
Abstract
Benefit finding (BF) may be a coping strategy that positively influences outcomes after a stressful event, but previous studies provide an inconsistent pattern of results across several different patient populations. This study aimed to reconcile these inconsistencies by testing whether positive affect related to a cardiac event (PA) mediates the relationship between BF and healthy dietary behaviors, and whether this mediating relationship is stronger for participants high in disease severity. Participants were patients with cardiovascular disease in a cardiac rehabilitation program. Results supported partial mediation, but the interaction was not as predicted: participants low in disease severity showed a stronger relationship between BF and PA than their counterparts high in disease severity. Additionally, the PA/healthy dietary behaviors relationship was negative. Health providers may encourage patients in CR to engage in BF, but also to make thoughtful food decisions when in a positive mood, especially for patients low in disease severity.
Keywords
Introduction
After experiencing a stressful or potentially traumatic event, individuals may attempt to create meaning or find benefits from the experience (Taylor, 1983). Benefit finding (BF) has been described as a coping strategy in which individuals identify benefits in adversity, or stressful events, that may positively influence psychological and physical health outcomes (Pascoe and Edvardsson, 2013). BF is conceptually similar to perceived growth, or posttraumatic growth, as individuals may experience positive changes resulting from stressful experiences (Park et al., 2009). Researchers have used various terms to describe positive changes resulting from potentially traumatic events, such as posttraumatic growth or stress-related growth (Helgeson et al., 2006). Individuals experiencing BF may report coping better with stress and problems or being able to take things as they come (Tomich and Helgeson, 2006). Specific areas of growth include but may not be limited to spiritual growth, improved relationships, new possibilities, personal strength, and appreciation for life (Calhoun and Tedeschi, 2004). Currently, BF researchers disagree on whether BF reflects actual growth or perceived positive changes (e.g., Littlewood et al., 2008; Park et al., 2009; Tedeschi and Calhoun, 2004).
Furthermore, resiliency differs from BF in that the former focuses on adapting and adjusting to adversity while beliefs about the self, others, and the world remain unchanged as one simply bounces back (Elam and Taku, 2022; Yao and Hsieh, 2019). Resiliency may or may not involve a struggle, while BF always involves a struggle following adversity, which means one may experience both BF and resiliency at once. Positive reappraisal consists of evaluating and labelling potentially threatening situations in a positive way instead of labelling or evaluating them as threats or challenges (Riepenhausen et al., 2022). BF does not involve reappraisals, rather one identifies benefits in a stressful life event, which involves less effort than positive reappraisal. Similar to BF, positive reappraisal has been found to be related to resiliency (Sears et al., 2003).
BF may protect against the effects of stress on psychological and physical health outcomes in a few ways. It may help individuals adjust to stressful events via self-enhancement, meaning creation, and regaining control as proposed by the theory of cognitive adaptation (Taylor, 1983). Self-enhancement is a process through which one compares themselves to individuals worse off in similar situations in order to increase one’s self-esteem, and identifies positive benefits or changes resulting from the event (Taylor et al., 1984). Creating meaning out of the stressful event may also help restore a sense of mastery, or control over one’s situation and life (Taylor, 1983). Increased mastery can be a catalyst to find positive changes that contribute to a healthy lifestyle. Specifically, BF may act as a buffer to minimize the effects of stress on health outcomes (Helgeson et al., 2006) through increasing self-esteem. Although BF may develop through distress-related illness, it may continue to help individuals cope with negative affective reactions in the long term (Tran et al., 2011). Overall, BF may be a protective factor against stress both in healthy individuals exposed to potentially traumatic events and in those with existing illness.
BF and cardiovascular disease (CVD)
CVD is a group of disorders of the heart and blood vessels that can cause myocardial infarctions (i.e., heart attacks; MIs), stroke, blood clots, or a build-up of fatty deposits in an artery that lead to hardening and narrowing of said artery (i.e., atherosclerosis; National Health Service inform, 2022; World Health Organization, 2017). CVD is the leading cause of death globally (World Health Organization, 2017). CVDs include coronary heart disease, which affects blood vessels that supply the heart muscle; peripheral arterial disease, which affects blood vessels that supply the arms and legs; and cerebrovascular disease, which affects blood vessels that supply the brain. Most forms of CVD are preventable by modifying risk factors such as tobacco use, unhealthy diet, obesity, physical inactivity, and abuse of alcohol. For example, a meta-analysis of patients with coronary artery disease, a type of CVD, showed that those with the largest improvements in diet, including increased intake of vegetables, fruits, nuts, legumes, and fish, showed a 49% decrease in all-cause mortality rate compared to those with the lowest quality diet (Iestra et al., 2005). Therefore, healthy lifestyle changes, including dietary ones, are beneficial for patients with CVD during their recovery. Cardiac rehabilitation (CR) is a comprehensive secondary prevention strategy that helps decrease the risks of re-experiencing a cardiac event by modifying nutritional and behavioral risk factors (Braverman, 2011). Patients in CR in the U.S. typically participate in 36 outpatient sessions over 12 weeks that include physical activity, counseling to manage everyday stress, and educational programs to learn to manage risk factors such as unhealthy diet (American Heart Association, 2016). A retrospective study conducted in the U.S. found a 45%–47% decrease in 5-year mortality from 1994 to 2008 in patients who participated in CR compared to patients who did not (Goel et al., 2011). Despite CVD’s prevalence globally, sparse research has examined BF in the context of patients with CVD, with only three studies among patients enrolled in CR.
In one study, Sanjuán et al. (2017) validated the Spanish-translated version of the Benefit Finding Scale (Antoni et al., 2001) using a prospective study of patients with CVD enrolled in a CR program in Spain. They found that baseline levels of BF were positively associated with positive affect, self-efficacy, and social support concurrently and at 8 weeks follow-up. Affleck et al. (1987) found that patients who engaged in BF following their first MI were less likely to experience a second MI 7 years later, and they had decreased mortality rates compared to their counterparts who did not engage in BF. A third study by Javed and Dawood (2016) surveyed patients following an MI and found that posttraumatic growth was positively associated with perceived social support, problem-focused coping, active emotional coping, extraversion, agreeableness, conscientiousness, and openness to experience.
BF and other health outcomes
Past research examining associations between BF and health outcomes has yielded mixed results within a variety of non-CVD patient populations including HIV, diabetes, and renal disease (De Vries et al., 2019; Littlewood et al., 2008; Tran et al., 2011). For example, BF has been found to be negatively related to symptoms of distress including negative affect, depression, and stress (De Vries et al., 2019; Littlewood et al., 2008; Tran et al., 2011), but unrelated to medication adherence, blood sugar levels, and substance use. In their meta-analysis, Helgeson et al. (2006) found that BF was negatively related to symptoms of depression and positively related to well-being, but in other studies BF was unrelated to depressive symptoms or well-being (Park and Helgeson, 2006; Pascoe and Edvardsson, 2013).
Time as a potential moderator
The inconsistent results between BF and health outcomes in non-CVD patient populations may be unraveled by examining these associations over time. Research suggests that BF may have positive effects when more time has passed since a potentially traumatic event occurred because individuals have had time to cognitively process the event (Tedeschi and Calhoun, 2004). If BF is a coping process instead of a trait that remains stable over time, it is expected to change over time (Helgeson et al., 2006; Park et al., 2009; Zimmaro et al., 2020). In addition, individuals should perceive more benefits as time passes due to the meaning-making and adjustment processes involved when dealing with a potentially traumatic event. In fact, Helgeson et al. (2006) hypothesized that, cross-sectionally, BF may be a cognitive strategy to reduce distress, and is therefore related to poor health outcomes in the short term (i.e., subjective physical health), while longitudinally BF may be associated with improved health outcomes.
Positive affect as a potential mediator
The inconsistent results between BF and health outcomes in non-CVD patient populations may also signify that this relationship is mediated by another variable: positive affect (Bower et al., 2009). In fact, studies have shown consistent associations between BF, positive affect, and optimism. For example, Tran et al. (2011) reported positive associations between BF, positive affect, and coping effectiveness among a sample of adolescents with Type I diabetes. These associations among constructs have also been documented in samples with CVD (Hoen et al., 2013; Sanjuán et al., 2017). In these cases, positive affect may function as a protective psychological factor that may increase following a stressful event such as a cardiac event or CVD diagnosis (Boehm and Kubzansky, 2012; DuBois et al., 2015; Sin, 2016). For example, Davidson et al. (2010) found that an increase in positive affect was associated with a reduced risk of experiencing a cardiac event within 10 years among individuals who had never experienced a cardiac event at study baseline. Additionally, positive affect has been shown to be positively associated with a decreased risk of all-cause mortality among patients with coronary artery disease, even after controlling for symptoms of depression and disease severity (Hoen et al., 2013). Increases in positive affect may enhance the benefits of preventive strategies such as CR (Davidson et al., 2010).
Disease severity as possible moderator
In addition to the literature implicating positive affect as a possible mediator variable, our literature review yielded another possible moderator variable: disease severity. Tomich and Helgeson (2004) suggested that if BF has a positive association with quality of life, it may be more beneficial for patients with more severe disease. Therefore, they argued that stage of disease may be a moderator variable. However, in their study of patients with breast cancer, BF at 4 months post-cancer diagnosis was unrelated to positive affect, but was positively related to negative affect three and ninth months later. In fact, those diagnosed with Stage II breast cancer reported higher levels of BF and higher levels of negative affect than those diagnosed with Stage I cancer as time elapsed, also supporting the moderating effect of time. In other words, patients diagnosed with higher stages of breast cancer, or increased disease severity, reported higher levels of BF and negative affect. In contrast to these findings, cross-sectional and prospective meta-analytic research has found a positive relationship between BF, positive affect, and optimism (Helgeson et al., 2006; Pascoe and Edvardsson, 2013).
Objective
Based on the literature reviewed, this study sought to fill gaps in our understanding about relationships between BF, positive affect, and one type of health outcome, healthy dietary behaviors, in patients with CVD in a CR program. Since theory predicts and research has found that BF tends to increase over time (e.g., Helgeson et al., 2006; Park et al., 2009; Zimmaro et al., 2020), Hypothesis #1 predicted that mean levels of BF would increase from the start of CR (i.e., Time 1) to the end of CR approximately 12 weeks later (i.e., Time 2). We also predicted (Hypothesis #2) that positive affect would mediate the relationship between BF and healthy dietary behaviors (Davidson et al., 2010). That is, we predicted that Time 1 BF would be positively related to Time 1 positive affect, which in turn would positively predict healthy dietary behaviors at Time 2. We predicted that this mediating relationship would be qualified by a moderation effect: disease severity would moderate the relationship between BF and positive affect (Tomich and Helgeson, 2004). We used risk stratification for disease progression as a measure of disease severity. Specifically, we predicted that the positive relationship between BF and positive affect would be stronger for participants at high and intermediate levels of risk stratification compared to those low in risk stratification.
Method
Participants and procedure
Participants were recruited by hospital staff as part of a larger, ongoing study at a CR program in a Midwestern hospital. The hospital in which the CR program is held is a safety-net hospital (SNH). SNHs serve the most vulnerable individuals in the community by offering healthcare to all, regardless of ability to pay (Popescu et al., 2019). This results in a large percentage of people of color, low income, and uninsured patients being served, compared to non-SNHs. Participants consisted of English-speaking patients 18 years or older who had recently experienced a diagnosis of CVD and were enrolled in the study at the start of their participation in the CR program. Among the 240 individuals who were invited to participate in the study, 78 declined for the following reasons: 57 were not interested, 14 due to a language barrier, four said the questionnaire was too long, two were unsure they would participate in the CR program, and one did not give a reason. This resulted in a 67.5% participation rate among those who were invited to take part in the study, with a total sample of 162 participants at Time 1. Follow-up data at Time 2 were collected from 96 of these participants, yielding an attrition rate of 41%. Therefore, the final sample size consisted of 96 participants for whom Time 1 and Time 2 data were available.
Descriptive statistics of participant characteristics (N = 96).

Note: CR = cardiac rehabilitation; BF = benefit finding.
At Time 2, at the end of CR, participants attended a final graduation session in which they were asked to complete the questionnaire a second time. Once again, they were given time to complete the questionnaire in a private office at the CR site. Data were again collected from participants’ EHRs. Those who completed the Time 2 questionnaire were compensated $10.
Measures
Demographic information, CR nurses’ evaluations of patients’ risk stratification for disease progression, and an eating pattern assessment were collected from participants’ EHRs. Self-reported measures in the questionnaire assessed BF and positive affect.
Demographics
The following demographic information was extracted from participants’ EHRs: age, biological sex, race/ethnicity, education level, and health insurance status. The questionnaire measured marital status, employment status, and annual income.
Risk stratification
Risk stratification for disease progression is an evaluation of a patient’s risk of disease progression, such as experiencing or re-experiencing a cardiac event based on modifiable (e.g., hypertension, diet, and exercise) and non-modifiable risk factors (e.g., age, biological sex, and family history; Singh and Zeltser, 2020). At Time 1, participants were categorized by CR staff as “low,” intermediate,” or “high” in risk of disease progression within 10 years based on the American Association of Cardiovascular and Pulmonary Rehabilitation (2004) guidelines. In addition to focusing on risk factors, these guidelines are also based on participants’ diagnoses and prior cardiac events. For data analyses purposes this variable was dichotomized by forming two groups, one low in risk stratification (n = 38), and another intermediate or high in risk stratification (n = 58). This categorization was decided upon as patients low in risk stratification may have been referred to CR due to angina (i.e., chest pain), which is not as severe as those intermediate or high in risk who were referred due to congestive heart failure, MI, or other more severe cardiac events. Additionally, our second hypothesis examined whether individuals at lower levels of risk of disease progression would report lower levels of BF compared to those at higher levels of risk stratification, based on risk factors, those at low risk would need to make comparatively fewer behavioral changes.
Benefit finding
The Benefit-Finding Scale (Tomich and Helgeson, 2006) consists of 14 items using a four-point rating scale (1 = Not at all; 4 = Very much) that were summed to calculate a total score, with higher scores indicating higher levels of BF; possible scores range from 14 to 56. The wording was changed from “having had breast cancer…” to “having a cardiac event…” to reflect participants’ experiences. For example, participants responded to a question asking, “Having a cardiac event has made me more productive.” The instrument has not been previously used in a sample of patients with CVD, but the internal consistency was excellent when used in samples of patients with breast cancer (α = 0.95, α = 0.92; Tomich and Helgeson, 2004, 2006, respectively). In this study, the coefficient alphas were 0.92 and 0.94 at Time 1 and Time 2, respectively.
Positive affect
Four items from the Positive and Negative Affect Schedule (PANAS; Watson et al., 1988) were used to measure positive affect related to a cardiac event (PA). The four items asked how often a participant’s cardiac event made them feel the following forms of PA over the past 1 to 2 weeks: inspired, proud, excited, and determined. Response options are on a five-point scale (1 = Very slightly or not at all; 5 = Extremely), with higher scores indicating higher levels of PA related to the cardiac event; possible scores range from 4 to 20. The internal consistency of the full-version PA subscale was reported as excellent (α = 0.93) in a sample of patients with coronary artery disease (Hoen et al., 2013). In this study, the adapted PA subscale yielded an alpha coefficient of 0.83, which is within the acceptable range.
Dietary behaviors
The Rate Your Plate scale (RYP; Gans et al., 1993) measures dietary behaviors across 24 food categories. Participants report how often they make heart-healthy food choices across these 24 food categories, with higher scores indicating a more heart-healthy diet; scores can range from 23 to 69. When the RYP has been used for cholesterol-screening and in educational programs (i.e., CR), cholesterol levels and healthy diets improved (Gans et al., 1993, 2000). However, Cronbach’s alphas for the RYP were not provided in these studies. In this study, RYP total scores were obtained from EHRs, so Cronbach’s alphas could not be calculated.
Data analysis
The data were analyzed using IBM SPSS Statistics (Version 27) and the PROCESS macro (Hayes, 2013, 2020). Independent samples t-tests showed that there were no statistically significant differences on any study variables between participants who completed the questionnaire at both time points (n = 96) versus participants who did not complete the questionnaire at Time 2 (n = 66). Participants who did not complete the Time 2 questionnaire were excluded from all further data analyses. After ensuring that assumptions of normality were met, multiple imputation was used to impute missing values for demographic variables, BF, PA, and RYP at Times 1 and 2. In total, 0.65% of cases were imputed. A paired-samples t test was conducted to determine whether BF at Time 2 was higher than BF at Time 1 (i.e., Hypothesis #1). For Hypothesis #2, the mediation model was first tested using Hayes’ Model 4, then the moderated mediation model was tested using Hayes’ Model 8. Both moderated mediation and mediation models used 5000 bootstrap samples. We used 0.05 as the alpha level for null-hypothesis significance testing (Cohen, 1992).
Results
Sample characteristics
Participant characteristics are shown in Table 1. The sample consisted of 58 males (60.4%), 60.4% of participants were not employed outside the home (n = 58), and the median annual household income was $10,000 to $19,999 a year. Participants ranged in age from 36 to 73 years old. About 18% of participants did not have any form of health insurance, while 16.7% without traditional forms of health insurance utilized the hospital’s discount program. The highest education level achieved varied widely: 57.3% completed or attended some high school or received a GED, 27.1% attended some college or trade school, and 15.6% received a two-year, four-year, or graduate college degree. Fifty-one participants (53.1%) identified as White and the remainder identified as Black/African American (43.8%), Hispanic/Latino (1%), or other or mixed race/ethnicity (2.1%). Marital status was dichotomized, with 39.6% reporting being partnered. The total number of CR sessions completed ranged from 27 to 36, with 57 individuals (59.4%) completing all 36 available sessions.
Correlations between all study variables (N = 96).

Note: BF = benefit finding; T1 = Time 1; T2 = Time 2; RYP = Rate Your Plate; PA = positive affect. *p < .05. **p < .01.
Covariates
To test for potential covariates in the moderated mediation models, we ran independent samples t-tests and bivariate correlations. These included demographic variables such as age, biological sex, race/ethnicity, marital status, and insurance status. Results showed that participants who were partnered had a higher mean RYP at Time 2 (M = 54.47, SD = 8.11) compared to their counterparts who were not partnered (M = 50.25, SD = 9.24; t [93] = 2.29, p = 0.02). Education and income were also positively related to Time 2 RYP (r = 0.31, p = 0.002 and r = 0.37, p < 0.001, respectively).
Hypothesis one
The paired-samples t test (t [95] = 2.10, p = 0.04) showed that BF increased from Time 1 (M = 40.33, SD = 9.72) to Time 2 (M = 42.12, SD = 10.07), supporting the first hypothesis.
Hypothesis two
Bootstrap confidence intervals (CIs) were used to determine whether the direct, indirect, and conditional indirect effects were statistically significant. Covariates of RYP at Time 2 consisted of marital status, education, annual income, and RYP at Time 1. The first mediation model showed that marital status was not significantly predictive of RYP at Time 2 (β = 0.10, p = 0.24), therefore, it was dropped as a covariate. The remaining three covariates were included in the hierarchical regression models for both mediation and moderated mediation.
Mediation
Model coefficients for hypothesis 2 mediation model and moderated mediation model (N = 96).
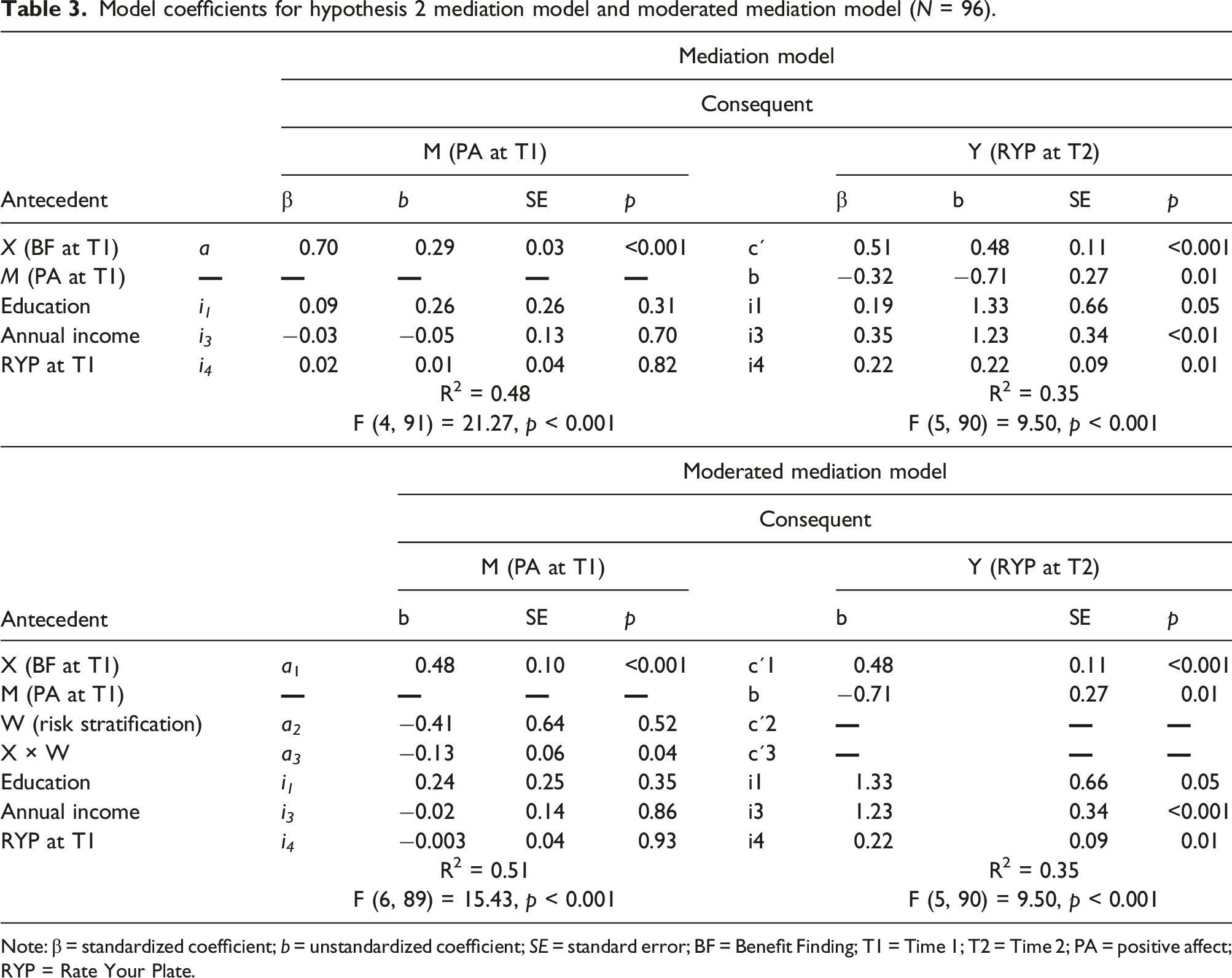
Note: β = standardized coefficient; b = unstandardized coefficient; SE = standard error; BF = Benefit Finding; T1 = Time 1; T2 = Time 2; PA = positive affect; RYP = Rate Your Plate.
Moderated mediation
Similar to the mediation model, direct effects for the moderated mediation model showed that BF at Time 1 was positively related to PA at Time 1 (see Table 3). In turn, PA at Time 1 was negatively related to RYP at Time 2. Additionally, BF at Time 1 was positively related to RYP at Time 2 while controlling for PA, risk stratification, and the three covariate variables (95% bootstrap CI [0.26, 0.71]). Of importance to this model, the interaction between BF and risk stratification predicting PA was statistically significant (F [1,89] = 4.23, p = 0.04). The upper and lower bounds of the bootstrap CIs for the conditional indirect effects did not include zero for participants at low (b = 0.35; 95% bootstrap CI [0.26, 0.44]) or intermediate/high risk for disease progression (b = 0.22; 95% bootstrap CI [0.13, 0.31]). However, these results only partially support Hypothesis #2. As depicted in Figure 1, participants who were classified as low in risk for disease progression had a steeper slope, or a stronger positive relationship, between BF and PA compared to their counterparts who were classified as intermediate or high in risk for disease progression. Thus, while all participants showed a positive correlation between BF and PA, it was stronger for those low in disease severity. Therefore, while we found a significant interaction, it was not in the direction predicted. In addition, we found partial mediation, but the direction of the relationship between PA and RYP was not as predicted (i.e., it was negative). Graph of interaction shown in moderated mediation hypothesis 2.
Discussion
The current study was conducted to gain insight into associations between BF and healthy dietary behaviors among patients with CVD enrolled in CR. Results supported the first hypothesis: levels of BF significantly increased from CR orientation to the end of CR. This finding aligns with predictions that individuals may need time to identify positive benefits following a potentially-traumatic event due to the possibly lengthy process of cognitive restructuring and rumination surrounding the event (Llewellyn et al., 2013). These results are consistent with past studies that have found increases in PTG/BF 10 years following lung transplantation (Fox et al., 2014), among men following an MI (Affleck et al., 1987), and among patients enrolled in CR diagnosed with CVD (Sanjuán et al., 2017).
The second hypothesis predicted that PA would mediate the relationship between BF and healthy dietary behaviors, and that the relationship between BF and PA would be qualified by an interaction with risk for disease progression. Results partially supported this hypothesis in two ways. First, the relationship between BF and dietary behaviors was only partially mediated by positive affect. Second, the strength of this mediating relationship differed based on participants’ classification of low versus intermediate/high in risk for disease progression (i.e., moderated mediation): participants who were categorized as low in risk for disease progression had a stronger, positive relationship between BF and PA compared to their counterparts high/intermediate in risk for disease progression. Therefore, PA was only a partial mediator and disease severity did not operate in the manner predicted. In fact, the role played by disease severity is not in line with past research. For example, in Carver and Antoni’s (2004) study, BF was longitudinally, positively related to positive affect at follow-up among patients with cancer.
These unexpected results could be explained by the fact that more time may be needed to see changes in the relationship between PA and BF based on risk stratification, as all variables were measured soon after the CVD diagnosis. Since BF levels increased following participation in CR, levels of PA may have also changed, which could have revealed a different relationship between all three factors at completion of CR. Therefore, future research is needed to examine these relationships over longer points in time beyond participation in CR. It is also possible that the modifiable nature of many CVD risk behaviors may leave patients at highest levels of disease severity feeling overwhelmed or anxious. By extension, patients with high levels of disease severity may perceive the task of changing their various health behaviors as a stressor. Those low in disease severity may be better able to recognize benefits because their prescribed behavioral changes are fewer in number. It is also possible that patients with higher disease severity experience increased stress overall due to being at higher risk for poor outcomes, compared to those with lower disease severity who may see less at stake if they do not make significant health behavior changes. Therefore, additional work in this area should compare the cognitive and affective processes surrounding BF in different patient populations.
When controlling for risk stratification, consistent with past research, BF was positively related to both PA and healthy dietary behaviors. For example, Llewellyn et al. (2013) stated that BF is more likely to be related to positive outcomes (e.g., optimism) compared to negative outcomes because the ability to identify positive benefits may be unrelated to adverse effects. As mentioned above, one meta-analysis found that BF was negatively related to symptoms of depression, but positively related to well-being and PA (Helgeson et al., 2006). Therefore, this study filled in a gap in the literature as it was previously unknown whether improved health outcomes such as healthy dietary behaviors were positively related to BF among patients in CR.
Results also showed an unexpected negative relationship between PA and heathy dietary behaviors. A possible explanation for this unexpected association may be the affect-as-information approach (Schwarz et al., 1991). This approach argues that individuals in a positive affective state may not be motivated or able to process decisions as carefully as they should, which may lead them to be satisfied with quick, heuristic judgments or misinformation. Therefore, individuals with high levels of PA may be less inclined to use analytical reasoning when deciding what to eat, possibly leading to unhealthy dietary choices.
Implications and future directions
These findings imply that health providers should encourage patients with CVD who participate in a CR program to engage in BF, as there may be a positive correlation with healthy dietary behaviors. In turn, healthy dietary behaviors have been linked with a number of positive health outcomes (e.g., decreases in body mass indices, systolic blood pressure, fasting blood sugar levels, and low-density lipoprotein; Said et al., 2021). However, patients should be reminded to make thoughtful decisions when in a positive mood if they are inclined to choose less healthy food options. While patients may experience positive emotions from engaging in BF, they may also be inclined to make risky food choices. This study of patients in CR is the first of which we are aware to test PA as a mediator of the BF/healthy dietary behaviors relationship, and to test for moderation by disease severity. Future research should examine BF at more than two times in the context of CR in order to examine trajectories.
Limitations
This study has a few limitations worth noting. First, participants were recruited from a single SNH in the Midwestern United States so results may not generalize to all patients in CR. Also, individuals were excluded from participation if they were unable to engage in exercise, so adults with CVD and physical impairments were not represented in the study. That said, the socioeconomic diversity of this sample can be considered a strength. Second, participants may have been subject to memory biases or distortions when filling out the BF scale, or to biases, such as the social desirability effect. Other possible memory biases or distortions include recall errors, so participants may have misremembered past actions or thoughts. For example, participants may have had difficulty recalling their PA from the past 2 weeks. Another possible limitation is that the PA and BF scales were adapted for use with a CR population, so they have not been previously used or validated with a sample of patients in CR. However, the internal consistency was found to be excellent in this sample at Time 1 for the adapted PA scale and at both Times 1 and 2 for the BF scale. A fourth potential limitation was that there were only two periods of data collection, so participants’ changes over time were limited to 3 to 4 months. Longer spans between data collection points and additional points of data collection following CR may be needed to detect meaningful changes in such cognitively- and emotionally-complex constructs. There is also the potential limitation of this being a correlational study as causal relationships between variables including BF, PA, and healthy dietary behaviors cannot be ascertained.
Conclusion
BF may be a type of positive coping strategy in which individuals identify benefits following stressful events (Pascoe and Edvardsson, 2013), including an illness or diagnosis such as CVD. BF may also be used as a buffer against the negative effects of stress on health outcomes (Helgeson et al., 2006). This study sought to fill the gap in our understanding of the relationship between BF and healthy dietary behaviors among patients with CVD in a CR program. Results supported the first hypothesis: BF levels significantly increased over the course of CR. However, the second hypothesis was only partially supported. While PA partially mediated the link between BF and healthy dietary behaviors, the strength of this mediating relationship differed based on participants’ disease severity. Contrary to our predictions, the positive association between BF and PA was stronger for those low in risk. Results also suggest that health practitioners may want to caution patients in positive moods from making quick decisions about food, as our findings showed an unexpected negative relationship between PA and healthy dietary behaviors. Future research is needed to examine the relationship between positive affect, BF, and risk stratification at more than one point in time and months beyond participation in CR.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: (1) This work was supported by the National Institutes of Health (National Cancer Institute grant [#T32CA193193]); (2) funds from the University of Missouri-Research Board awarded to Kym Bennett; and (3) funds from the UMKC School of Education, Social Work, and Psychological Sciences Elizabeth Noble, PhD award fund.