficients ranging from 0.60 to 0.70 across studies (Wallston, 2005). In the current sample, scores in the internal HLC subscale demonstrated good internal consistency reliability (0.78)
Statistical analyses
A preliminary analysis was conducted to examine the bivariate correlations of the variables included in the study. To examine the indirect effect of illness intrusiveness on the association between CHF severity and anxiety symptom severity, a simple mediation model was tested using a non-parametric, bias-corrected bootstrapping procedure using macros provided by Preacher and Hayes (2004). To determine that a mediation effect is present, the 95% confidence intervals produced in the SPSS output for the direct and indirect effects cannot include zero. Additionally, five separate mediation analyses were conducted using each of the five illness intrusiveness subscales to examine which subscales mediated the relation of CHF severity to anxiety symptom severity. A hierarchical multiple regression analysis was conducted to test the moderating effect of internal HLC on the relation of illness intrusiveness to anxiety symptom severity, controlling for patients’ age. All variables were centered at the mean, which reduces the likelihood of multicollinearity problems.
Results
Demographics
Demographic statistics of the 116 adult male veterans indicated a mean age of 66.18 years (range 49-88 years old; standard deviation (SD) = 8.70). In this sample, 65.5% were Caucasian, 25% were African American, 3.5% were Hispanic, and 6% were of other ethnicities. Approximately 63% of the participants were married, 33% separated, divorced, or widowed, and 10% were never married. In terms of education, 18% had a General Educational Development (GED) degree or less than a high school education, 17% were high school graduates, 49% had some college education, and 15.5% were college graduates.
Bivariate correlations
Means (M), standard deviations (SD), and intercorrelations for predictor and criterion variables.
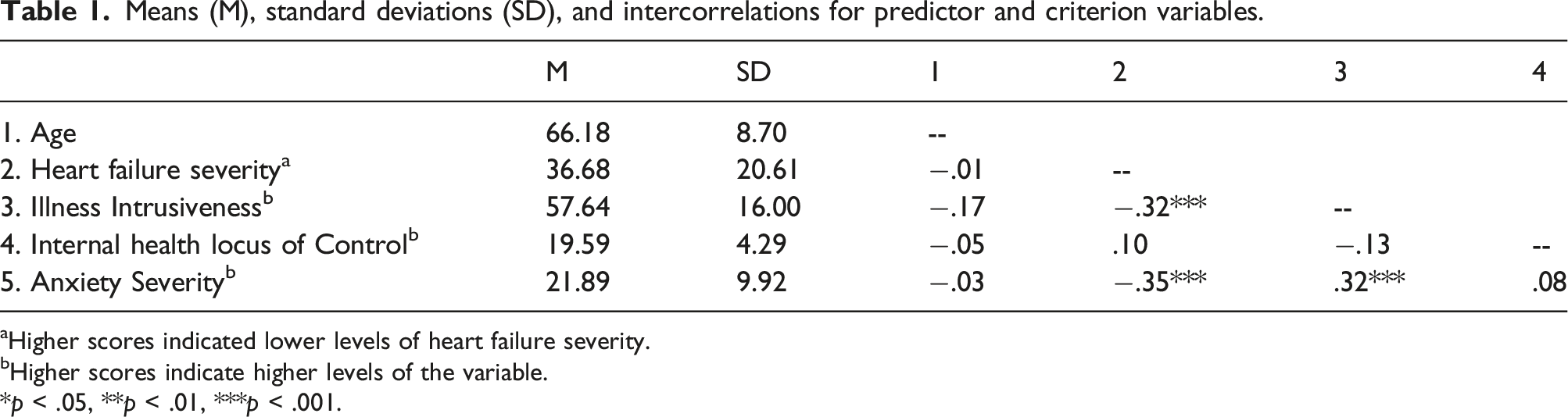
aHigher scores indicated lower levels of heart failure severity.
bHigher scores indicate higher levels of the variable.
*p < .05, **p < .01, ***p < .001.
Relations of illness intrusiveness, CHF severity and anxiety
Mediation results (see Figure 1) showed significant indirect effects for illness intrusiveness on the association between CHF severity and anxiety symptom severity (indirect effect estimate for illness intrusiveness = −0.038, SE = 0.018; 95% CI, −0.082 – (−0.01). Specifically, greater CHF severity was associated with greater illness intrusiveness (a path; β = −0.25, SE = 0.07, t = −3.52, p < .0001), and greater illness intrusiveness scores were associated with greater anxiety severity (b path; β = 0.15, SE = 0.06, t = 2.6, p < .01). In addition, results indicated a significant direct effect of CHF severity in relation to anxiety symptom severity, while adjusting for age (direct effect estimate (c’ path; β = −0.131, SE = 0.044, t = −2.95, p < .01; 95% CI, −0.219 – [-0.043]), meaning that greater CHF severity was positively associated with anxiety symptom severity. Results of a regression analysis indicated that the total effect of CHF severity on anxiety severity was significant as well (c path; β = −0.349, p < .001). Total (c path) and Indirect Effect (ab paths) of CHF Severity on Anxiety Symptom Severity Through Illness Intrusiveness. *p < .05, **p < .01, ***p < .001.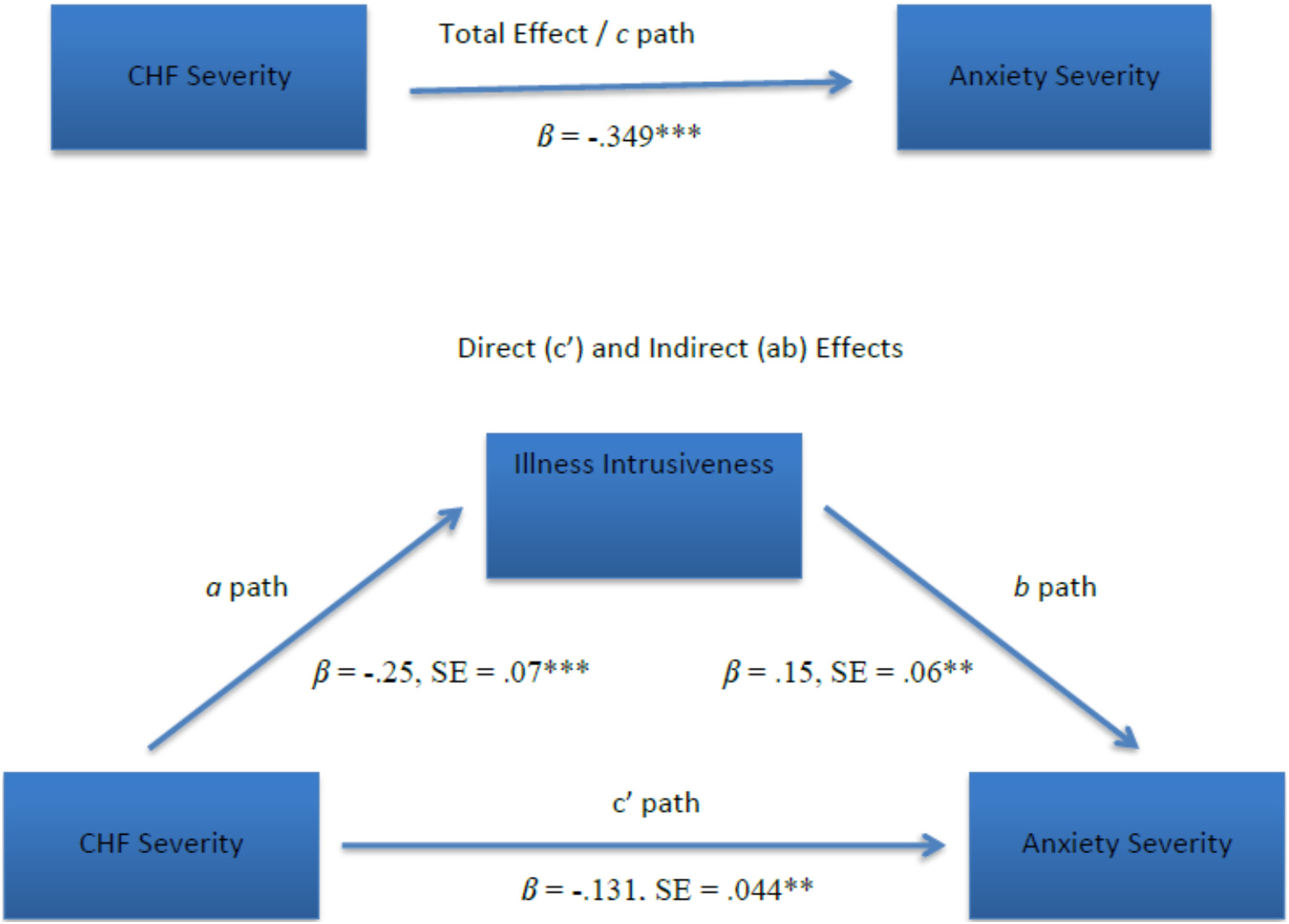
Further mediation analyses showed significant indirect effects for the physical, work, and other illness intrusiveness domains on the association between CHF severity and anxiety symptom severity (indirect effect estimate for illness intrusiveness – physical = −0.028, SE = 0.016; 95% CI, −0.071 – (−0.01); indirect effect estimate for illness intrusiveness –work = −0.033, SE = 0.018; 95% CI, −0.081 – (−0.005); indirect effect estimate for illness intrusiveness – other = −0.035, SE = 0.018; 95% CI, −0.086– (−0.008)). The indirect effect for the social/recreational and marriage/family domains were not statistically significant.
Relations of illness intrusiveness, internal HLC and anxiety
Hierarchical regression analysis summary for age, illness intrusiveness, and internal health locus of control, predicting anxiety symptom severity.

*p < .05, **p < .01, ***p < .001
Discussion
The purpose of the current study was to examine two components of the illness intrusiveness model in a sample of veterans diagnosed with comorbid CHF and anxiety. The study examined whether illness intrusiveness (total score and five domains) would mediate the relation of CHF severity to anxiety symptom severity, and if internal HLC would moderate the relation between illness intrusiveness to anxiety symptom severity. It was expected that the endorsement of a higher level of internal HLC might buffer the relationship between illness intrusiveness and anxiety, whereas the endorsement of a lower level of internal HLC may strengthen this relationship.
Consistent with our first hypothesis and with prior studies, results indicated that illness intrusiveness mediated the relationship between CHF severity and anxiety symptom severity (Devins et al., 1993a, 1993b; Devins et al., 1994). In other words, the extent to which patients perceived that CHF disease factors interfered with their engagement in daily life activities explained, at least in part, the relation of CHF severity to anxiety symptom severity. As LeMaire et al. (2012) discussed when interpreting similar results on depressive symptoms in patients diagnosed with CHF, the intrusiveness of CHF symptoms may be a better predictor of anxiety than the severity of the CHF symptoms themselves.
Additionally, results indicated that the three illness intrusiveness domains of physical well-being/diet, work/finances, and other aspects (e.g., religious/spiritual, community/civic, self-improvement/expression activities) also significantly mediated the relationship between CHF and anxiety severity. These findings suggest that these three domains may be most relevant in explaining the relation of CHF severity to anxiety severity. Further, there may be specific factors related to the intrusiveness of CHF symptoms in the domains of physical well-being/diet, work/finances, and other community/self-improvement activities that causes anxiety over and above the intrusiveness of CHF symptoms in the domains of marital/family and recreation/social relations. Perhaps the supportive aspects of marriage/family and social relationships serve as a buffer against how CHF severity affects anxiety severity; in fact, research shows that social support can be a means to improve health-related outcomes of patients with CHF as it facilitates self-care behaviors (Fivecoat et al., 2018; Graven and Grant, 2014; Salyer et al., 2012) and increases quality of life (Dehghani, 2018).
Due to the nature of CHF symptoms (e.g., shortness of breath, fatigue, etc.) and the limitations they may cause in one’s activity level, it makes sense that one’s physical well-being/diet and work/finances would be affected and thus, lead to increased anxiety. Many patients who are diagnosed with heart failure or experience a cardiac event undergo a significant change in their lifestyle, including having to change lifelong habits of physical activity and diet, and it is typically recommended that they engage in a cardiac rehabilitation program and take time off work to focus on their recovery. Changing old habits and forming new, healthier habits can be challenging for many and taking time off work can affect patients’ finances, role responsibilities, and quality of life; these patients may feel that their life meaning, and purpose has been taken away from them and experience feelings of loss and anxiety related to the future. Therefore, psychological interventions that address how to cope with these lifestyle changes and teach patients how to effectively manage their anxiety and other emotional responses are warranted.
Results did not provide support for the hypothesis that internal HLC would moderate the relation of illness intrusiveness to anxiety symptom severity. Studies have been mixed regarding how internal HLC is operationally defined and measured. In this study, internal HLC was operationalized from Rotter’s perspective as a personality predisposition to believe that one has control over the progress or outcomes of the disease. However, according to the illness intrusiveness framework, personal control refers to what extent illness and treatment related factors hamper patients’ sense of control over various domains of functioning or valued life activities. While the illness intrusiveness framework proposes that psychological factors may moderate the relation of illness intrusiveness to psychological wellbeing (Poochikian-Sarkissan et al., 2008; Talbot et al., 1999), in the current study a sense of personal control over health outcomes was not associated with anxiety symptoms nor moderated the relation of illness intrusiveness to anxiety symptoms. Previous studies have indicated that the association of internal LOC and psychological distress tends to be stronger for stressors perceived to be controllable than for those perceived to be uncontrollable (Papanikolaou et al., 2013; Peacock & Wong, 1996). It is possible that patients who experience CHF do not perceive their CHF’s symptoms and related intrusiveness as controllable stressors, which may explain the study’s lack of findings regarding HLC.
If confirmed by future longitudinal studies, the identified mediational role of illness intrusiveness domains in the relation of illness severity and psychological wellbeing may have important clinical implications for individuals presenting with comorbid CHF and anxiety symptoms. Clinicians and other health professionals may improve CHF patients’ quality of life by helping them decrease the interference the illness has on their valued life activities. More specifically, clinicians can help CHF patients improve their skills to cope with disease-related changes in physical well-being/diet, work/finances, and other community and self-improvement activities, which may prevent or decrease anxiety (and other mental health) symptoms in this population and, ultimately, contribute to an improved quality of life.
Limitations and future directions
Although the findings of the current study add to the existing illness intrusiveness medical literature, results need to be interpreted considering the study’s limitations. First, mediation models are best applied to examine causal relations in longitudinal designs; thus, the correlational and cross-sectional nature of the data can preclude definitive conclusions about the direction of the mediation relationship. To better clarify this relationship, future research with a larger sample may examine the relative importance of the various domains of illness intrusiveness in explaining the relation of illness severity to psychological well-being. It may also be beneficial to explore which aspects of illness intrusiveness are more strongly associated with anxiety via a regression analysis; this information may help tailor the clinical intervention in the most relevant domains. Second, although the measures used are well-established instruments, they are not based on objective data. For instance, researchers might use more objective measures of anxiety and heart disease, such as stress hormones or ejection fraction, to further increase the accuracy of the findings regarding these constructs. Third, the sample consisted of all male veterans from two VA hospitals in the U.S. This serves as a threat to the external validity of the study since the results may not be generalizable to female Veterans or civilian populations, or even male veterans in other hospitals. Future investigations can further this area of research by including a larger sample of veterans with CHF and anxiety symptoms.
Conclusion
Results illustrate the importance of assessing and treating illness intrusiveness to ultimately reduce or prevent anxiety symptoms in patients with CHF. For patients whose CHF interferes with their daily life activities, this intrusiveness might influence the relationship between their level of CHF severity and the amount of anxiety symptoms they experience. Further research on the illness intrusiveness theoretical model in more samples of patients with CHF will allow mental health and medical professionals to appropriately assess and treat patients diagnosed with CHF.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.