
Abstract
The current study aimed to examine the health-related quality of life (HRQoL) and to identify its related factors amongst adult patients with type 2 diabetes mellitus (T2DM). This cross-sectional study recruited randomly 519 patients diagnosed with T2DM for at least 6 months in the Family medicine center (FMC) of Agricultural General Hospital in Hanoi, Vietnam. The Short Form 36 (SF-36) health survey was used to measure their HRQoL. The female patients had lower physical and mental scores than the male patients. Patients with older age, comorbidity, and insulin treatment were more likely to have lower HRQoL. Meanwhile, educational attainment and having frequent exercise were positively associated with HRQoL.
Introduction
Diabetes mellitus is one of the most common chronic, non-communicable disease that has been rising rapidly from 108 million people in 1980 to approximately 463 million in 2019 worldwide (IDF Diabetes Atlas 9th edition 2019, n.d.; Roglic and World Health Organization, 2016). Every one out of five people who are above 65 years old have diabetes, and most of them are living in low- and middle-income countries (IDF Diabetes Atlas 9th edition 2019, n.d.; Zhou et al., 2016). According to the World Health Organization (WHO), type 2 diabetes mellitus (T2DM) is the most common form of diabetes (WHO, n.d.). Individuals diagnosed with diabetes mellitus suffer not only from the dangerous health-related complications but also from a decrease in their quality of life (Jing et al., 2018; Schram et al., 2009).
Health-related quality of life (HRQoL) is a multi-dimensional concept which persists individual’s perception of physical, emotional, and social well-being (Rubin and Peyrot, 1999; Trikkalinou et al., 2017). Many studies show that people living with T2DM have lower quality of life than healthy persons due to high pressure of treatment (John et al., 2019; Polonsky, 2002). For chronic diabetic patients, a complete cure is an impossible task, therefore, it is important to keep patient at a stable stage, both physically and mentally. Understanding the predictors and identifying risk factors of HRQoL are important to developing comprehensive interventions and treatments for those living with diabetes (Moriarty et al., 2003).
Evaluation of HRQoL of people living with diabetes is a burning topic with many studies worldwide, including USA (Ahn et al., 2018), Europe (UK Prospective Diabetes Study Group, 1999; Redekop et al., 2002), and Asia (Arifin et al., 2019; Pan et al., 2016; Pham et al., 2020). Many associated factors between HRQoL of them has been highlighted (Arifin et al., 2019; Pan et al., 2016; Pham et al., 2020). Most have found relationships between HRQoL and sex, age, financial status, educational attainment, occupations, body mass index (BMI), concomitant risk factors (hypertension, dyslipidemia, etc.), treatment therapy, and their lifestyle.
Vietnam is a lower middle-income country where diabetes incidence is increasing with an alarming rate (Nguyen et al., 2015). By 2035, the prevalence of diabetes and pre-diabetes might rise to 7% and 15.7% of total population, respectively (Pham and Eggleston, 2016). Thus, diabetes is one of the most concerning issues of Vietnamese healthcare providers and policy makers. Little empirical evidence of HRQoL of people living with T2DM, however, exists in resource-scarce settings like Vietnam (Nguyen et al., 2018). This study aimed to measure the HRQoL of patients with T2DM and identify its associated factors in the Family medicine center (FMC) of Agricultural General Hospital in Hanoi, Vietnam in 2019.
Method
Study design
In the end of 2019, a cross-sectional interviewer-administered survey was conducted amongst out-patients of the Family medicine center (FMC) of Agricultural General Hospital in Hanoi, Vietnam. The FMC of the Agricultural General Hospital is the first family doctor center in Hanoi established in 2010 with the support of Liege University, Belgium (VUFO, 2020). In 2019, the FMC was merged into the out-patient department, where out-patients of diabetes are managed (Agricultural General Hospital, 2018). Moreover, Family medicine center (FMC) of Agricultural General Hospital was chosen because of its accessibility and availability of people living with diabetes in the databases.
A random sampling of the total 2523 patients with T2DM was retrieved from the electronic medical records of FMC. We applied the following formula to calculate the sample size for a finite population (Daniel and Cross, 2018):

Zα/2 = 1.96 for the Normal distribution at α/2 for a confidence level of 95%, d = 0.04 (margin of error), p = 0.5 (to get the highest sample size), and N is the population size. After adding a 10% of refusal rate, a total of about 515 is the needed sample size.
Patients were randomly chosen and invited to enroll in the study if they met the following criteria: (1) aged ⩾ 18 years old; (2) diagnosed with T2DM since at least 6 months; (3) diagnosis was performed based on the “Guidelines for diagnosis and treatment of T2DM” issued by the Ministry of Health in 2017 (Decision No. 3319/QD-BYT) (Ministry of Health, 2017); (4) agreed to participate; and (5) was able to answer the questionnaire. Among 2523 patients of random sampling pool, we invited 562 patients to participate the study. A total of 519 patients fulfilled all inclusion criteria and agreed to participate in the study.
The data collection team included four well-trained undergraduate medical students. Medical staff in the hospital were not chosen to minimize the social desirability bias. Patients were interviewed directly when they finished their regular diabetic examination.
Measurements and instruments
Prior to the (primary) survey, 20 participants with various socio-economic characteristics were piloted to check for the content validity of the questionnaire. Only minor word changes were made based on the feedback of participants. The questionnaire included the following information:
Socioeconomic characteristics
Information was self-reported by the participants in terms of sex (male/female), age, occupation (working, unemployed, and retired), educational attainment (primary school or lower, secondary school, and high school or higher), and BMI (<23, ⩾23 to <25, and ⩾25).
Diabetes treatment-related characteristics
Participants were asked about their health risk behaviors, including smoking, alcohol drinking, and physical activity. The questionnaire was also designed to explore patients’ duration of diabetes, comorbidities, distance to the closest health facility, health insurance, and self-care ability.
Psychological measurement using Short Form (SF-36) questionnaire
The Short Form 36 (SF-36) health survey questionnaire is a popular tool to measure quality of life. The SF-36 questionnaire has been widely used and validated in Vietnam (Pham and Do, 2017). The SF-36 contains eight dimensions for assessing physical functioning (PF), role limitations caused by health problems (RP), bodily pain (BP), general health perceptions (GH), vitality (VT), social functioning (SF), role limitations caused by personal or emotional health problems (RE), and general mental health (MH). The first four dimensional is summed to create the physical composite score (PCS), while the last four dimensional is summed to create the mental composite score (MCS). Total score for the SF-36 ranges between 0 and 100, with higher scores indicating a better quality of life.
Statistical analysis
Statistical analysis was performed using Statistical Package for the Social Sciences 23.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to summarize the patients’ characteristics. Independent samples t-test or Mann–Whitney U test was used for group comparisons. Pearson’s correlation was performed to test the correlation among continuous variables while Spearman’s correlation was performed among ranked variables. Because the outcome data were normally distributed, multivariate linear regressions were applied to examine factors associated with psychological problems. All statistical tests were two-sided (α = 0.05). P-value <0.05 was accepted as significant.
Ethics approval
This study was approved by the Institutional Review Board of Agricultural General Hospital in Vietnam. All participants were assured of confidentiality, asked to sign an informed consent, and given instructions informing them about the ability of refusing to answer any question or discontinue their participation at any time. Patients’ personal information collected from interviews was encoded and only researchers had the ability to access data. All data was used for research purposes only.
Results
Table 1 presents the socio-economic characteristics of all participants, in which over half of them were female. The mean age of our sample was 67.04 years of age (±8.52), and there was no statistical difference between the ages of two sexes. 68% of male were retired, compared to 59.4% of female. There was a significant difference in educational attainment between male and female (p < 0.001), in which 25.2% of female completed primary school or lower, much higher than that in male (9.5%). All of participants had health insurance.
Characteristics of study participants (n = 519).

Italicized values are significant at ***p < 0.001 from Chi-square t-test results.
Regarding health-related information, 75.8% of participants had comorbidity. Hypertension and dyslipidemia were the two most common comorbidities among 519 participants (55.3% and 37.0%, respectively). The mean duration of diabetes was 7.97 ± 6.41 and 8.10 ± 6.51 in male and female, respectively. Besides, 24.6% of patients were overweight and 29.3% were obese. There was, however, no significant difference between male and female.
In terms of lifestyle, the proportion of female and male patients that had family members with diabetes were 24.9% and 18.9%, respectively. The proportions of the male patients smoking and drinking alcohol were significantly higher than that in female patients (p < 0.001). Only 2% of female smoked and 3.7% drank alcohol, compared to about half of male smoked and drank alcohol. Both sexes did exercises at regular basis (75.4%), however, there was no significant difference in the frequency of doing exercises between male and female patients.
Table 2 highlights the scores of eight domains of HRQoL of study participants by sex. There were significant differences between the scores of male and female in five out of the eight SF-36 domains. Besides, both composite scores and overall QoL score were statistically significant different as well. The physical composite score of male patients was higher than that in female patients (53.34 ± 18.19 comparing to 47.31 ± 15.35), indicating a higher physical HRQoL. Also, the mental composite score highlighted higher values for male compared to female (65.32 ± 13.60 and 62.01 ± 11.77, respectively), indicating a higher mental HRQoL as well. Not surprisingly then, the male’s overall HRQoL was statistically higher than female’s (59.21 ± 14.30 vs 54.74 ± 11.66, p < 0.001).
Quality of life scores of study participants by sexes.
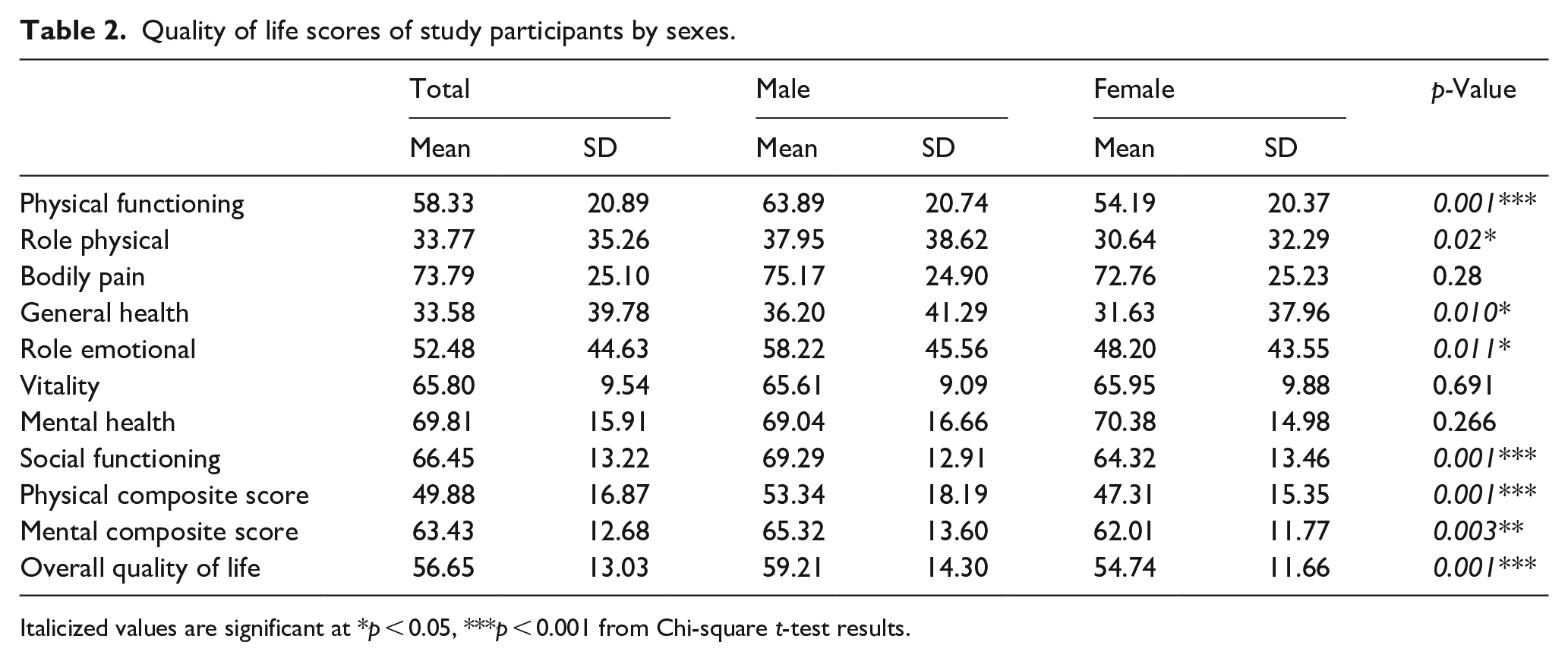
Italicized values are significant at *p < 0.05, ***p < 0.001 from Chi-square t-test results.
Figure 1 illustrates a significant positive correlation between physical composite score and QoL as well as mental composite score and QoL (p < 0.001). In particular, the coefficient indicated that for every additional point in physical score, HRQoL score was expected to increase by an average of 0.91 points. Similarly, for every additional point in mental score, HRQoL score was expected to increase by an average of 0.83 points.

Correlation between physical and mental composite scores and quality of life.
Table 3 shows the results from multivariate regression identified factors associated with HRQoL among people living with diabetes mellitus in Hanoi (Vietnam). Higher education level, no diabetes complications, and no insulin treatment were associated with a higher physical score as well as mental score, and therefore, they had a higher QoL (p < 0.05). Meanwhile, older age was negatively associated with both physical score (Coef = −4.442; 95% CI: −12.816, −4.946, p < 0.001) and mental score (Coef = −4.176; 95% CI: −9.270, −3.331, p < 0.001). Older people living with diabetes had worse QoL (Coef = −5.157; 95% CI: −10.454, −4.678, p < 0.001). Doing physical exercise only had a significant relationship with physical score (Coef = 2.344, 95% CI: 1.081, 12.404, p < 0.05). This relationship could not be found in mental score.
Factors associated with HRQoL among diabetic patients.

<0.05. **<0.01. ***<0.001.
Table 3 also reveals that physical and mental scores of people living with diabetes and without hypertension were significantly higher than those got both diabetes and hypertension. As a result, the former had a higher QoL (Coef = 2.605; 95% CI: 0.769, 5.488; p < 0.01). Meanwhile, there was no significant relationship between having dyslipidemia or heart diseases and QoL (p > 0.05). Patients with only diabetes had a better mental score than those with both diabetes and lung diseases (Coef = 2.477, 95% CI: 1.366, 11.832, p < 0.05).
Discussion
Our study brought valuable evidences about the HRQoL of people with type 2 diabetes mellitus (T2DM) who were being treated in the Family medicine center (FMC) of Agricultural General Hospital in Hanoi, Vietnam. In this study, we found that our participants had lower physical score and mental score than those in Chinese (Hu et al., 2015) but higher than those in Swedish (Svedbo Engström et al., 2019) and US (Ahn et al., 2018). Although, our sample did not include healthy adults, previous studies found that T2DM people have lower scores of HRQoL than the general population with the same age (Koopmanschap, 2002; Pan et al., 2016).
Over the past few years, many studies investigated deeply into the differences between male and female with diabetes. Female with diabetes appeared to have worse HRQoL than male with diabetes (Al Hayek et al., 2014; Undén et al., 2008). Similarly, our study showed that the SF-36 score in male was higher significantly than in female. Males had significantly higher scores than female in five out of eight domains, except bodily pain, mental health, and social functioning. This result was in line with other studies worldwide. In United Kingdom, researchers found that female patients had lower score in all domains except bodily pain (Woodcock et al., 2001). Similarly, among Australian population, female with diabetes had poorer HRQoL than male in seven out of eight domains (Chittleborough et al., 2006). In an Asian country like India, male participants also had statistically significant higher HRQoL score than female counterparts (Gautam et al., 2009).
The relationship between diabetes and HRQoL is complex and can be affected by various factors in different contexts. Under this study, multivariate regression model confirmed that age was statistically significantly associated to both physical and mental component of HRQoL, which is consistent with previous studies (Gabric et al., 2018; Wexler et al., 2006). Age is the strongest predictor among demographic, lifestyle, and clinical factors (p < 0.0001). Similar findings have been reported in both European and Asian studies with inverse correlation of HRQoL and age (Gabric et al., 2018; Wang and Yeh, 2013). In the fact that elderly people usually have more than one chronic conditions, which means that they might have cognitive complications and have to take multiple medications, which is one of many factors that impacts their physical and mental health (Brown et al., 2004; Nguyen et al., 2018).
This study also found the impact of the education attainment on HRQoL of people living with diabetes. People with higher education were more likely to have better HRQoL. There are contradictory results about the relationship between education and HRQoL of people living with diabetes. In Serbia, Spasić et al. (2014) found no significant relation between these two factors. Meanwhile, in accordance with the current study, a study in United Kingdom claimed that having more than 12 years of education can positively affects HRQoL of T2DM people (Wexler et al., 2006). Some studies believed that patients with diabetes who had higher education might have better social provision, positive self-esteem, and good understanding of the disease which led to treatment adherence to achieve better health status and life quality (UK Prospective Diabetes Study Group, 1999; Redekop et al., 2002).
Comorbidity has been reported to be highly prevalent among people living with T2DM (Chung et al., 2013; Larkin et al., 2015; Spasić et al., 2014). Consistently, approximately three-fourths of our sample reported that they had other comorbid conditions. Hypertension and dyslipidemia were the two most common ones. However, the prevalence of these two diseases were lower in a recent research in Vietnam in 2019 (78.4% and 81.2%, respectively) (Nguyen et al., 2019). Results from regression model indicated that those suffering from diabetes complications were more likely to report lower HRQoL. This result is in line with other recent studies in Vietnam and other countries (Arifin et al., 2019; Gillani et al., 2019; Pham et al., 2020). These diabetes complications have the potential to add significant health and finance burdens, and have been associated with diminished HRQoL in adults (Wexler et al., 2006). As a result, it makes the treatment of patients become more challenging, which requires a comprehensive intervention program to improve patients’ health status and life quality.
In this study, we found that people without insulin injection have a statistically significant better HRQoL in both physical and mental component compared to those using this therapy. A large study from the U.S. reported that individuals on insulin had a lower HRQoL score than those who took oral agent (Glasgow et al., 1997). Moreover, people living with T2DM switching from oral medication to insulin therapy tent to have more difficulties on social functioning, bodily pain and mental health than those who were not treated with insulin (Goddijn et al., 1999). By contrast, various studies indicate that the relationship between them is not significant or the change of treatment has no impact on HRQoL (Chung et al., 2013; Mayberry and Osborn, 2012; Sakamaki et al., 2006). The lower HRQoL in insulin-treated patients is likely explained by the suffering associated with a heavier burden of expense and living conditions (Wang and Yeh, 2013). In addition, daily insulin injections may cause pain and increase the fear of insulin dependent in patients, which probably depress them and further reduce HRQoL (Vancampfort et al., 2015). Therefore, educational counseling programs for insulin-treated patients are necessary to improve their life quality.
Last but not least, physical exercise is another key factor shown by the multivariate analysis to be associated with better HRQoL, especially in physical components. Sung et al. found that a regular exercise program results in increased daily activity, activity intensity, and energy expenditure levels; as well as decreased biochemical effects, FBG, HbA1c, and TG levels among T2DM elderly, which helps to improve their life quality in general (Sung and Bae, 2012). The meta-analysis on diabetes and physical training confirmed that patients with diabetes is beneficial for controlling disease and enhancing HRQoL (Cochran and Conn, 2008). A systematic review on 18 articles also supports this idea, where they found that patients who did more physical exercise had better HRQoL in five subscales of SF-36, including role physical, general health, vitality, social functioning and mental health.
Our study suggests that HRQoL of patients with T2DM can be affected by various factors, including demographic, lifestyle, and clinical. Educational counseling programs would help people to understand their health status and treatment, thereby improve their treatment adherence and positive attitude toward diabetes. Furthermore, it is important to providing interventions to limit diabetes complications, medical side effects, and offering psychological support during treatment. Doing physical exercise also plays an essential role in reducing the risk of HRQoL impairment.
The results of the current study should be interpreted in the light of a few limitations. Due to the cross-sectional design, it was not possible to draw conclusions on the cause-and-effect relationship between HRQoL and associated factors. The generalizability of our study results to other hospital settings and/or national population is limited because our data was collected in only one hospital of Vietnam. The recall bias and the use of self-reported data also limits our results. Finally, SF-36 is one of the most common HRQoL measurements, however, based on the intentions, researchers can choose to assess health quality via different tools, thus, it may lead to the different findings.
Conclusion
In conclusion, the results of this study brought evidences on HRQoL of patients with diabetes in the Family medicine center (FMC) of Agricultural General Hospital in Hanoi, Vietnam. Sex, age, educational attainment, diabetes complication, and treatment therapy were risk factors for both physical and mental components of HRQoL. It is vital to understand the effect of diabetes on HRQoL in order to improve health status and life quality of those with diabetes.
Footnotes
Acknowledgements
We would like to express my very great appreciation the board of directors, doctors, especially doctors at Family medicine center of the Agricultural General Hospital. Special thanks to all patients who have enthusiastically participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.