
Abstract
A cross-sectional study was conducted among 262 newly admitted patients of a cancer hospital in Vietnam. The Vietnamese version EORTC-30 questionnaire 3.0 was used to interviews patients during the first week after their admission. Lower global quality of life and physical functioning scores were significantly associated with older age, lung and gastrointestinal cancers. Emotional functioning score was lower among female patients as compared to males. Financial difficulty was an important preditor for almost all functional scales. Management of early symptoms, providing early emotional supports and appropriate policies to reduce financial difficulty are important to improve cancer patients’ quality of life.
Introduction
Quality of life is “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns” and addressing quality of life is important as it’s one of the major indicators to measure a person’s well-being (World Health Organization, 1994).
Measuring quality of life in cancer patients is important, and has been integrated into guidelines and also used in clinical trials to indicate treatment outcomes and is used as a prognostic factor in certain situations (Bjordal et al., 1994; Carrillo et al., 2016; Fournier et al., 2016; Rogers, 2016). It is suggested that health-related quality of life is integral to treatment planning, refining treatment protocols, and more personalized follow-up support; should be regularly assessed during patient care; health-related quality of life assessment on an individual patient basis can be helpful to trigger multi-professional support and interventions (Rogers, 2016).
At the moment, there are multiple quality of life assessment scales. These include general tools like EQ-5D questionnaires (EQ-5D-3L, EQ-5D-5L, EQ-5D-V) of the EuroQol Group or the 36-Item Short-Form Health Survey questionnaire (SF-36) of the Boston Health Research Institute in the United States (EORTC), tools designed for all cancer like the EORTC QLQ-C30 of the European Organization for Research and Treatment or tools designed for a specific category of cancer like the EORTC QLQ-H&N35 for head and neck cancer, the EORTC QLQ-BN20 for brain cancer of the EORTC (EORTC – Quality of Life, n.d.).
There have been many research and clinical trials using these tools to describe the quality of life of various patient groups with different demographic backgrounds and clinical characteristics including cancer stages, cancer categories. . . (Beaulac et al., 2002; Bjordal et al., 1994; Curran et al., 1998; Rogers, 2016; Sterba et al., 2016) Regarding the management and treatment of cancer, some studies have found differences in the quality of life of patients after undergoing different therapies. Some studies have found that social support has a positive effect on managing the quality of life of patients (Chun-Sick et al., 2012; Ye et al., 2017).
On newly admitted patients at an early stage, mental support has proven useful in helping improve patients’ quality of life and immune function as well as their ability to cope with the disease (Ye et al., 2017). Therefore, being able to determine the relationship between quality of life and socio-demographic background and clinical characteristics of newly admitted patients would help clinicians and policymakers in providing mental and physical supports that will help with the treatment and management in a very early stage.
Vietnam is among countries, that have been facing an increase of burden from non-communicable diseases, including cancer. During the period from 1990 to 2018, the number of new cancer cases as well as deaths by cancer has almost tripled (Pham et al., 2019). However, knowledge about the quality of life of these patient groups, especially in association with their different clinical and demographic background is limited. This study aims to: (1) examine the quality of life and related functions (physical, role, emotional, social, cognitive) scores of newly admitted patients to a cancer hospital and its association with socio-demographic characteristics and cancer category.
Methods
Study setting
This study was conducted in the Hanoi Oncology hospital, in the capital of Vietnam. The hospital mostly serves the population from Hanoi (about 8 million inhabitants in 2019) and from nearby provinces. The hospital has 615 inpatient beds. In 2019, the hospital had 120,770 patient visits, 55,232 inpatient-day and 65,538 outpatients.
Study design
The study is a cross-sectional study using face to face interviews with the subjects and data extracted from the hospital records.
Study subjects and sample
The sample included 262 patients who were admitted for the first time and less than a week in Hanoi Oncology Hospital in 2019. The study excluded patients who were unable to answer or didn’t agree to participate in the study. The sample size was calculated using the World Health Organization formula to estimate a mean of global quality of life score of 65.8 and a standard deviation of 23.4 according to the reference value from EORTC for cancer patients at stage I and II (EORTC Groups, 2008). A significant level of α equal to 0.05 was used. The required sample size was 49. The sample of 262 allowed comparison of quality of life between groups of patients with different clinical and socio-demographic characteristics.
Instruments and key variables
Patients were interviewed with an instrument consist of two parts: (1) Demographic background: The questionnaire includes name, gender, age, education, occupation, marital status, living areas (urban/rural), people living with, diagnosis status, cancer category. (2) The European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire, 30-item version 3.0 (EORTC QLQ-C30), Vietnamese. The Vietnamese version of this questionnaire was translated and validated by the EORTC Groups. The questionnaire was used for quality of life assessment: includes 30 questions that make up for six multi-item function scales that measure physical, role, social, emotion, cognitive function, and overall quality of life; three multi-item symptoms scales that measure pain, fatigue, nausea and vomiting; six single symptoms items that measure constipation, diarrhea, appetite loss, dyspnea, insomnia and financial consequences of the diseases. The scales and items have scores ranged from 0 to 100. With Function scales, the higher the score the better the function was whereas with Symptoms scales and items, the higher the score, the more was the severity of the symptoms.
Data collection process
The data extracted from hospital records comprised patient ID, name, gender, birth and diagnosis. The interviewers were four medical students in their 2nd, 3rd, and 5th year. They were trained for data collection by the research group before the study. Each day the research team collected information about newly admitted patients of the hospital from the Consultation Department. An interview plan then was made for the next days. Based on the plan, the interviewers visited the patients’ room and planned the interview for each patient after getting informed consent. All interviews were performed within the first week since patients admitted to the hospital. The interviews were done in the patient room or anywhere in the hospital providing that the selected patients felt comfortable and nothing interfered with the interview.
Data management and statistical analysis
Epidata 4.0 was used to store interview data. Completed questionnaires were cleaned before entering to Epidata software. Check file was used to control for logical errors that may occur during data entry and interview. Data on some background information of patients extracted from hospital records then was merged with interview data using the Patient’s ID. STATA version 12 was used to analyze data. The EORTC QLQ-C30 scores were described using mean, standard deviation, median and interquartile range (IQR).
Comparisons of the symptom scale scores between disease groups were done using the Kruskal-Wallis test since the distribution of these variables were not normal distribution.
Tobit regression model was used to examine the association between the global quality of life score, functional scale scores of patients with different sociodemographic and clinical backgrounds. These variables were censored variables from 0 to 100 and were not normally distributed, therefore, the Tobit regression model was used, for it was designed to estimate the linear relationship between variables when the dependent variable were censored. (McDonald and Moffitt, 1980).
Ethical clearance
The research was granted ethical clearance from The Ethical Committee of the Hanoi Oncological hospital. All study subjects were informed about the objective of the study, their right to refuse the interview or stop the interview at any points or skip any questions that may make them uncomfortable.
Results
Sample characteristics
In the 262 patients studied, the female made up for the larger part and accounted for 69.1% of the sample. The common age group was from 45 to 59 years old (43.5%) with the mean age being 49.4 ± 12.0. Most of the patients came from rural areas (72.1%) with the occupation being farmers (44.3%) or self-employed (24.4%). Most patients were married (83.5%) and were living with their family or relatives (96.9%). Regarding education, 42.7% of patients completed secondary education 21.4% of patients completed high school education and 16% of patients went for further education.
Regarding disease category, head and neck cancer accounted for 59.5% of the sample, gastrointestinal cancer was 18.3%, gynecological and breast cancer were 12.6% while lung cancer accounted for 5% and other diagnoses were 3.8% including genital-urinary cancer, skin cancer, and salivary gland cancer (Table 1).
Sample characteristics.

Prevalence of symptoms
Analyzing EORTC QLQ-C30 questionnaire items, 11.8% of patients reported experiencing quite a bit or very much pain and 26.7% reported that pain has interfered with their daily activities. Regarding sleep, 19.5% has struggled quite a bit while 14.5% reported having a lot of difficulties trying to sleep. Regarding mental state, about half of the patients reported feeling tense, worry or depressed and 14.2% of patients felt tense, 20.6% felt worried and 17.1% felt depressed quite a bit or more (Table 2).
Occurrence of symptoms.

Functional and symptoms scores
The median score for Global quality of life was 75 (IQR: 66.7–83.3); for physical functioning was 100 (IQR: 86.7–100), for role functioning was 100 (IQR: 83.3-100), for emotional functioning was 83.3 (IQR: 66.7–100), for cognitive functioning was 100 (IQR:83.3–100) and for social functioning was 100 (IQR:83.3–100).
The median score for Fatigue was 11.11 (IQR: 0–33.33), for Insomnia was 33.33 (IQR: 0–66.67). all five symptoms of Appetite loss, Constipation, Nausea and vomiting, Dyspnea, and Diarrhea had a median score of 0 and the upper value of the interquartile range for those five symptoms was also 0 (Table 3).
Descriptive statistics of EORTC QLQ-C30.

Differences in symptom and functional scores
Using the Kruskal-Wallis test, we found a difference in the score for Dyspnea between the lung cancer group (33.3; IQR: 0–66.7) and other disease categories. Differences in the scores for pain and appetite loss were also found. The pain scores of patients with Gastrointestinal Cancer, Lung Cancer were significantly higher than that among patients with other cancer groups. The pain score of patients with the Head and Neck cancer group was lower than that among patients with the Gynecological and Breast cancer. The score for Appetite loss among patients with Gastrointestinal and Lung Cancer was significantly higher than that among patients with Head and Neck cancer, Gynecological and Breast cancer, and other cancers. No difference between disease groups was found in the score for symptoms of Fatigue, Insomnia, Constipation and Diarrhea (Table 4, data on the test are not shown).
Medians and interquartile ranges of EORTC QLQ-C30 scores by each functional and symptom scale and by type of cancer.

Using Kruskal-Wallis test, the scores for physical functioning and Role functioning of those patients with Head and Neck Cancer were higher than that of patients with Gynecological Cancer and Lung cancer. Social functioning score of patients with Head and Neck cancer was also higher than that of patients with Gynecological cancer. However, no difference in EF and CF scale scores between disease categories was found (Table 4, data on the test are not shown).
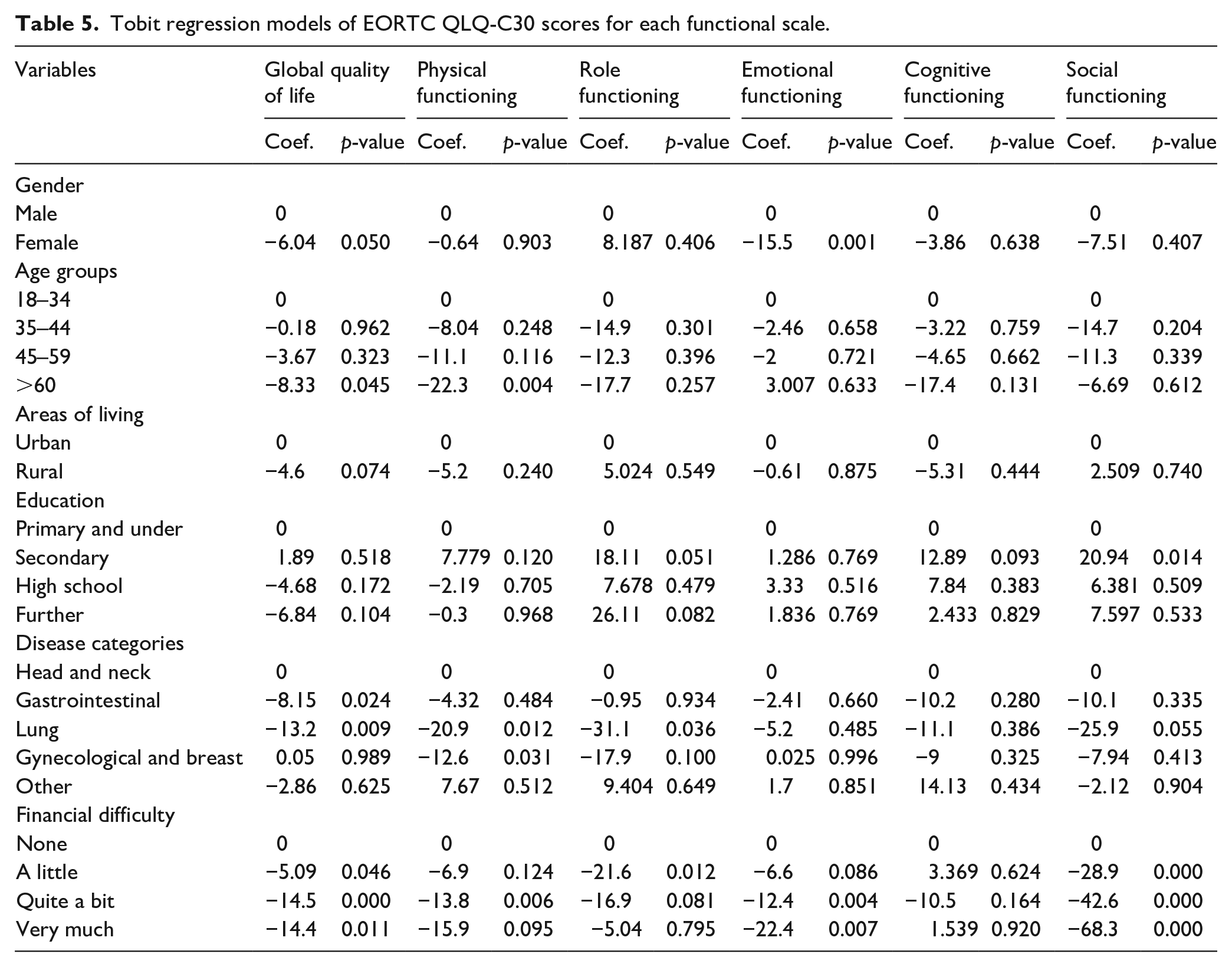
The regression model shows that the score for emotional functioning among female patients was significantly lower than that among male patients. Patients over 60 years old had a lower global quality of life score than other age groups (p < 0.05). Patients with secondary education had the highest Social Functioning score as compared to other patients. Disease category had a significant association with patients’ Global Quality of Life, Physical Functioning and Role Functioning scores. Global Quality of Life scores among patients diagnosed with Gastrointestinal cancer and Lung cancer were lower than that of other patient groups. Physical Functioning scores in patients with Lung cancer and Gynecological and Breast cancer were lower than that of other cancer categories. Lung cancer patients also had lower Role Functioning scores than the rest of the sample. There was no difference in the scores for Cognitive functioning, Emotional functioning and Social functioning between cancer categories. Self-perception of financial difficulty was associated with most of the functions. Patients reported having “quite a bit” and “very much” financial difficulties had significantly lower scores of Global Quality of life, Emotional functioning and Social functioning than that of patients who reported not having any financial difficulties (Table 5).
Tobit regression models of EORTC QLQ-C30 scores for each functional scale.
Discussion
The scores for functioning scales estimated for cancer patients in our study were higher as compared to some similar studies in other settings. The difference is probably because our sample consisted of newly admitted patients, mostly in an early stage of cancer (Bjordal et al., 1994, 2000; EORTC Groups, 2008; Nguyen and Ta, 2017; Tran et al., 2019). Comparing our results with EORTC QLQ-C30 Reference Values for all cancer patients at stage and I-II, a similar pattern was found, with emotional function score being the lowest while other function staying relatively high (EORTC Groups, 2008). Our findings can be interpreted that in newly admitted cancer patients, physical health had not been affected as much as mental health. Specifically, in the early stages of cancer, physical impairment and symptoms are not prevalent while patients could be very worried to receive bad news about their deadly disease. This was also supported by the findings that among newly admitted patients, insomnia and fatigue symptoms were the most common among patients and it’s the same for all disease categories. These findings imply that to help maintain and improve the quality of life of the cancer patients the hospital or health facilities should be serious about care for patients’ emotions at the very early stage of hospital admission.
We found that pain and appetite loss in patients with gastrointestinal and lung cancers were higher compared to patients with other cancers. This is understandable as the symptoms are normally characterized by the disease category.
We found that the quality of life in the patient that was over 60 years old was significantly lower than the younger age group. These findings contradicted the previous two studies on gastrointestinal and breast cancer patients in Vietnam using the EORTC QLQ – C30 questionnaire in 2019, showing that the quality of life is lower among younger people (Ngoc Thi Dang et al., 2019; Tran et al., 2019). Gender was also a factor related to the quality of life in cancer patients, as we found the emotional functioning score among females was lower than males. This share similar result to previous studies conducting on patients at different stages (Laghousi et al., 2019; Schmidt et al., 2005; West et al., 2015). Also, identical to our study, other research in Vietnam (Ngoc Thi Dang et al., 2019; Tran et al., 2019) and other countries (Jacob et al., 2019; Roick et al., 2019) have suggested that financial burden is associated with lower quality of life in cancer patients. This is probably due to the financial burden placing on top of the disease putting more strains on the patient’s mental status.
In terms of disease categories, our research shows that gastrointestinal cancer and lung cancer patients had lower quality of life than head and neck cancer and gynecological and breast cancer patients. This could be explained by the fact that gastrointestinal and lung cancer usually have a worse prognosis (National Cancer Institute, n.d.) and induce more pain than head and neck cancer, leading to treatment and being informed about the stages of the disease affects the patient’s quality of life. This is different from the previously reported results in 768 patients of stage III and IV who received chemotherapy or surgery in Karnataka, that no statistically significant relationship between the types of cancer was found with a quality of life score (Nayak et al., 2017). This could be due to the pain and other symptoms that gastrointestinal cancer and lung cancer patients had to suffer that aren’t found in head and neck cancer patients. It’s clear in our study that patients with lung and gastrointestinal struggled more with pain and appetite loss than head and neck cancer and gynecological/breast cancer patients.
With other factors being studied including: accommodation, education and occupation, our research did not find the relation between these factors and quality of life score calculated according to EORTC QLQ – C30, as a previous study has suggested (Roick et al., 2019).
The study had a limitation regarding sample size, as the number of patient in some cancer categories were rather small and might have caused a lack of statistical significance in the finding of this group. The data collected was from newly admitted patient, therefore at the time of data collection, there were no recorded information on the prognosis and staging of the disease. As a result, the relationship between the prognosis and staging and patients’ quality of life couldn’t be estimated.
Conclusion
Newly admitted patients’ quality of life associate mostly with gender, age, financial status and disease type. Management of early symptoms and providing early emotional supports are suggested to improve patients’ quality of life along with treatment period. Developing the health care system and creating appropriate policies to support those patients with financial difficulty also plays a key role in reducing patients’ burden.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.