
Abstract
To date, little attention has been given to prenatal depression, especially in low and middle-income countries. The aim of this research was to assess the prevalence of depression and its associated factors amongst pregnant women in a central Vietnamese city. This cross-sectional study included 150 pregnant women from 29 to 40 weeks of gestation, from eight wards of Hue city, via quota sampling from February to May 2019. We employed the Patient Health Questionnaire (PHQ-9) to assess depression. Findings suggest the need to provide routine screening of pregnant women in primary care for depressive symptoms and other mental health problems.
Introduction
Depression is a common mental health concern that affects women globally, especially during the perinatal period (Howard et al., 2014). Its prevalence in pregnancy has been estimated to range from 6.5% to 26.7% (Gavin et al., 2005; Okagbue et al., 2019). The prevalence rates of antenatal depression differ within and between countries. Perinatal mental disorders are more prevalent in low- and middle-income countries (LMICs), compared to those from high income countries. In high-income countries, the prevalence of depression in pregnancy is estimated to range from 7.4% to 12.8% (Bennett et al., 2004), compared to 15.6% (95% CI: 15.4–15.9%) in LMICs (Fisher et al., 2012).
Evidence suggests that if not treated and diagnosed early, depression during pregnancy can have more serious consequences in the postpartum period (Falah-Hassani et al., 2017). Moreover, a number of short-term and long-long term adverse outcomes for the children of women who suffered from antenatal depression have been identified (Dunkel Schetter and Tanner, 2012; Gentile, 2017; Lefkovics et al., 2014). Such outcomes include increased risk of low birth weight, infants that are small for gestational age, preterm birth (Accortt et al., 2015; Grigoriadis et al., 2013; Staneva et al., 2015a; Szegda et al., 2014); and increased vulnerability to behavioral and emotional problems such as depression and other mental health issues in later childhood and adolescence (Plant et al., 2016; Van den Bergh et al., 2005).
In Vietnam, most research on depression in the perinatal period has focused on postnatal depression only (Do et al., 2018; Murray et al., 2015; Tran et al., 2018b, 2019; Upadhyay et al., 2019; Vo et al., 2017; Wesselhoeft et al., 2020), with a paucity of research focusing on antenatal depression. The two existing studies of antenatal depression amongst Vietnamese pregnant women report prevalence of 4.9% and 28.2% (Fisher et al., 2013; Ngo et al., 2018). Both of these studies were conducted in the North of Vietnam, and there has been limited research conducted throughout the rest of the country. Additionally, although a recent systematic review suggested that common mental disorders (including depression) are significantly associated with intimate partner violence during pregnancy (OR: 3.69, 95%CI: 2.51–5.42), the associated factors linking this to maternal depression remain unclear due to the complexity of this relationship and a lack of screening during pregnancy (Kingston et al., 2015). This study aimed to estimate the prevalence of depressive symptoms during pregnancy in 2019, and identify factors affecting depressive symptoms among pregnant women in a central region of Vietnam.
Methods
Study design
This research formed part of a pilot baseline study conducted as part of the Evidence for Better Lives Foundational Study (EBLS-FS)—among eight medium-sized cities from low- and middle-income countries, including Ghana, Jamaica, Pakistan, the Philippines, Romania, South Africa, Sri Lanka, and Vietnam. Details of the protocol have been published elsewhere (Valdebenito et al., 2020). In Vietnam, a cross-sectional study was conducted from February to May 2019 to estimate the prevalence of maternal health in Hue city.
Study setting
The study was conducted in Hue city, the ancient imperial capital of Vietnam and the capital of Thua Thien Hue province. Hue city is located in the central region of Vietnam, covering an area of 70.67 km2. Its population in 2018 was approximately 358,754 people and it is divided into 27 wards (Portal of Thua Thien Hue Province, 2020). The official estimate of the poverty rate in 2019 is approximately 1.51% (Thua Thien Hue Provincial People’s Committee, 2020).
Study participants
We included pregnant women with a gestational age ranging from 29 to 40 weeks, aged 18 years and above, residing in Hue city for at least 6 months. Exclusion criteria included women who refused to participate, or who planned to migrate from Hue city within 3 months after giving birth.
Sample size and sampling
A quota sampling method was employed to select 150 participants from a list of pregnant women who were recruited via ward health centers during their standard antenatal care visits in each ward selected for this study. The geographical stratification was based on the list of wards in the two Southern and Northern parts of Hue city. From the two parts of Hue City, eight out of 27 wards were randomly selected and then, from each selected ward, the midwife from the ward health center contacted eligible pregnant women for recruitment. As a result, a total of 195 participants were approached, and 150 pregnant women were successfully recruited, achieving a response rate of 76.9%. The 45 women who refused to participate cited reasons such as inadequate time for participating in the interview or imminent due date of delivery.
Measurements
The dependent variable
Depression: The Patient Health Questionnaire (PHQ-9) was used to measure the severity of depressive symptoms experienced in the last 2 weeks (Kroenke et al., 2001). The short module scores the nine DSM-IV criteria for depression, including anhedonia, dysphoria, sleep disturbances, fatigue, changes in eating, low self-esteem, concentration difficulties, hypo-or-hyper-active behaviors, and thoughts of suicide or homicide. Each item was rated on a 4-point Likert scale: Not at all = 0; Several days = 1; More than half the days = 2; Nearly every day = 3. The possible range was 0–27. A total score greater or equal to 10 was the cut-off for moderate to severe depression (Kroenke et al., 2001).
Independent variables
Maternal sociodemographic characteristics: We included maternal age, maternal education, employment status, type of relationship with the father of the baby, and perceived social status. Perceived social status was measured by using the MacArthur scale of subjective social status—a single-item on a 10-point Likert-type scale that assesses a person’s perceived rank relative to others in their group (Adler et al., 2000). Those who scored themselves as three or less were considered as having perceived low social status. Items on reproductive health and prenatal characteristics included unwanted pregnancy, parity, and frequency of prenatal check-ups.
Adverse Childhood Experiences (ACEs): The adapted 19 out of 31 items of the ACE-International questionnaire (WHO, 2019) were employed to measure any adverse experience before age 18 years. The domains included in this study were: emotional abuse; physical abuse; sexual abuse; violence against household members; living with household members who were substance abusers; living with household members who were mentally ill or suicidal; living with household members who were imprisoned; growing up with one or no parents, parental separation or divorce; emotional neglect; physical neglect. The number of ACE events were later classified as two groups: those who experienced at least four ACEs, and those who experienced less than four ACEs across the nine domains.
Exposure to intimate partner violence (IPV) during pregnancy was recorded if perpetrated by a current husband/ partner during the past 6 months. We used the adapted version from the WHO Multi-country Study on Women’s Health and Domestic Violence Against Women to measure prenatal IPV (Garcia-Moreno et al., 2006). The WHO questionnaire comprises four questions on emotional IPV, six questions on physical IPV and three questions on sexual IPV. Emotional violence was defined as being insulted, humiliated, intimidated or threatened to hurt her or someone she cared for. Physical violence referred to being slapped, pushed, hit, kicked, chocked or threatened. Sexual violence was defined as being physically forced to have sexual intercourse, consenting due to fear of partner’s reaction, or being forced to do a sexual act which she found degrading or humiliating. Pregnant women who experienced any type of prenatal IPV in her lifetime were classified as having experienced at least one type of lifetime IPV. If they experienced at least one type of IPV in the last 6 months, they were considered as IPV exposed during pregnancy.
Self-report stress: The Perceived Stress Scale (PSS) (Cohen et al., 1983) was applied to measure the level of maternal stress. This scale was validated in the Vietnamese population (Dao-Tran et al., 2017). It consists of ten items that measures how stressful certain life situations were rated by respondents during the last month via a 4-point Likert scale: Not at all = 1; Several days = 2; More than half the days = 3; Nearly every day = 4. A mean score of greater than one was defined as perceived stress.
Partner’s characteristics: We recorded age, educational attainment, and employment status based on information provided by the women.
Partner supportiveness: The quality of the mother–father relationship was measured by the partner supportiveness scales (Goldberg and Carlson, 2014). This was a 5-item scale and each item was rated on a 5-point Likert scale: Never = 1, Rarely = 2, Sometimes = 3, Often = 4, Always = 5. A mean score of less than two was defined as low support from partner.
Social support: The Multidimensional Scale of Perceived Social Support (Zimet et al., 1988) was applied to investigate social support. Twelve items measured perceptions of support from three sources: family, friends, and a significant other. The original scale uses a 7-point Likert-type scale, while our questionnaire reduced it to 5-point Likert-type scale: Strongly disagree = 1, disagree = 2; Neutral = 3; agree = 4; Strongly agree = 5. A mean score of less than three was defined as low social support.
Data collection
Before data collection, eight midwives were trained intensively for 3 days regarding the study protocol. One midwife from each ward health center conducted interviews via a tablet assisted face-to-face interview in either a private room in a ward health center, or at a participants’ house if appropriate. Information on IPV during pregnancy were collected using Computer-Assisted Self-Interviewing. The interview data were then submitted directly into a secure web application for building and managing online surveys and databases called “Qualtrics,” with data stored at the University of Cambridge (United Kingdom).
Data analysis and statistical method
Participant characteristics were described using frequency and percentages for categorical data, and mean (SD), for continuous variables. To investigate the factors associated with depression among pregnant women, odds ratios (OR) and 95% confidence intervals (95%CI) were estimated using multivariate logistics models. All analyses were performed using the R program (R Core Team, 2014). Statistical significance was defined as two-tailed p values of less than 0.05.
Ethical considerations
The study was approved by the Ethical Review Committee of Hue University of Medicine and Pharmacy (No H2018/430 dated November 15, 2018). Permission to conduct the study was also obtained from provincial and wards authorities in Thua Thien Hue province, Vietnam. Participants were informed about the study and provided written informed consent prior to the interviews.
Results
General characteristics of the study population
Table 1 describes participant characteristics. The mean age was 29.9 years (SD = 5.0 years), with a range between 19 and 47 years. Most women were between 25and 35 years old (71.3%); finished high school or above (62.0%), had paid work in the last 12 months (71.3%), and lived with the father of the baby (97.3%). Among those participants, 12.7% had perceived low social status. Regarding prenatal characteristics, most of the study participants were multiparous (70.7%), wanted to be pregnant (69.3%) and received at least four antenatal checkups (95.3%). About 30% of pregnant women experienced at least four types of ACEs before 18 years old and 28% perceived stress during the previous month. Twenty-two women (14.7%) reported experiencing at least one type of IPV during the last 6 months. The prevalence of emotional violence was highest (14.0%), followed by physical violence (2.0%) and sexual violence (1.3%). The mean age for the participants’ partners was 33.1 (SD = 6.0). Most of the women’s husbands had paid work in the last 12 months (98%) and more than half of them completed high school or above (57.3%). Overall, 2.7% of women perceived low support from their husband and nearly half of the participants perceived themselves as having low social support (47.3%).
Characteristics of study population (n = 150).

Main findings
Table 2 indicates that the prevalence of moderate to severe depression among study participants was 12.7% (95%CI: 7.3%–18.1%). The mean score of the PHQ-9 was 5.2 (SD = 3.7).
Prevalence of antenatal depression among pregnant women (n = 150).
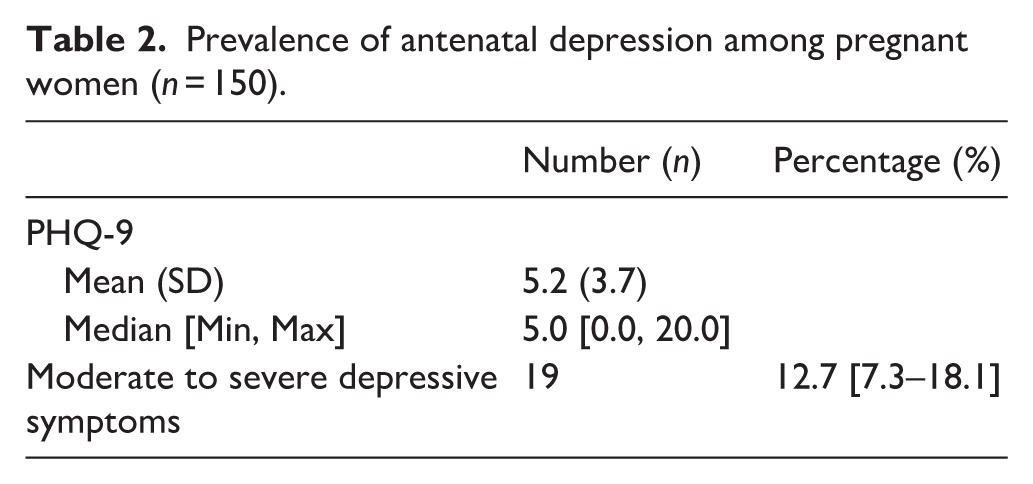
Table 3 presents the factors associated with depressive symptoms amongst pregnant women. Pregnant women who self-reported as being stressed (aOR = 7.62; 95%CI: 2.66–21.81) and had husbands with education attainment of primary school or below (aOR = 4.28; 95%CI: 1.02–17.85) were more likely to experience moderate to severe depression. Perceived low support from partners was significantly associated with the odds of depressive symptoms, but only in univariate analysis (Crude OR = 24.37; 95% CI: 2.39–248.52) not multivariable regression (aOR = 23.62; 95% CI: 0.83–672.53). Our findings did not show any association between depressive symptoms and other factors, such as maternal age, unwanted pregnancy, antenatal check-ups, ACEs, and prenatal IPV, partner’s age, and support from their partner or society.
Factors associated with moderate to severe depressive symptoms among pregnant women (n = 150).

p < 0.05.
Discussion
The strength of this study
This study was one of the first studies on depression among pregnant women in the central region of Vietnam. The main strength of this study was that we used a standardized, validated instrument to measure self reported depressive symptoms (Collier et al., 2020; Dreher et al., 2017; Hinton et al., 2018; Nguyen et al., 2016; Vo et al., 2019). Furthermore, data collectors were well-trained midwives which ensured the quality of data collection. In addition, the application of Qualtrics also reduced missing information compared to use of a paper-based questionnaire.
Main findings
Our study revealed that more than one in ten women experienced moderate to severe depression during the antenatal stages of pregnancy (12.7%). In Vietnam, studies that used the Edinburgh Postnatal Depression Scale (EPDS) to measure antenatal depression reported various findings. A higher prevalence was demonstrated in a study conducted in Hanoi in 2007 (14.7%) (Fisher et al., 2007), which involved 61 pregnant women attending an antenatal clinic. A larger study in Dong Anh, in the North of Vietnam which involved 1274 women in the first and second trimester of pregnancy yielded a lower prevalence of 5.0% (Ngo et al., 2018; Tran et al., 2019). Compared to other countries, our findings reported a lower prevalence of depression during the third trimester than others studies which employed the PHQ-9 scale to measure, which were 26.8% in Ghana and 32.7% in Côte d’lvoire (Bindt et al., 2012), 27.6% in Peru (Yang et al., 2016), 24.9% in Ethiopia (Bitew et al., 2016), and 31.1% in Italy (Venanzio, 2017). Inconsistent prevalence estimates were seen in other studies that used different tools to measure depression besides the PHQ-9 (Bennett et al., 2004; Sawyer et al., 2010; Underwood et al., 2016). There is a disparity in the proportion of women who experienced antenatal depression across countries and within countries. This disparity is likely attributable to macro-level variation in the living conditions of pregnant women, such as the stability of partnership arrangements, access to public health services, and stressful life events, but also methodological differences between studies. Moreover, the high prevalence of antenatal depression in this study suggests the needs for screening for depression during pregnancy at clinical settings in order to reduce the risk of pregnancy outcomes. The effectiveness of screening interventions followed by interventions has been confirmed in other studies (O’Connor et al., 2016; Ponting et al., 2020).
Our study demonstrated that one factor that might be link to antenatal depression was having a partner with a low level of education. Therefore, further interventions should pay attention to families with husbands of low education backgrounds. In this study, lack of support from partners was found to be associated with the odds of experiencing antenatal depression in bivariate analysis but not in the multivariate analysis. The small sample size might be one explanation for this difference. The high correlation between inadequate partner support and a higher risk of experiencing antenatal depression may be explained by gendered role assignment within families in Hue city. In Hue city, it is common for women to take responsibility for child rearing whilst men assume a the role of “breadwinner” and household leader (Dao et al., 2012). This finding is supported by the literature which suggested that having a supportive husband is associated with good maternal mental health during pregnancy and after childbirth (Murray et al., 2015; Vo et al., 2017). Partner supportiveness is protective for pregnant women and aids coping with stressful life events, and is therefore likely to have a significant impact on maternal and infant well-being postpartum (Dayan et al., 2010; Zegeye et al., 2018). A current synthesis of qualitative research reconfirmed partner supportiveness as an important resource for maternal well-being during pregnancy (Staneva et al., 2015b).
This study also identified that stress was associated with higher odds of experiencing depression during pregnancy. This finding was consistent with other studies (Ahmed et al., 2019; Bayrampour et al., 2016). Previous studies have revealed that stress can alter hormonal responses, including increasing the activity of the hypothalamic–pituitary–adrenal axis, and reducing levels of norepinephrine which can trigger maternal depressive symptoms (Moret and Briley, 2011; Pariante, 2014; Seth et al., 2016). This finding suggests that the contents of screening for prenatal mental disorders should cover not only antenatal depression, but also stress, anxiety and other mental disorders if possible, which might enhance a better control for prenatal mental problems.
Findings from our study indicated that gender-based risk factors such as experiencing IPV were not significantly associated with prenatal depression. This might be due to small sample size, which prevents measurement of this association. However, our study indicated that 12% of pregnant women experienced prenatal IPV, which was in line with findings of a systematic review reporting a range of IPV prevalence from 5.9% to 32.5% among 4598 pregnant women in Vietnam (Do et al., 2019). These important findings raise a critical question about how to screen for psychological abuse and violent tactics, and how to remove social barriers and encourage women to disclose experiences of violence. Though domestic violence has become less acceptable among Vietnamese women (Trinh et al., 2016), there is still a perceived social norm that emphasizes women’s responsibility to maintain the harmony and reputation of the family, and to build the “cultural family” and “cultural village” (Schuler et al., 2006) which can prevent disclosures of IPV (Kwiatkowski, 2011; Schuler et al., 2016; Tran et al., 2018a; Vu et al., 2014). Moreover, the influence of Confucian social norms may also inhibit women from disclosing family issues (Tran et al., 2016). In addition, this disparity may be due to the willingness of women to disclose IPV exposure, which is likely to be affected by culture and social norms. A recent review also reported an association between IPV and depression (Fisher et al., 2012; Howard et al., 2014; Tsai et al., 2016). Another study in Vietnam also confirmed this relationship (Fisher et al., 2013). Therefore, screening for IPV during antenatal care remains strongly recommended.
Our study revealed that ACEs were not associated with depression among the study participants. This finding was different from a systematic review which identified a strong effect of multiple ACEs on mental illness, especially antenatal depression (Howell et al., 2017; Hughes et al., 2017; Wajid et al., 2019). However, this finding was supported by a previous study in Hue city among 608 adults. The authors of this study did not find a significant association between ACEs’ exposure and mental disorders (Do, 2019). This unexpected result may be explained by the cultural context in Hue city which is strongly influenced by Confucianism, and where parents may apply corporal punishment and harsh discipline to manage their child’s behavior (Hoang, 2014). In this context, parental physical punishment may be perceived as normative and necessary to educate children (Rudy and Grusec, 2006) rather than being conceptualized as an adverse experience. Another explanations may be recall bias, as some emotional experiences from childhood might not be recalled clearly in adulthood (Fergusson et al., 2000), or respondents were less likely to report ACEs.
Limitations of the study
This study had several limitations. First, the sample size of this pilot study was small and participants were recruited using a non-probabilistic sampling method. The response rate of this study was 76.9% which is considered moderate quality based on EPHPP checklist (Effective Public Health Practice Project, 1998). However, with a small sample size and moderate response rate, caution must be applied, as the findings might not be generalized to the whole Vietnamese population. Data were also collected in the third trimester of pregnancy; thus, our findings may not be generalizable to the first and second trimesters of pregnancy. Second, recall bias and reporting bias may have affected the internal validity of this study. For example, the unwillingness of participants to disclose stigmatizing experiences such as IPV and depression, might have led to an underestimation of their true prevalence. To address this issue, we collected data using Qualtrics, and interviews were administered by well-trained midwives who had close rapport with study participants. Third, some items of the PHQ-9 related to symptoms of pregnancy (i.e. fatigue, poor appetite, difficulty sleeping) may mirror somatic symptoms of depression, which may lead to an overestimation of the proportion or severity of depression. Moreover, the PHQ-9 is a self-reported scale rather than clinical assessment and also not specific to assess depression for perinatal periods like other tools (i.e. the EPDS), which may have led to an under- or overestimation of antenatal depression.
Conclusion
The prevalence of moderate to severe depressive symptoms experienced antenatally was 12.7%. Experiencing stress, having a husband with a low level of education and perceived low levels of support from their husband were found to be significantly associated with higher odds of antenatal depression amongst the study population. However, in the multivariate analysis, husband’s support was no longer a significant factor. These findings suggest the need to screen for depression during pregnancy in central Vietnam. A collaborative care approach between antenatal care services and mental health care practitioners will ensure that women who have symptoms of antenatal depression are managed appropriately. In additional, routine screening of pregnant women in primary care for common perinatal mental disorders could be added to existing antenatal assessments. With appropriate referral systems in place, this could reduce women’s vulnerability to its adverse consequences and help to achieve optimal postnatal outcomes. Health promotion programs should encompass psychosocial health, gender equity and women’s right to be free from violence, especially during pregnancy. Further studies with larger sample size should be considered.
Footnotes
Acknowledgements
We are indebted to the mothers who participated in this study and to Thua Thien Hue provincial People Committee, provincial Department of Labor, Invalids, and Social Affairs, provincial Department of Health and especially staffs from Institute for Community Health Research and Faculty of Public health of Hue University of Medicine and Pharmacy for data collection in fieldwork. Our sincerely thank also goes to Hue University for the partial support under the core research program.
Author contributions
BYLT, TVV, ME conceptualized the research question and participated in the analysis plan. BYLT performed the data analysis and drafted the manuscript. TVV, ME, LM, SVM, LNH, HPD, and THD advised about study design, data collection tools and manuscript contents. All authors read and approved the final draft of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper is an output of the Evidence for Better Lives Foundational Study (EBLS-FS). More information on this study can be found at ![]() . We are grateful for support for the EBLS-FS from: the UK ESRC Impact Acceleration Fund [grant number ES/M500409/1]; the Fondation Botnar, Switzerland [grant number RG92422, research project 6132]; the Jacobs Foundation, Switzerland; the UBS Optimus Foundation, Switzerland; the University of Cambridge School of Social Sciences Research Support Fund, UK; the British Academy, UK; the Consuelo Foundation, the Philippines; and Queensland University of Technology, Australia.
. We are grateful for support for the EBLS-FS from: the UK ESRC Impact Acceleration Fund [grant number ES/M500409/1]; the Fondation Botnar, Switzerland [grant number RG92422, research project 6132]; the Jacobs Foundation, Switzerland; the UBS Optimus Foundation, Switzerland; the University of Cambridge School of Social Sciences Research Support Fund, UK; the British Academy, UK; the Consuelo Foundation, the Philippines; and Queensland University of Technology, Australia.