
Abstract
Physical activity restrictions can be particularly difficult for children with hemophilia and their parents, as most children want to engage in the same activities as their friends or siblings. This study aimed to assess parents’ need for a booklet on how to manage physical activity restrictions based on the self-determination theory and gather their suggestions for the booklet’s improvement in a focus group. Data were analyzed using thematic analyses to highlight to what extent the needs of parents were met by the booklet, as well as their suggestions for improvement. A discussion on the methodology of the booklet’s creation is also presented.
Keywords
Introduction
Hemophilia is a bleeding disorder in which blood clotting is prolonged due to a missing clotting factor. Hemophilia patients require regular infusions of the missing clotting factor, as well as important precautions for the detection and prevention of bleeding episodes. Repeated muscle and joint bleeding can lead to arthropathy, chronic pain, and loss of range of motion in the long-term (Garcí a - Das í et al., 2015; McLaughlin et al., 2014). After diagnosis, parents must quickly learn to handle many tasks, such as securing the home, recognizing bleeding symptoms, and learning how to infuse, in order to keep their children safe (Shaw and Riley, 2008). Parents often feel overwhelmed by their new responsibilities (Edmunds et al., 2007). They may also feel uncomfortable with administering painful infusions and they may worry about their child’s safety (Beeton et al., 2007).
Parental care evolves as the child ages. A new area of questions and concerns usually arises when the child becomes interested in organized sports. Although physical activity is highly recommended to prevent bleeding in the muscles and the joints, patients with severe hemophilia are commonly advised to avoid certain types of sports that are at risk of causing bleeding, such as football and hockey (Anderson and Forsyth, 2005; Broderick et al., 2012; Mulder et al., 2004). Physical activity restrictions vary according to disease severity, joint health, and muscle strength (Petrini and Seuser, 2009; Srivastava et al., 2013). Physical activity restrictions can be particularly difficult for children, as most want to engage in the same activities as their friends or siblings (Williams and Chapman, 2011). Children commonly react with sadness and anger when given physical activity restrictions. Balancing the child’s desire for a normal active lifestyle and the need to protect them from risk represents a dilemma for parents (Shaw and Riley, 2008). Some decide to allow their children to participate in high-risk sports and hope that they will not injure themselves, while others tend to adopt overprotective behaviors (Abali et al., 2014; Beeton et al., 2007). Non-compliance with physical activity recommendations issued by healthcare providers is common among children with hemophilia (Bérubé et al., 2017; Nazzaro et al., 2006; Ross et al., 2009).
The self-determination theory (SDT) is helpful in understanding the process by which parents can set limits without compromising their child’s well-being, in addition to increasing their self-motivation to comply with healthcare providers’ recommendations (Deci and Ryan, 2002). According to this theory, parents can foster the development of a more autonomous and long-lasting form of motivation for health-related goals in their child by adopting an autonomy-supportive style of communication (Ryan and Deci, 2017). This theory is particularly helpful in the context of growing children who gradually need to acquire more autonomy in regard to their illness management. Studies on the SDT have shown that self-motivation for self-care health behaviors, even the ones that are not pleasant in themselves, can be fostered in children and adolescents. For example, parental autonomy support has been shown to preserve patient glucose monitoring frequency during adolescence, when glucose monitoring typically decreases (Wu et al., 2014). An environment that supports autonomy has also been shown to promote greater motivation for physical activity (Huéscar Hernández et al., 2020; Lim and Wang, 2009).
Autonomy-supportive parenting is focused on meeting the three basic psychological needs of children: autonomy, competence, and relatedness. Meeting the need for autonomy involves the active nurturing of the child’s capacities to self-regulate using techniques like taking the child’s perspective, offering meaningful choices, and encouraging initiative and self-expression. Meeting the need for competence refers to using scaffolding strategies, providing non-evaluating feedback, and setting limits in a non-controlling way. Finally, meeting the need for relatedness refers to being involved with the child in a warm, caring, and non-judgmental manner (Deci and Ryan, 2002). Further information on the theoretical background of this study, as well as the SDT’s communication strategies, has been published elsewhere (Bérubé et al., 2016).
Studies have highlighted the need to support parents of children with hemophilia in managing their responsibilities (Beeton et al., 2007; Bottos et al., 2007). However, only a few studies on interventions for parents have been conducted in hemophilia and no known empirically tested interventions focus specifically on helping parents manage physical activity restrictions (Cuesta-Barriuso et al., 2014; Dutreil et al., 2011; Kennedy et al., 2017; Penica and Williams, 2008). A literature review confirmed that, when properly designed, health information leaflets can increase satisfaction, knowledge and adherence to treatment (Sustersic et al., 2017). Among other benefits, the availability of educational materials increases the effectiveness of verbal communication (Wizowski et al., 2008).
In the literature, the methodology used for the development of health-related or psychosocial information material for patients and their family is rarely detailed. Although guidelines are available, they remain broad and do not detail the concrete steps to accomplish the development and need assessment of information material using a mixed method (Farrell-Miller and Gentry, 1989; Oliver et al., 2008a). Furthermore, knowledge transfer has repeatedly been identified as an important issue in the scientific community. It is paramount to support patients and their family by providing them with access to quality information material derived from empirically validated models.
The aims of this study were: To develop, with the help of healthcare professionals in hemophilia, a theory-based booklet for parents of children with hemophilia focused on how to manage physical activity restrictions and recommendations; To assess parents’ need for the type of material developed (i.e., a theory-based booklet) and to gather their suggestions for the booklet’s improvement in a focus group; To improve the booklet based on the suggestions elaborated in the focus groups with parents and meetings with the healthcare team. To present a detailed methodology on the creation, adaptation, and assessment of the need and acceptability of a theory-based booklet.
Methods
Booklet development
The methodology for the booklet development was based on recommendations for the production of written material for patients. (Oliver et al., 2008b; Sustersic et al., 2017). The booklet content was elaborated in collaboration with a nurse, a psychologist, and a social worker from Sainte-Justine University Health Centre’s Hematology Clinic, in Montreal
The healthcare professionals were first approached to discuss the need for providing parents with written material on physical activity management. The healthcare professionals expressed that there was a lack of written materials in hemophilia, particularly on physical activity management. At this first meeting, we held a brainstorming session to determine the target population, and the key concepts that should be addressed in this booklet. Following this meeting, a first version of the booklet’s content was produced by the research team using the SDT and taking into account the healthcare professionals’ ideas and key concepts. A second meeting with the healthcare professionals was held to review the booklet’s content. They were invited to suggest ideas and changes. Their suggestions were immediately discussed to reach consensus within the healthcare team. Subsequently, each professional was met individually to work on the writing. A final meeting with all healthcare team members was held to achieve the version to be presented to participants. This version did not include images, although text boxes indicated where the images would subsequently be added. This was done with the idea that participants would feel more comfortable to criticize or propose major changes to a draft document than a document that looked in its final form. Further information on the adaptation of communication tools from the SDT to the specific context of hemophilia has been published elsewhere (Bérubé et al., 2016).
Booklet evaluation and suggestions for improvement
Participants
For this study, we approached parents of children with severe hemophilia treated at the Hematology Clinic. At the clinic, patients from the same age group have the same biannual appointment where they meet with each of the healthcare professionals during the day and participate in different group activities. We identified two groups representing an acceptable range of school-age children: 5–7 year-olds and 8–9 year-olds. An informative email was sent to all eligible parents and we contacted all parents who did not opt out after receiving the email. We aimed to recruit 5–10 parents for each of the two focus groups. Parents aged less than 18 years, and children or parents with a severe psychiatric disorder were excluded from this study. In total, 11 parents (eight mothers and three fathers) of pediatric patients aged 5–7 years old (60%) or 8–9 years old (40%) with hemophilia A (60%) or B (40%) were recruited and participated in the focus groups. In the 8–9 year-old group, at least one parent of every child that attended the hemophilia day at the clinic accepted to participate, while in the 5–7 year-old group, the parents of two children who attended the hemophilia day refused to participate in the study, saying they were not interested. The Sainte-Justine UHC Research Ethics Board approved this study (#2018-1877).
Procedure
The study design was a sequential mixed method based on a questionnaire, and focus group interviews about the booklet to evaluate its pertinence and acceptability (Creswell et al., 2003). First, parents participated in a 30-min information session about the study during which the booklet was presented. They were then invited to fill out a questionnaire about the booklet to share their opinions on different dimensions (see Measures). Finally, they took part in the focus group interview, which placed emphasis on the elements that had been negatively evaluated in the questionnaire. Parents were invited to discuss each of these elements and to suggest ways to improve them. In total, there were two focus group interviews, one for each age group of children. The interviews were designed and conducted according to the recognized principles of focus group interviewing (Wilkinson, 2015). The facilitators’ role (SB, DO) was to ensure the fluidity of the discussion with open-ended questions. They were also responsible for ensuring that the discussion remained focused on the booklet and its improvement. If participants mentioned issues, concerns, or needs that were out of the scope of the present study, they were told that time would be set aside at the end of the interview to discuss these aspects. Particular attention was given so that all parents were able to express their opinion. The interviews were audio recorded and transcribed verbatim.
Measures
We developed a questionnaire (See Supplementary File 1). Our questions were inspired by ones used in previous studies (Kazdin, 2005; Ogez et al., 2019; Sahler et al., 2002). The questionnaire included 36 items relative to eight categories: the format (5 questions), the clarity of the information (2 questions), the structure (1 question), the length (2 questions), the expected positive effects (17 questions), the possible negative effects (2 questions), the usefulness and ease of implementation of the advice (4 questions), and the target population (3 questions). The responses were provided on a 6-point Likert scale for each suggestion, from 0 “strongly disagree” to 5 “strongly agree.” For each category of questions, space was provided to allow participants to write comments.
Analysis
Descriptive analyses were led on the scales completed by the parents. We compared the mean score of our sample to the middle scale point of 2.5 on the 0–5 scale with a Wilcoxon signed-rank test, to indicate whether mean perceptions were positive, negative, or neutral in our sample. Qualitative data (textual responses to open-ended questions in the questionnaires) and interview transcripts were processed and encoded using the NVivo 11 software by analysts who received appropriate training specifically for this study. A descriptive thematic analysis method was used to create an inventory of themes by two independent coders (SB, DO) (Massey, 2011). Agreement was reached after two meetings to reach the final coding structure and code descriptions. Our analysis was based on articulated data, that is, the information that was expressed by participants in response to the question posed (Massey, 2011). The objective was to ensure that all improvements proposed by the participants were identified, organized, and grouped together to facilitate the editing stage. In presenting the results from the qualitative data, participants were identified by alphanumeric codes in the subsequent paragraphs (P1 to P11). Since the aim of the focus group was to obtain rather short and technical responses focused on improving the booklet, only quotes that significantly added to accuracy or understandability were presented in the results. We embedded short quotes in the text, and longer quotations were presented in a distinct paragraph.
Production of the final version
We met again with the psychologist, the nurse, and the social worker to critically analyze the central themes (or suggestions for improvement) to assess whether they considered that the suggested changes should be implemented. Since the number of parents was deliberately limited, each comment was considered to likely represent the opinion of a significant number of parents. The themes were thus considered as equally important whether they represented the opinion of one or several parents. Each theme (i.e., suggestion for improvement) was evaluated based on its usefulness, its feasibility in a booklet-type documentation, as well as the extent to which it met the aim of this specific booklet, current scientific knowledge, and the values of our healthcare center (e.g., fostering the empowerment of people and communities). We worked to obtain a consensus between healthcare professionals, as to whether the proposed changes should be adopted. When this consensus was reached, we met individually with the members of the healthcare team to modify the booklet’s writing and presentation (the final version is available in Supplementary File 2).
Results
Booklet development
The consultation process with our hematology clinic’s psychologist, nurse, and social worker provided a rich brainstorming where many ideas were proposed. It was decided that the target population would be parents of school-aged children with hemophilia. The reasoning behind this decision was that it is generally at school age that children begin to compare themselves and want to move and play in the same way as their friends. While the healthcare team was not introduced to the self-determination theory concepts prior to the initial meeting, their suggestions on parenting strategies were largely in line with them. This facilitated the production and edition of the booklet in collaboration with the healthcare team. Consensus was easily reached when one professional wanted to change, add, or remove a topic. The only exception was that they could not easily decide who would be the resource person to refer parents to if they felt the need to talk or to have more information on the topic. It was finally decided that the message would be that every healthcare team member was there to provide support by listening to parents and/or referring them to the right specialist.
Booklet evaluation and suggestions for improvement
Responses to questionnaires
Parents’ responses as to their opinion about the leaflet.

Note. Item’s rating: 0 (totally disagree) to 5 (totally agree); M different than neutral point, * p < .05, ** p < .01.
Qualitative analysis of parents’ evaluation and recommendations from the focus groups
Format, length, and structure
During the focus groups, there was a consensus that the booklet was clear and easy to understand. Most parents considered booklet-type documentation to be a good and convenient format. P9 explained that a paper format allows parents to keep it for the time they will need it. However, P9 also felt that the booklet should be a little longer to give enough information without becoming too long to read. Importantly, some parents (P2, P3, and P9) also expressed that the booklet was only an introduction and that they would need more help with the aspects discussed in the booklet.
When parents were asked what they thought about the way the information was structured, the majority responded that it was well divided. However, one parent (P2) thought the information should be given in bullet points rather than in a continuous text. Another parent (P1) suggested keeping the structure as it was, but to add a summary of the important information to remember at the end of the booklet, an idea that was well received by P2 and other parents. All parents also agreed that a list of resources, activities, and links to more information on the subject would be useful if added at the end of the booklet.
Target population
Most parents suggested that the booklet should be distributed as soon as possible after the announcement of the diagnosis. Some parents (P9 and P11) pointed out that parents, after a diagnosis like hemophilia, usually tend to search for information on the internet about the course of the illness and the limitations their children will have to face, making the booklet more useful during this period. One parent in the 8–9-year-old focus group (P3) said that parents are masters of their trade after their child reaches a certain age and that the booklet would not be useful to them. P1 discussed the importance of applying the communication tools from the booklet as early as possible with their child.
P1: Well indeed I find that it is a booklet that should be given to you much earlier, because... precisely to build all this bond of trust there... and how we will interact with our child I find that it is from the beginning you know
For P9, the content might be useful to some people and not to others depending on many factors: the child’s health status, treatment type, knowledge, and parenting skills, etc.
Content
Some themes were highlighted by the parents as the most appreciated: the notion of teamwork with the child to find solutions (P2, P3, and P9 would have liked more emphasis on this aspect), P11 liked to be reminded that help was available to them if they needed it. Other parents (P6 and P11) indicated that the most useful advice they retained from the booklet was to listen to their child rather than rushing to solutions. P6: In that booklet, I make it a point, is that maybe to listen to him and let him talk instead of telling him you should do that. To say, how do you feel about it? What do you understand? To let him find his own solutions...
P9 and P10 expressed that the booklet’s possible comforting effect lied in its common sense which would reassure them that they are already doing the right thing for their child. However, P9 found that focusing on restrictions could generate some stress in the reader, and P10 said that it was important to de-dramatize the illness. These parents (P9 and P10) also expressed that the booklet was not specific enough to hemophilia and was lacking specific examples on how to apply the recommendations.
Missing content
Parents also highlighted different themes they felt were missing from the booklet. All agreed that mention should be made of how to encourage children to be physically active and how to valorize children. It was brought up that boys develop their self-esteem through their participation in sports (P2, P9, P10, and P11). Therefore, some parents (P1 and P10) thought the booklet should highlight that children who grow up with hemophilia acquire unique strengths: They are courageous (…) they are resilient (…).
Some parents (P7, P9, and P10) added that parental discourse should focus on possible and interesting alternatives. In this line, they (P10 and P11) suggested adding a list of ideas for safe physical activities for people with hemophilia. The idea of integrating these activities early in their child’s life also appeared fundamental to parents (P7, P9, and P10). P11 added that it was a good opportunity for parents to try new sports with their child and to share a unique moment that promotes the relationship.
Many parents (P2, P3, P10, and P12) mentioned that the notion of building a long-lasting trusting relationship was essential, since establishing a secure bond would help their child to integrate and refer to the rules. They also thought that this relationship might discourage the child from hiding injuries that would require attention. Many parents (P2, P3, P10, P11, and P12) felt that they should empower their children in their decisions, such as talking to them about the risks that they face in certain sports. These parents (P2, P3, P9, P10, and P12) also deemed important that the booklet more realistically addresses the notion of striking a balance between banning and allowing certain sports, as well as promoting flexibility to encourage parents to refrain from using excessive protection.
Some parents (P2 and P3) asked whether they should disclose their own emotions to their child. According to P3, expressing emotions to the child promotes a climate of cooperation. Many parents (P2, P3, P9, and P10) mentioned that they themselves experienced a kind of grieving process when they realized that their child would not be able to play certain sports, and, therefore, experienced some of the same emotions as their child. Several parents (P2, P3, P4, and P5) would have liked the booklet to mention that they have a right to feel guilty or sad and that it takes time to adapt to new challenges. P12 was concerned that restricting sports could cause depression in their child. Some parents (P10, P2, and P3) would have found it helpful to have examples of specific questions to ask their child to help them express themselves.
All other propositions that were not directly linked to the booklet are briefly addressed in Supplementary File 3 to guide further research.
Production of the final version
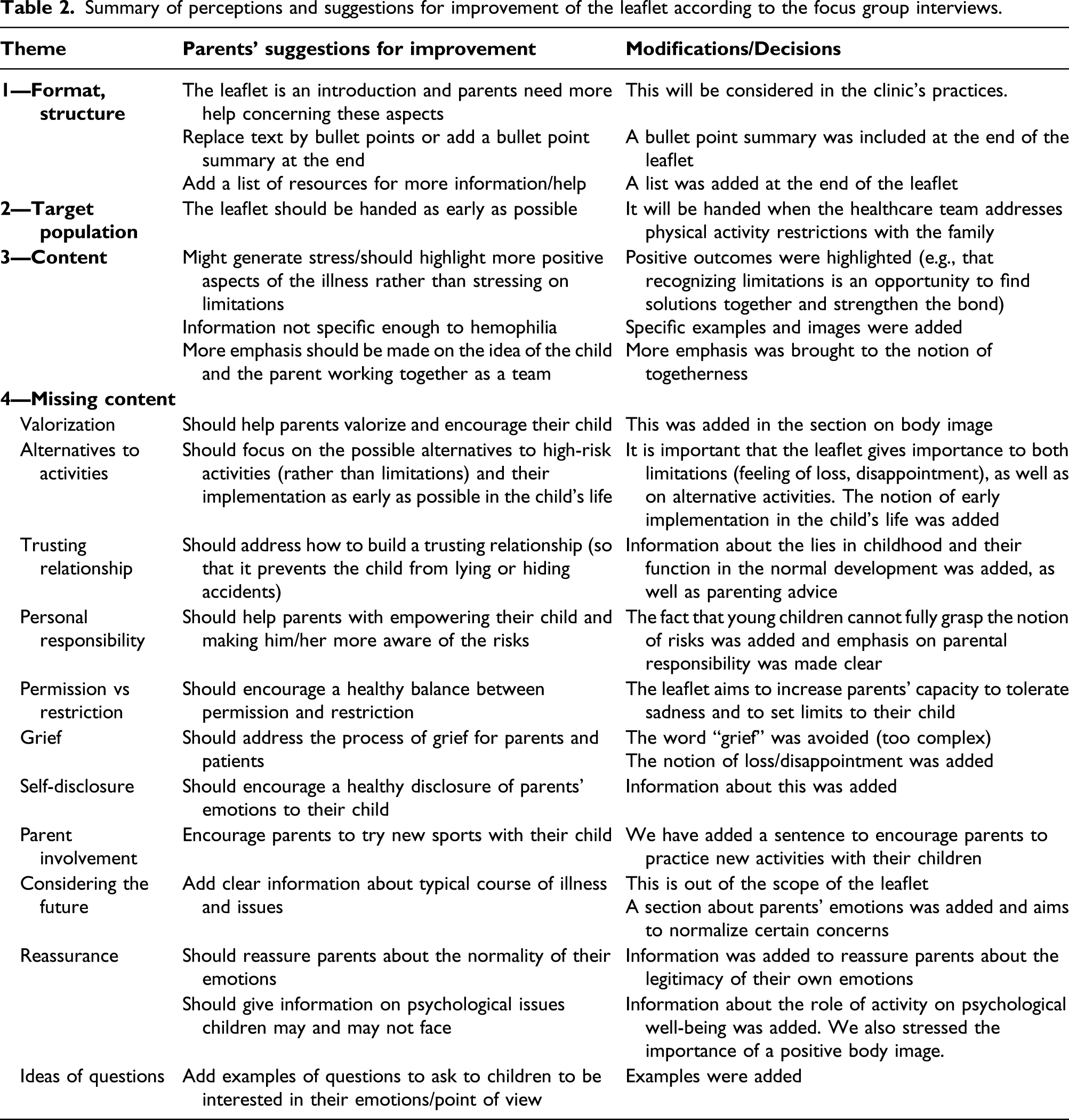
Summary of perceptions and suggestions for improvement of the leaflet according to the focus group interviews.
Discussion
It is recognized that healthcare settings should not only meet the medical needs, but also the practical and emotional needs of patients and their family (Oates et al., 2000). In this study, we (1) developed a booklet intended for parents of children with hemophilia based on the SDT, (2) assessed parents’ need for this type of material using a questionnaire and focus groups as well as (3) adapted the booklet according to most of their suggestions. Data collected helped us to refine the booklet in collaboration with healthcare providers.
The booklet development process with healthcare professionals went as planned. Having group meetings and one-on-one meetings with the staff made the writing process easier. Obtaining consensus on the points to be modified following parents’ comments from the focus groups was done without difficulty since the clinical staff members had already established certain guidelines in their communication with the parents. The anonymity of the comments also seemed to allow the team to distance themselves from the criticism that may have been raised by the participants.
As in other studies, parents easily described the challenges related to their child’s illness, and the strategies they used to try to overcome them (Williams and Chapman, 2011). The focus group allowed the team of researchers and healthcare providers to discover relevant themes to add to the booklet. Interestingly, many of the themes that parents felt were missing from the documents were in line with the SDT: building a trusting relationship, having a teamwork approach, and finding alternatives (Bérubé et al., 2016; Ryan and Deci, 2017). Some parents sought to foster a relationship of trust to prevent their child from lying to them about accidents or engaging in risky physical activity. The ability to lie and to keep secrets is part of the healthy development of a child, but can also be a problematic behavior in some instances (Talwar and Crossman, 2011). In hemophilia, small secrets can have big consequences, for example, the child hiding a bleeding accident or lying about engaging in a high-risk activity for fear of reprimand. It was decided that the booklet would explain the normalcy of occasional lies, but also promote, through parenting tips, a warm and sensitive relationship between the parent and the child, which could in turn reduce the number of lies. A study on lies in adolescence has shown a relation between parenting that supports autonomy and adolescents’ identification to the honesty value as well as perceived low costs/high benefits of honesty, which ultimately predicted honesty (Bureau and Mageau, 2014).
Another important aspect that emerged from the focus groups was that parents had questions about their own emotions and sought ways to understand and cope with them. They sought reassurance but also wondered whether they should disclose some of their emotions to their child. A study on mothers of children with hemophilia aged 8–12 years showed that 21% of these mothers reported clinical distress (Limperg et al., 2016). Parents sometimes think that giving their child less information or hiding negative emotions may protect them in return, but studies on the subject seem to support the added value of true parental communication, within a certain limit (Claflin and Barbarin, 1991; Karnilowicz et al., 2018). Parents’ emotional experience was also described as a grieving process in the focus groups. The grief of the healthy child is a well-known topic in the literature on parenting a child with a chronic illness (Kepreotes et al., 2010). In hemophilia, the grieving process surrounding physical activity restrictions is sometimes particularly difficult for fathers, as sports are culturally considered as an important aspect of fatherhood (Myrin Westesson et al., 2015). Parents in our study felt that the booklet was only an introduction and asked to receive a list of resources to accompany them, demonstrating their openness to receive more support. It is to be noted that at the Sainte-Justine University Health Centre’s hemophilia clinic, parents are invited to participate in different workshops and meet on a biannual basis: psychoeducational workshops for parents of children of different ages, groups and discussions with other parents, one-on-one meetings with the nurse, the doctor and the physiotherapist, optional meetings with the social worker and the psychologist, etc. Their interest in the booklet can be interpreted as a need to obtain information in different formats. The paper material can allow some parents to think more introspectively from their home and can also act as a reminder of the information that is explained in more detail during different activities.
Parents have conflicting decisions to make concerning their child’s physical activity, as they often want to let their children engage in the same activities as their peers. This sometimes brings them to rationalize that higher risk sports are sometimes acceptable (Beeton et al., 2007). We observed variability in compliance with recommendations in our participants. While some of our participants were very adherent or partially adherent, others said that they did not impose any restriction over their child’s physical activity, and this decision was sometimes hidden from the healthcare team. Some parents have expressed their discomfort with the emphasis on restrictions in the booklet and would have preferred that efforts be made to balance restrictions and permission. In fact, the idea of the booklet was specifically aimed at helping parents set necessary limits in a way that would not be detrimental to children despite the difficult emotions this might trigger. This can even have a positive impact on children’s well-being and self-motivation according to studies on the SDT (Edmunds et al., 2007; Núñez and León, 2015). We modified the booklet to reflect the positive aspects of setting limits and tried to make the booklet version attractive to parents, even though the subject is often a sensitive one. Importantly, the booklet’s purpose was also to encourage safe physical activity. An effort was made not to encourage overprotection which could have harmful effects on the child’s physical and psychological health. There is a consensus in the literature on the importance of encouraging physical activity for people with hemophilia (Harris and Boggio, 2006; Negrier et al., 2013). Furthermore, physiotherapists and other health professionals can recommend adjustments to certain sports to make them safer (Harris and Boggio, 2006; Negrier et al., 2013).
While approaches for developing interventions and material vary greatly, guidelines usually recommend using a focus group to assess needs before creating any material or intervention (Moscoso et al., 2013; Oliver et al., 2008b). In this study, since the need for this type of documentation was clearly stated by the healthcare team and since we knew, from the literature, that there were many issues surrounding physical activity in children with hemophilia, we decided to present participants with a draft version of the booklet. We believe that this way of proceeding enriched the dialogue between parents during the focus groups and provided a concrete support for their discussion. It may be difficult for some parents to conceive what kind of information might be helpful to them without being presented with some ideas. Importantly, participants were also invited to express if this type of documentation corresponded to their needs. Further studies will assess the effects of using the booklet.
Some limitations must be considered when interpreting the results. This is a single-site study based in Canada, where prophylaxis access is possible through the public healthcare insurance system, which limits the results’ generalizability. The intervention methods and the recommendations may differ substantially from one treatment center to another. Furthermore, the sample was conveniently selected based on dates of clinical appointment.
Conclusion
In conclusion, with the help of healthcare professionals, we conducted a mixed-method study to develop a booklet on managing physical activity restrictions and recommendations for parents. We also assessed parents’ need for this kind of material, collected their suggestions for improvement, and reviewed the booklet according to their suggestions. The results showed that despite the high-quality support offered at the Hematology Clinic for children and their family, parents seem to need better support and information on the issues related to physical activity. Parents expressed they needed a booklet that would be reassuring and would normalize their emotions. Parents were also particularly interested in concrete and specific information, such as the importance of silently listening to their child instead of rushing to solutions. They also wanted more parenting tips such as ideas of questions to ask their child to better understand their perception of the illness and its impact on their life. The study’s output is a booklet whose implementation could be studied in the hematology clinic. It is also ready to be adapted to other hemophilia treatment centers.
Supplemental Material
sj-pdf-1-hpo-10.1177_20551029211039920 – Supplemental Material for It’s difficult to say no: Development of a parenting booklet about physical activity restrictions and recommendations in pediatric hemophilia
Supplemental Material, sj-pdf-1-hpo-10.1177_20551029211039920 for It’s difficult to say no: Development of a parenting booklet about physical activity restrictions and recommendations in pediatric hemophilia by Sarah Bérubé, David Ogez, Jennifer Aramideh, Claudine Amesse, Claude J Bourque, Claire Longpré, Lorraine Muise, Ariane Levesque and Serge Sultan in Health Psychology Open
Supplemental Material
sj-pdf-2-hpo-10.1177_20551029211039920 – Supplemental Material for It’s difficult to say no: Development of a parenting booklet about physical activity restrictions and recommendations in pediatric hemophilia
Supplemental Material, sj-pdf-2-hpo-10.1177_20551029211039920 for It’s difficult to say no: Development of a parenting booklet about physical activity restrictions and recommendations in pediatric hemophilia by Sarah Bérubé, David Ogez, Jennifer Aramideh, Claudine Amesse, Claude J Bourque, Claire Longpré, Lorraine Muise, Ariane Levesque and Serge Sultan in Health Psychology Open
Supplemental Material
sj-pdf-3-hpo-10.1177_20551029211039920 – Supplemental Material for It’s difficult to say no: Development of a parenting booklet about physical activity restrictions and recommendations in pediatric hemophilia
Supplemental Material, sj-pdf-3-hpo-10.1177_20551029211039920 for It’s difficult to say no: Development of a parenting booklet about physical activity restrictions and recommendations in pediatric hemophilia by Sarah Bérubé, David Ogez, Jennifer Aramideh, Claudine Amesse, Claude J Bourque, Claire Longpré, Lorraine Muise, Ariane Levesque and Serge Sultan in Health Psychology Open
Footnotes
Acknowledgments
We are very grateful to Émélie Rondeau for her technical help during the data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sarah Bérubé received a studentship award from the Canadian Institutes of Health Research (CIHR), the Sainte-Justine UHC Foundation and the Fonds pour la Recherche du Québec en Santé (FRQs) in collaboration with the Fondation des Étoiles.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.