
Abstract
Research suggests that stigma impacts help-seeking behaviour and health outcomes for people affected by mental illness. This study compared the attitudes of Australian non-governmental organisation support workers towards people with mental illness with those of other health professionals. Three hundred and seventy four support workers were randomly allocated to answer questions about one of the six vignettes. Results indicated that non-governmental organisation support workers held more positive attitudes towards people with mental illness than those of general practitioners, psychiatrists and psychologists measured in prior research. These results suggest that non-governmental organisations may be a more positive and comfortable entry and referral point for mental health clients.
Keywords
Mental illness accounts for 12.9 per cent of the total disease burden in Australia, putting it third as a broad disease category behind cancer and cardiovascular disease (Institute for Health Metrics and Evaluation, 2013). These rates of mental illness highlight the importance of help-seeking among mental health clients. Unfortunately, stigma interferes with help seeking and impacts mental and physical health outcomes for people affected by mental illness (Corrigan, 2004; Henderson et al., 2013; Pascoe and Richman, 2009; Rusch, 2009). Health professionals, particularly mental health professionals, are a first line of contact for people with mental health difficulties who are seeking help and support in a time of need. Despite their important role, health professionals’ attitudes towards people with mental illness may reinforce the stigma that this group of people experience (Morgan et al., 2016).
The impact of health professionals’ attitudes may be particularly damaging to this vulnerable population (Frese and Davis, 1997; Horsfall et al., 2010). Although a review by Wahl and Aroesty-Cohen (2010) indicates that there is a need for further research on health professionals’ attitudes, particularly among professions where contact with people with mental health issues is high, the non-governmental organisation (NGO) sector has been ignored in studies of health professionals’ attitudes. The extant research on the attitudes of psychologists, psychiatrists and general practitioners (GPs) towards people with mental illnesses has yielded inconsistent results. For example, different programmes of research indicate that these professionals hold the same attitudes as the general public (Mental Health Council of Australia (MHCA), 2011), less positive attitudes than the public (Hugo, 2001; Nordt et al., 2006) and more positive attitudes than the public (Stuber et al., 2014; Lauber et al., 2004). To the best knowledge of the authors, there are no extant studies that include NGO mental health workers in Australia. This is despite the fact that provision of mental health services by psychologists and allied health accounts for 5.3 per cent of government health spending, private psychiatrists account for 3.9 per cent of the budget and GPs account for 3.6 per cent of the budget, whereas NGO funding sits at 6.6 per cent of government mental health spending in 2010–2011 (Department of Health and Ageing, 2013).
The NGO sector has also seen impressive growth worldwide and in Australia. Between 1992 and 2011, expenditure on NGO services as a percentage of state and territory spending, which is the bulk of health spending in Australia, grew from 2.1 per cent to 9.3 per cent of funding (Department of Health and Ageing, 2013). The World Health Organization (2008) suggests that NGOs, described as informal community care, should form the larger part of mental health support services as a part of an integrated strategy to support people with mental health issues. Given the substantial impact that the attitudes of health professionals may have on outcomes for people receiving support, there is a need to compare attitudes between varied health professionals working in the mental health sector. A series of studies undertaken in Melbourne compared the attitudes of large samples of GPs, psychologists, psychiatrists and the general public (Reavley et al., 2014). This study aims to replicate the methods of the Reavley et al. (2014) study with a sample of NGO workers to compare their attitudes to those of the other health professionals reported in that paper.
Methods
Procedure
Three mental health NGOs participated. The total sample of staff working at these organisations was approximately 1900, of whom 374 agreed to participate in this study. One NGO was national, one operated across two of the eastern states of Australia and one operated in one state only. The basic aims of the research were discussed with the senior staff in these organisations, who were instructed not to pass on the aims of the project and did not take part in the research. All persons employed by the organisations were invited to participate in the online survey by a link sent out by the administration staff in the participating organisations so as to preserve anonymity. The study received ethics approval from the Human Research Ethics Committee at the University of Queensland. Approval was also required from the research teams at the participating NGOs. Participants indicated their consent by clicking on a button stating their agreement to participate after reading an information sheet describing the various measures in the study.
Survey questionnaire
The questionnaire was identical to that used in previous research (Reavley et al., 2014) and was presented online (with question order randomised) to participants in their workplace using Qualtrics software (Qualtrics, 2016) from a server based at the University of Queensland.
The vignettes were designed to illustrate six different diagnoses: depression, post-traumatic stress disorder (PTSD), early schizophrenia, chronic schizophrenia, depression with suicidal ideation and social phobia. All vignettes were written to satisfy the diagnostic criteria for the disorders according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) and the International Classification of Diseases – Tenth Revision (ICD-10).
Each participant read only one vignette. As an example, the depression and depression with suicidal ideation vignettes below drew the distinction between the two conditions by accenting the ideation while keeping the vignettes otherwise identical. All vignettes used are available in previously published articles (Jorm et al., 2005; Reavley and Jorm, 2011):
Depression vignette: ‘John is 30 years old. He has been feeling unusually sad and miserable for the last few weeks. Even though he is tired all the time, he has trouble sleeping nearly every night. John doesn’t feel like eating and has lost weight. He can’t keep his mind on his work and puts off making decisions. Even day-to-day tasks seem too much for him. This has come to the attention of his boss, who is concerned about John’s lowered productivity.
Depression with suicidal ideation vignette: ‘John is 30 years old. He has been feeling unusually sad and miserable for the last few weeks. Even though he is tired all the time, he has trouble sleeping nearly every night. John doesn’t feel like eating and has lost weight. He can’t keep his mind on his work and puts off making any decisions. Even day-to-day tasks seem too much for him. This has come to the attention of John’s boss who is concerned about his lowered productivity. John feels he will never be happy again and believes his family would be better off without him. John has been so desperate, he has been thinking of ways to end his life’.
Personal and perceived stigmas were measured using the nine-item scale developed in the 2014 study by Reavley et al. Personal stigma included items such as: ‘People with a problem like John’s could snap out of it if they wanted’. Perceived stigma included items such as: ‘Most people believe that a person with a problem likes John’s could snap out of it if they wanted’ to differentiate it from personally held stigma attitudes. The five-point response scale ranged from strongly agree to strongly disagree with lower scores indicating more positive attitudes. Self-reported desire for social distance was measured using a five-item scale that measured willingness to have social contact with people who have the mental health issue described in the vignette (Link et al., 1999). Participants were asked ‘how willing would you be to’ engage in various types of interactions with the target of the vignette, such as ‘have John marry into your family’ and ‘move next door to John’. The four-point response scale ranged from definitely willing to definitely unwilling with lower values indicating a greater willingness to have social contact.
Statistical analysis
One-way analysis of variance (ANOVA) between NGOs was conducted in SPSS version 23 (SPSS Inc., 2010). The Ryan–Einot–Gabriel–Welsch stepdown was used to adjust for familywise error in post hoc comparisons. Where Levene’s test showed that the variances between groups were unequal the Brown–Forsyth ANOVA was used, and the Tamhane T2 was used for adjusting for familywise error in post hoc comparisons. Comparisons between the data gathered on professional groups in previous research (Reavley et al., 2014) was performed using online t-test calculator (GraphPad, 2017), not assuming equal variances, and corrected for familywise error using the Holm–Bonferroni stepdown procedure. As the Ns in the Reavley et al. paper were given as ranges, the conservative assumption of lowest N for each group was used for the calculations.
Results
There were 420 people who logged into the questionnaire and 374 provided complete responses. The data were collected in mid-2016. The mean overall response rate for completed surveys within the NGOs was 24 per cent while the response rates for completed surveys within each NGO were 22, 24 and 28 per cent. Demographic data for the participants are depicted in Table 1. This gender bias seen below in Table 1 is representative of the female bias in employment in these types of organisations in Australia.
Participants’ age, gender and time working in the sector.

People who had been in the sector less than 1 year had an average duration in the sector of 6 months, and people who had been in the sector more than 1 year had an average duration of 6.6 years.
Professional group differences
Statistical comparisons between the other professions and the general public have been reported elsewhere (Reavley et al., 2014); therefore, the comparisons presented below are comparisons between NGO worker attitudes and those of each of the professions. The overall scales have been split into the factors that were previously identified as those that contributed significantly to the attitudes of both the general public and health professionals (Reavley et al., 2014). That is, people with mental ill health are weak rather than sick or that they are dangerous and unpredictable. Table 2 below shows that the personal attitudes of workers in NGOs were significantly more positive in each domain when compared with those of other mental health professionals. Workers in NGOs in Australia were significantly less likely to think that people with mental ill health were being weak rather than being sick or that they were dangerous or unpredictable as compared to all other health professionals. Furthermore, the social distance scores show that they were more willing to include someone with mental ill health in their lives.
Personal attitudes.

GP: general practitioner; NGO: non-governmental organisation.
As average scores (standard deviations) out of 5 – lower values relate to more positive attitudes.
Significantly different from NGO workers p < 0.05.
Significantly different from NGO workers p < 0.01.
Interestingly, although the NGO workers had the most positive attitudes towards people with mental health issues, their perceptions of other people’s attitudes, their perceived stigma, were significantly less positive than those of other health professionals (Table 3).
Perceived stigma, perceptions of the attitudes of others.

GP: general practitioner; NGO: non-governmental organisation.
As mean (standard deviations) out of 5 – lower values relate to more positive perceptions.
Significantly different from NGO workers p < 0.001.
Gender differences
The current sample of NGO workers has a higher proportion of females than in the comparison research project (Reavley et al., 2014), and in both data sets, the attitudes of females were more positive than males. It would, therefore, be instructive to investigate male and female attitudes to determine whether the more positive attitudes of NGO workers are due merely to having a higher proportion of females in the study.
Table 4 shows that even when the attitudes of males in NGOs are compared with the overall attitudes of each profession, personal attitudes are significantly more positive with the exception of psychiatrists’ perceptions of being weak rather than having a sickness and the social distance of psychologists.
Comparison of male NGO workers’ personal attitudes to each health profession.

NGO: non-governmental organisation; GP: general practitioner.
Values are given as mean (standard deviations).
p < 0.05; **p < 0.001.
Within NGO worker differences
The data across the three NGOs were remarkably consistent, with the only difference being that workers in one NGO thought that people with mental health issues were less dangerous than did workers in the other two NGOs (Table 5).
Comparison of attitudes in different NGOs towards people with mental health issues.
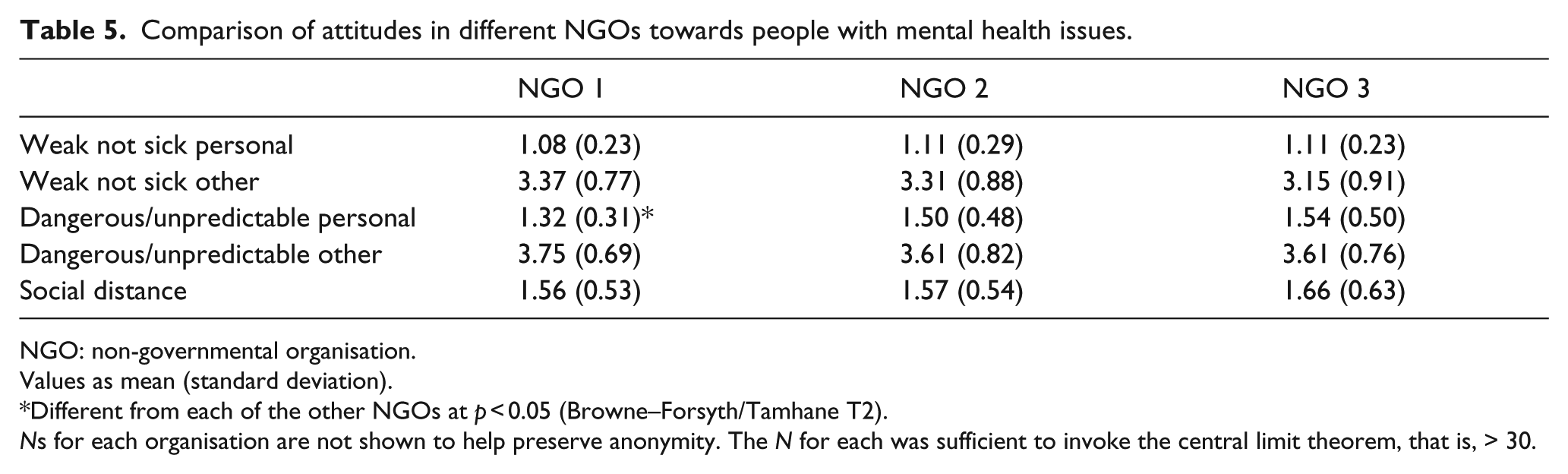
NGO: non-governmental organisation.
Values as mean (standard deviation).
Different from each of the other NGOs at p < 0.05 (Browne–Forsyth/Tamhane T2).
Ns for each organisation are not shown to help preserve anonymity. The N for each was sufficient to invoke the central limit theorem, that is, > 30.
Comparison of the perceptions of people classified in the diagnostic categories of the six vignettes shows that there were no differences between diagnoses in the personal perceptions of the person being weak rather than sick (Table 6). However, when thinking of the perceptions of others, NGO workers thought that others would see people with chronic schizophrenia as being sick more so than weak, whereas social phobia would be seen more as weakness. In regard to dangerousness, NGO workers thought that people with either form of schizophrenia were more dangerous and unpredictable than those with other diagnoses, with the exception of depression with suicidal ideation. Personal perceptions of depression with suicidal ideation were not significantly different from any of the other categories. NGO workers thought that others would see people with either of the schizophrenia diagnoses as being more dangerous or unpredictable. Chronic schizophrenia generated the highest social distance, whereas social distance from people with early schizophrenia was not significantly different from other diagnostic categories with the exception of PTSD which had the lowest social distance.
Attitudes and diagnostic categories.
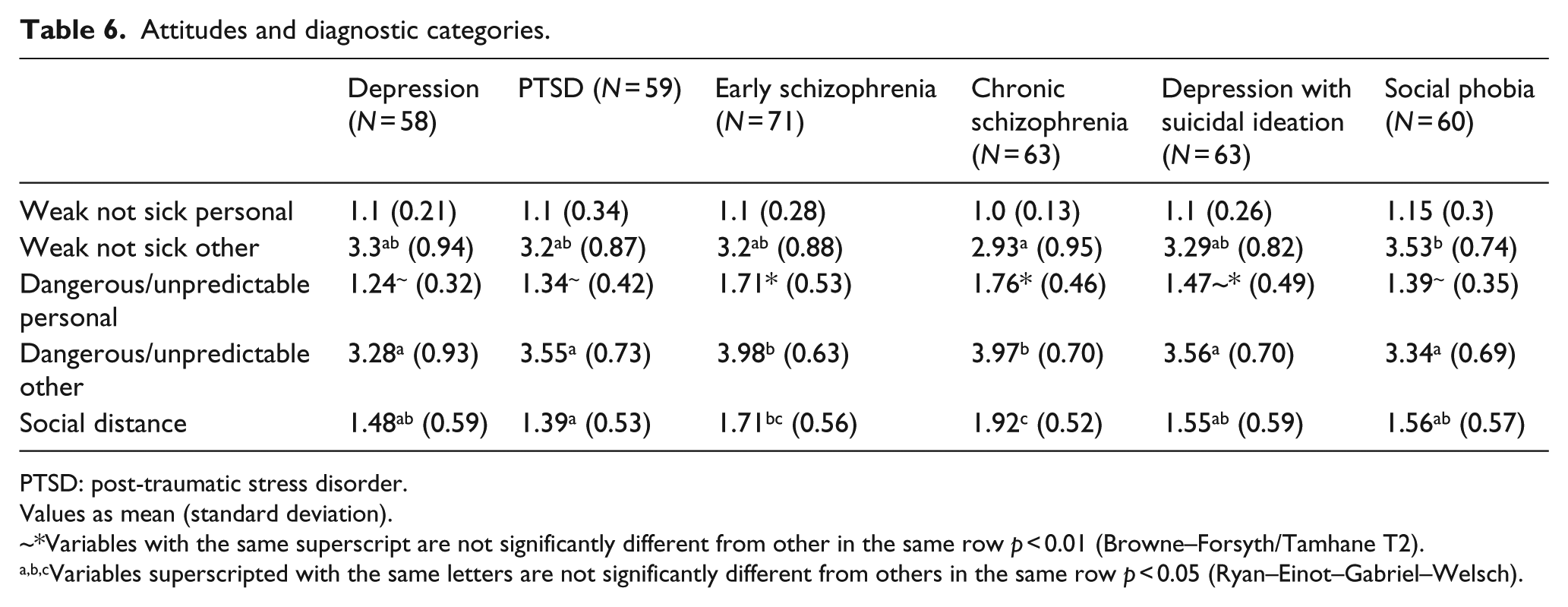
PTSD: post-traumatic stress disorder.
Values as mean (standard deviation).
~*Variables with the same superscript are not significantly different from other in the same row p < 0.01 (Browne–Forsyth/Tamhane T2).
a,b,cVariables superscripted with the same letters are not significantly different from others in the same row p < 0.05 (Ryan–Einot–Gabriel–Welsch).
Discussion
The results of this research indicate that the attitudes of NGO workers towards people with mental health issues were more positive than those of the comparison mental health professionals. This finding emerges even when the NGO comparison group is limited to male NGO workers compared to the combined data of the male and female samples of other professional groups. The more positive attitudes among NGO staff may make NGOs more accessible than some of the other services and hence may encourage people to engage with care and to continue receiving appropriate support. Currently, NGOs both receive referrals from, and refer people to, public and private mental health professionals. NGO employees work alongside GPs, psychiatrists, psychologists, public and private mental health systems to support the physical and mental health of their mutual clients/patients and can thus act as a conduit for referrals and ongoing support for physical and mental health of people affected by mental illness.
One of the most comparable results in this study is social distance. Previous research has found no difference in the desire for social distance between health professionals and the public (Jorm and Oh, 2009; Reavley et al., 2014). The consistent finding, both in the overall scores and in the breakdown between males and females, is that NGO workers have less of a desire for social distance compared to both other health professionals and the general public. This may be due to the high number of people working in these organisations who identify as someone with lived experience of mental illness. Two of the three organisations that participated include the percentage of people working in the organisation that identify as having lived experience of mental ill health in their annual reports. In one organisation, the percentage was 50, and in the other, the percentage was 70, figures that are greater than the proportion of the population that have lifetime experience of mental illness or substance use disorder in the Australian Bureau of Statistics (ABS) surveys of 1997 and 2007 (ABS, 2008).
To the best of these authors’ knowledge, there is no extant research on the proportion of psychologists, psychiatrists and GPs who identify as having lived experience of mental ill health. But the introduction of a peer workforce and lower educational barriers to entry suggests that the proportions may be higher in NGOs compared to those professions. In addition, Bateman and Smith (2011) state that there is considerable lived experience among workers in Australian mental health NGOs. Relatedly, NGO workers thought that others held more stigmatising attitudes towards people with mental ill health than other health professionals or the general public. Previous research has suggested that health professionals are more reluctant to accept an illness in them than in a patient as evidenced by the higher scores on perceived stigma compared with personal stigma (Adams et al., 2010; Reavley et al., 2014). However, a significant percentage of NGO workers have already acknowledged that they have a lived experience of mental illness; therefore, the reason for this more negative perception of others attitudes cannot be due to non-acceptance of their own illness. It may be that this group has direct personal experience of stigma from others and that this has negatively coloured their perceptions of others’ attitudes. It would be an interesting area for future research to establish why perceptions of the attitudes of other are so negative among these NGO workers.
The overall less positive attitudes among NGO workers towards people with schizophrenia are consistent with earlier research (Reavley et al., 2014). However, the perceived attitudes of people with either early or chronic schizophrenia were not seen as being more likely to be weak than others with a mental illness, except between chronic schizophrenia and social phobia. In relation to the perceived attitudes of others, NGO workers believe that others perceive little difference between the mental illnesses included in the vignettes, but also believe that others have much less positive attitudes towards people with mental ill health than those of NGO workers.
As with any research, there are limitations to this study that should be kept in mind when interpreting these results. The comparisons with other health professionals rely on data published in previous research, using the N, mean values and standard deviations to make the direct comparisons that have been reported here.
The original data were published in 2014, which raises the possibility of a change in attitudes from health professionals in this intervening period. Previously published work that has assessed attitudes across a time span has not reported attitude changes across such a short time span (Reavley et al., 2014; Wahl and Aroesty-Cohen, 2010), but this possibility cannot be ruled out. In addition, only three NGOs participated in this research, and they may not be representative of other Australian NGOs. Nonetheless, there was a remarkable consistency of data obtained across the three organisations, suggesting that they may provide a reasonably representative sample.
Conclusion
Mental health NGO workers, be they male or female, have generally more positive attitudes towards people with mental illness than was found among other health professionals and the general public. These data suggest that these organisations are well placed to be a low stigma point of entry to mental health support as well as a low-cost ongoing support and referral system for people living in the community with mental ill health. Research assessing why these attitudinal differences exist and why NGO support workers have more positive attitudes towards their clients than health professionals in other sectors would be valuable. Such findings may inform education strategies to promote positive attitude towards clients with mental health issues among staff outside of the NGO sector.
Supplemental Material
Supplemental material for Attitudes of people working in mental health non-governmental organisations in Australia: A comparison with other mental health professionals
Supplemental material, Supplemental_material for Attitudes of people working in mental health non-governmental organisations in Australia: A comparison with other mental health professionals by Grenville Rose, Courtney von Hippel, Loren Brener and Bill von Hippel in Health Psychology Open
Footnotes
Acknowledgements
The authors acknowledge the contribution of the participating NGOs. The corresponding author thanks the other authors for donating their time and expertise to this project.
Author’s note
Author Grenville Rose is also affiliated to Flourish Australia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was partially funded by an Australian Research Council Linkage Grant - The role of implicit identity and implicit beliefs in recovery from mental illness.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.