
Abstract
This study aimed to describe the status of antenatal depression and its associated factors among pregnant women in Vietnam. A cross-sectional study was conducted in four obstetric hospitals in Vietnam from January to September 2019. A total of 1260 pregnant women were interviewed using a structured questionnaire. A Tobit regression model was used to determine factors associated with antenatal depression. Results showed that pregnant women were at high risk of antenatal depression (24.5%). Women with fetus abnormalities and higher education were at higher risk of antenatal depression. We highlighted the need for implementing formal screening programs to early detect antenatal depression.
Introduction
Depression has been increasingly common among pregnant women (Hewitt et al., 2010). It is estimated that 10 percent of women worldwide experienced antenatal depression, and it is higher in developing countries, which accounted for 15.6 percent (Sidhu et al., 2019). Vietnam is among the countries with a high prevalence of antenatal depression, ranging from 12.2 to 29.1 percent (Nhi et al., 2018; Van Ngo et al., 2018).
The etiology of antenatal depression has interested scholars around the world. A systematic review by Biaggi et al. (2016) highlighted multiple factors linked to antenatal depression such as lack of partner/social support, history of abuse/domestic violence, history of mental illness, unintended pregnancy, and present/past pregnancy complications. As a result, prolonged depression during pregnancy may boost the risks of adverse birth outcomes, including premature birth, low birth weight, and delayed development (Fekadu Dadi et al., 2020; Gentile, 2017). Also, it is evident that women who suffered from antenatal depression are more likely to develop postnatal depression (Eastwood et al., 2017; Ogbo et al., 2019).
To respond, the World Health Organization (WHO) launched Global Mental Health Action Plan 2013–2020 to promote mental health with four main objectives: strengthening leadership and governance; providing mental health and social care services at community levels; implementing strategies to promote mental health; and strengthening information systems, evidence, and research (WHO, 2013). Also, in developed countries like the United States, efforts to reduce depression have been made. In 2016, the US Preventive Services Task Force endorsed depression screening among adults, which included pregnant and postpartum women (Siu et al., 2016). In Australia, screening for antenatal depression has been routinely conducted by healthcare providers in most primary care settings (Ogbo et al., 2019).
Meanwhile, antenatal depression has been inadequately detected and treated in Vietnam. Current reproductive care services, such as gestational diabetes, hypertension, eclampsia, infants’ pneumonia, and premature birth, merely focused on the physical health of mother and baby (Ministry of Health, 2016). Depression has not been considered as a chronic disease that involves both physical and social aspects. To the best of our knowledge, there is no formal screening program for depression in perinatal care settings. As a result, the lack of mental health services as a part of standardized prenatal care may boost the prevalence of antenatal depression in the future. As it is essential to pay devoted attention to the mental health of mothers, this study aimed to synthesize the powerful evidence about the prevalence of antenatal depression and its associated factors by recruiting a large sample size in multi-settings. The results enable policymakers and relevant stakeholders to design pragmatic and evidence-based interventions to minimize the prevalence of antenatal depression in Vietnam.
Methods
Study design and setting
We conducted a cross-sectional study on pregnant women who came to the following hospitals for antenatal examination: National Hospital of Obstetrics and Gynecology (Hanoi), Thanh Hoa Obstetrics and Gynecology Hospital (Thanh Hoa), Hue University of Medicine and Pharmacy (Hue), Ho Chi Minh City Medical and Pharmacy University Hospital (Ho Chi Minh) from January 2019 to September 2019—in which Hanoi is in the North, Thanh Hoa and Hue are in the center, and Ho Chi Minh is in the West of Vietnam. We chose these hospitals based on the scale and the representation of diverse sociodemographic characteristics of study subjects.
Study participant
Pregnant women were recruited based on the following criteria: (1) being at least 18 years old; (2) visiting selected hospitals for regular health checkup during a study period; (3) agreeing to enroll in the study; (4) having ability to answer the questionnaire.
Sample size and sampling
In this study, a convenient sampling technique was applied to recruit participants. First, we approached pregnant women when they were waiting for clinical examination and checked for eligibility criteria. All potential women were explained about the study’s purpose, benefits, and responsibilities. Written informed consent was then obtained to confirm their enrollment. The final sample size was 1260 women, which were similarly distributed in four selected hospitals (315 women/hospital) with a response rate of 90 percent.
Measurements
The survey instruments included questions on sociodemographic information, clinical characteristics, and the Edinburgh Postnatal Depression Scale (EPDS). The questionnaire was piloted on 60 pregnant women (15 women/hospital) to evaluate the feasibility, duration, and other adverse events. The questionnaire was then finalized by principal investigators before a full-scale research project. According to the article on sample size estimation for pilot studies, it was recommended that the reasonable minimum sample size for the pilot study was 30 where the purpose is a preliminary survey, and the precision of parameter estimates increases as sample size increases (Johanson and Brooks, 2009).
We collected information about age, gestational age, education, marital status, occupation, monthly personal income, and monthly household income/person.
With regard to clinical characteristics, the important variables were pregnancy times, history of miscarriage, abortion, premature birth and stillbirth, delivery method, time since last pregnancy, birth intention, history of and current gynecological diseases, current comorbidities, abnormal signs of fetus. EPDS is the most frequently validated screening tool for assessing symptoms of perinatal depression (Hewitt et al., 2010). It is a 10-item self-reported questionnaire about feelings experienced over the past weekdays; each question has four levels of response scored 0–3 with a total score ranged from 0 to 30. However, in Vietnam, self-report completion is unfamiliar (Fisher et al., 2004), and therefore, collecting data by individual structured interviews would be more feasible. The cut-off score of EPDS has varied due to cultural variation in antenatal depression expression and different diagnostic criteria across countries (Smith-Nielsen et al., 2018). In this current project, women with EPDS score of 10 or higher were classified as being at risk of antenatal depression. This cut-off point has been used in previous studies in Vietnam (Nhi et al., 2018; Van Ngo et al., 2018).
Data collection
We collected data via face-to-face interviews. All participants were invited to a private room to ensure confidentiality and encourage participants to comfortably discuss about sensitive topics during the interview. We combined several approaches to maximize the quality of data. All interviewers must undergo 1-week intensive training before a pilot. In addition, each hospital had a coordinator who worked closely with local data collectors to timely handle adverse events during data collection.
Data analysis and statistical methods
Raw data were entered by Epidata (version 3.1) and analyzed by Stata (version 15, StataCorp LP, College Station, TX, USA). Descriptive statistics including frequency, percentage, mean, and standard deviation were used to summarize sociodemographic characteristics. The Tobit model was used to determine factors associated with the EPDS score. Tobit was used to estimate linear relationships between variables when there is censoring from below and above in the dependent variable. In this case, EPDS is censored with scores ranging from 0 to 30 so Tobit model would be applicable. We used a stepwise forward selection strategy with the threshold of p < 0.2 to design a reduced regression model. A p value ⩽0.05 was considered statistically significant.
Ethical considerations
Our study proposal was approved by the Institutional Review Board of Hanoi Medical University (Decision no: 06/HMUIRB). Participants’ information was completely confidential and only served for the study purposes. They were free to leave the study at any time without influencing their medical examination. In this study, participants’ involvement was voluntary without any incentives.
Results
Table 1 illustrates sociodemographic characteristics of respondents. In a total of 1260 women, the majority obtained high school education (64.6%) and lived in the urban (73.6%). Of note, most of them lived with a spouse/partner (99.3%) and were employed (92.2%). The mean gestational age was 28.6 (SD = 9.3) years. The average monthly personal income was 7.3 million VND (SD = 7.8), and the average monthly household income/person was 9.8 (SD = 21.9).
Sociodemographic characteristics of respondents.

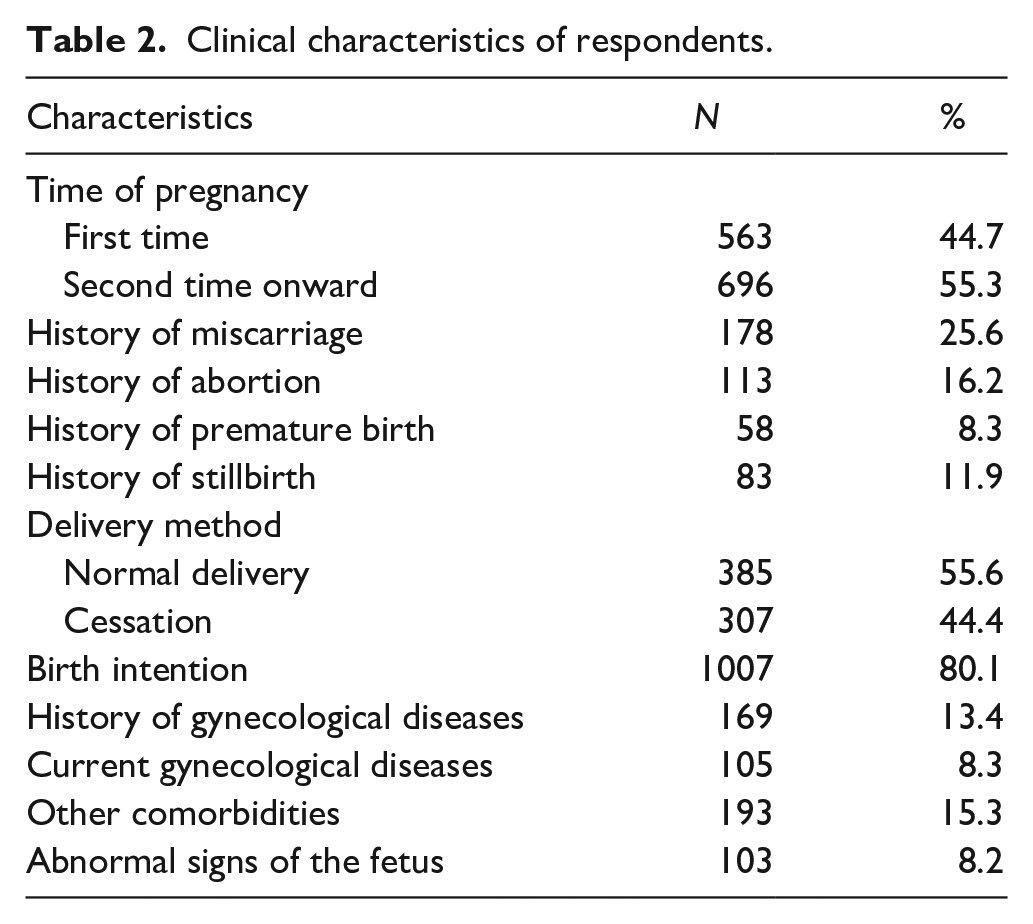
Clinical characteristics of respondents are demonstrated in Table 2, nearly half of women got pregnant for the first time, and more than 80 percent intended to have a baby. Of note, approximately one in four women had been miscarried (25.6%); meanwhile, the history of abortion (16.2%), premature birth (8.3%), stillbirth (11.9%), and gynecological diseases (13.4%) were lower. Women currently suffering from gynecological diseases accounted for 8.3 percent. With regard to birth intention, the majority of respondents intended to have a baby (80.1%). The number of normal deliveries was higher than cessations (55.6% and 44.4%, respectively). Of note, nearly 10 percent of women reported abnormal signs of fetus.
Clinical characteristics of respondents.
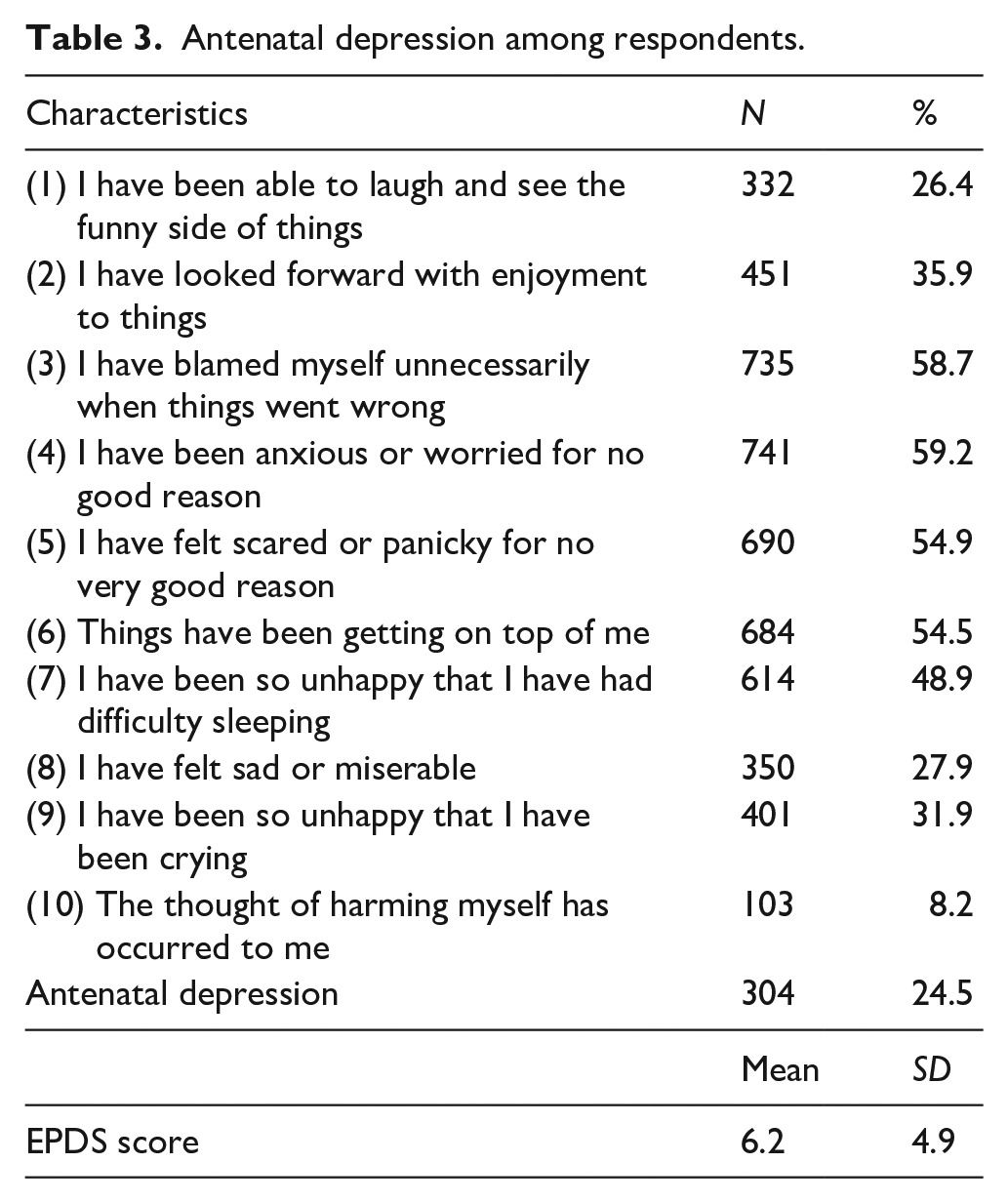
The assessment of antenatal depression symptoms was illustrated in Table 3. At least one in four women subjected to negative experience in most statements of EPDS, excluding self-harm intention with 8.2 percent. Noticeably, nearly 25 percent were at risk of antenatal depression. The average EPDS score was 6.2 (SD = 4.9%).
Antenatal depression among respondents.
The results of regression model were figured in Table 4. There were seven significant predictors chosen from Stepwise analysis: education (high school vs <high school) (p = 0.0002), location (p = 0.0023), abnormal signs of fetus (p = 0.0033), gestational age (p = 0.0139), education (>high school vs high school) (p = 0.0308), history of gynecological diseases (p = 0.0697), history of abortion (p = 0.1619). According to Tobit analysis, while women with older age (Coef = −0.17, 95% confidence interval (CI) = −0.27 to −0.08), late gestational age (Coef = −0.06, 95% CI = −0.11 to −0.02), and lived in the rural (Coef = −1.14, 95% CI = −2.09 to −0.18) were at lower risk of antenatal depression, those with higher education (Coef = 2.74, 95% CI = 1.39–4.08 & Coef = 2.61, 95% CI = 1.41–3.81) and abnormal signs of fetus (Coef = 2, 95% CI = 0.57–3.43) were more likely to suffer from antenatal depression.
Factors associated with antenatal depression.

Note. p < 0.05 was considered statistically significant. EPDS: Edinburgh Postnatal Depression Scale; CI: confidence interval.
p < 0.05; ***p < 0.01.
Discussion
The current study highlighted the status of antenatal depression among women in Vietnam and explored several associated factors. Pregnant women were at high risk of antenatal depression (25%). Older women, later trimester of pregnancy, and rural residence were associated with lower risk of antenatal depression. In contrast, women with higher educational levels and signs of fetal abnormalities are more likely to experience depression.
Our result was much higher than the findings in Western Europeans (8.6%) (Shakeel et al., 2015), Brazil (14.8%) (Handady et al., 2015), Northeast Ethiopia (17.9%) (Belay et al., 2018), Australia (7.0%) (Eastwood et al., 2017) but lower than the findings in Bangladesh (29%) (Nasreen et al., 2011) and in Tanzania (39.5%) (Kaaya et al., 2010). This can explain differences in social cultural variations, sample size, screening tool, and cut-off point. From this figure, we urgently call for public awareness of antenatal depression. Also, we highly recommend the integration of an effective screening tool in primary care settings to early detect depressive symptoms during the pregnancy period. This procedure is routinely used in most primary health care settings in Australia to identify the risks of antenatal depression (Ogbo et al., 2019). Given the fact that EPDS is a widely used screening tool for antenatal depression, future researches should focus on the feasibility of this tool in the Vietnamese population.
In addition, the regression model showed that older women were less likely to suffer from depression. While many studies investigated the relationship between age and depression during pregnancy, the results have been equivocal. Some suggested older women were at higher risk of antenatal depression (Fisher et al., 2013; Weobong et al., 2014), while others endorsed opposite results (Bawahab et al., 2017; Field, 2017). Nevertheless, one possible justification for our results is that older women may have experience with previous births and better preparation for pregnancy. Besides, we supposed that older women can regulate their emotions better in comparison with their counterparts. A study examining the emotional differences in young and older adults by Fernández-Aguilar et al. (2018) suggested that older adults recovered more easily from negative emotions.
Of note, it was reported that those with later trimester of pregnancy had a lower risk of depression. This result is consistent with a systematic search of the PUBMED and PsycINFO databases by Accortt et al. (2015). This is because their bodies may adjust to their hormone levels and they are well adapted to physical and physiological changes. Women rarely suffer from severe problems such as vomiting, poor appetite, fatigue during this period. Of note, rural residence was at lower risk of antenatal depression. A previous study by Habtamu Abebe et al. found that antenatal depression was seven times higher among urban women than the counterparts (Habtamu Belete et al., 2019). We hypothesized that the urban citizens get under pressure from overload work and stay in a competitive environment, which are some reasons why they suffer from depression, especially the pregnant woman.
By contrast, women with higher levels of education were more likely to experience depression. Our result was contradictory to a previous study in China (Hu et al., 2019). We hypothesized that well-educated women tend to have richer social relationships and high positions in society, and being pregnant might hinder job prospects and social relationships. As a result, these women might feel hopeless and unconfident. The future researches should shed light on the link between education and perceived depression during pregnancy so that we could decide the target group for the interventions.
Furthermore, this study also found that fetal abnormalities were associated with antenatal depression, which is consistent with the previous literature (Alijahan et al., 2014; Kaasen et al., 2017). Anxiety and distress may be generated from worrying about the baby’s future and feeling of guilt. Since these groups are more vulnerable to antenatal depression, we propose that the interventions should target women with fetal abnormalities.
Our study is subjected to some limitations. First, this is a cross-sectional study so we could not determine cause and effect. Second, since this study was conducted in hospitals, the results may not be applicable to the general population. Ideally, a community-based research design may increase the generalization.
Conclusion
To sum up, our study suggested that pregnant women perceived high levels of depression. Women with a high level of education and the existence of abnormal signs of a fetus were significant predictors of antenatal depression. One potential strategy would be to implement formal screening programs to early detect psychological disorders as a part of standardized perinatal care. Under the scope of this study, we could not draw the direction between above predictors and antenatal depression. Ideally, we encourage scholars to conduct a longitudinal study in the future, considering that it might take more time and resources. Nevertheless, our study provided evidence on the burden of antenatal depression which helps inform plans and allocate health resources.
Footnotes
Acknowledgements
The authors are grateful to National Hospital of Obstetrics and Gynecology, Thanh Hoa Obstetrics and Gynecology Hospital, Hue University of Medicine and Pharmacy, and Ho Chi Minh City Medical and Pharmacy University Hospital for their permission and support during data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.