
Abstract
Purpose of review:
The purpose of this commentary is to address the challenges of implementing the evolving Kidney Disease Improving Global Outcomes (KDIGO) glomerulonephritis (GN) guidelines within the Canadian health care context, highlighting barriers to adoption of the guidelines and discussing contextual issues unique to Canada.
Sources of information:
The KDIGO 2021 guidelines with 2024 updates in antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis and lupus nephritis, as well as the 2025 updated guideline for immunoglobulin A (IgA) nephropathy.
Methods:
A Canadian Society of Nephrology (CSN) working group with expertise in GN was formed, representing nephrologists, pathologists, pharmacists, and patient partners with geographic representation from across Canada. Recommendations and practice points were reviewed by member surveys, with discussions to reach consensus and frame the commentary.
Key findings:
The commentary highlights diagnostic investigations, the role of immune treatments for primary glomerular diseases, and the growing role of conservative kidney therapies.
Limitations:
A review of the quality of evidence was not undertaken. Implementation and uptake of the guidelines will vary across each province given drug availability and cost.
Implications:
The commentary aims to provide tailored guidance to enhance the care of Canadians living with glomerular disease.
Introduction
Reflective of the rapidly emerging molecular research underpinning our understanding of the pathophysiology of glomerular diseases as well as the multitude of clinical trials in the field, Kidney Disease Improving Global Outcomes (KDIGO) released new guidelines in 2021 1 with subsequent chapters already receiving updates, including antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis, 2 lupus nephritis (LN), 3 and most recently immunoglobulin A (IgA) nephropathy. 4 Despite this expanded knowledge for diagnostic testing as well as the many new, but often expensive treatment options, implementation and uptake of the guidelines will vary globally given drug availability as well as cost implications.
Canada is unique among countries with universal health care, in that it does not have a universal national pharmacare program. Instead, drug coverage varies significantly by province or territory. Furthermore, Canada’s small market share and proximity to the United States serves to disincentivize pharmaceutical companies from seeking Health Canada Approval. As such, the Canadian Society of Nephrology (CSN) has again established a Canadian glomerulonephritis (GN) working group to create a guideline commentary, 5 highlighting barriers to guideline uptake given our local contextual factors while providing guidance aimed to improve the care of Canadians living with glomerular diseases.
Methods
The 2021 KDIGO GN Guideline consists of evidence-based recommendations formulated using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) 6 approach and practice points. First included in these guidelines, practice points represent expert consensus statements to provide guidance when there is insufficient or inconclusive evidence to warrant a recommendation, but do not include an explicit discussion about benefits, harms, patient values, or resource considerations, and are not graded for strength of evidence. 7 To provide context to the 2021 KDIGO GN guideline relevant to the Canadian kidney community, a commentary was developed and written using the recently updated CSN methods. 8
The Canadian Society of Nephrology’s Clinical Practice Guideline Committee (CSN-CPGC) appointed a multidisciplinary working group, consisting of a chair and co-chair, adult nephrologists with clinical and content expertise, renal pathologists, renal pharmacists, and people with lived experience. Consistent with CSN policy, consideration was given to geographical representation from across Canada and other equity factors, such as age, gender, and career stage. The 2021 KDIGO GN guidelines were reviewed except for Chapter 4 (Pediatric Nephrotic Syndrome) and Chapter 7 (Infection-Related Glomerulonephritis). In addition, the 2024 ANCA-associated vasculitis 2 and LN 3 updates were reviewed, as well as the 2025 IgA nephropathy (IgAN) guidelines’ update. 4
The working group systematically reviewed all recommendations and practice points, identifying those to be included in the commentary. To determine inclusion, the following criteria were considered: (1) high yield for clinical practice, (2) resource constraints (frequently excluded from guideline development), (3) potential for targeted knowledge translation activities relevant to the local, regional, and national context, (4) factors specific to delivery of health care in Canada, and (5) recommendations wherein the working group questioned the strength of the evidence (Table 1).
Discussion Criteria for Recommendations.
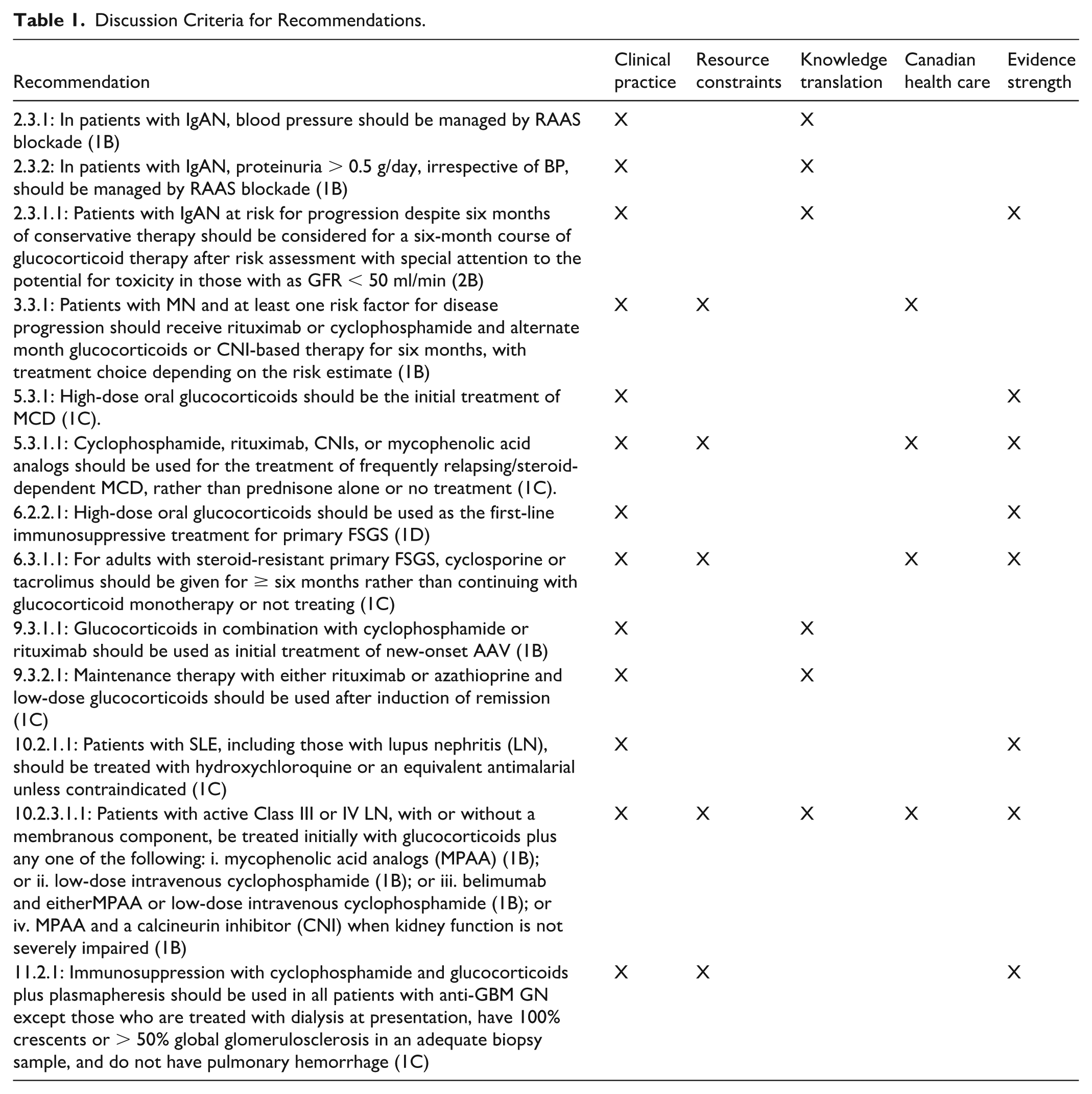
Prior to the first working group meeting, each member completed a survey, indicating whether each recommendation: (1) required discussion regarding the supporting evidence, (2) required discussion for Canadian implications, and (3) did not require further discussion. The survey also allowed participants to abstain from responding and included an accompanying free text field for each question. Responses from the survey, including free text comments, were collated and disseminated in advance of the first working group meeting, and were used to frame meeting discussions. With respect to practice points, chapters were assigned to working group members tasked to identify those requiring discussion. These identified practice points were also presented and discussed at working group meetings. While the group did not perform or conduct systematic reviews to inform the commentary, any new studies since the publication of the guideline were incorporated into the discussion per the working group discretion. The chairs provided a chapter template to all working group members in advance who then utilized meeting minutes and survey results to draft their assigned chapters.
Dissemination of this commentary will be done through a variety of approaches, including publication in peer-reviewed nephrology journals as well as posting of the full document on partner websites, including the CSN, Kidney Foundation of Canada, Ontario Renal Agency, BC Renal Agency, and Can-SOLVE along with relevant commentaries in appropriate local, national, and international forums.
Chapter 1: General Principals for the Management of Glomerular Disease
Given that immunosuppression may be required for months to years, the same care that is afforded our transplant population should be applied to those with glomerular diseases, including cardiovascular risk reduction strategies to treat concomitant hypertension and hyperlipidemia (Practice Points 1.5.1 and 1.6.4), maintenance of vaccination schedules (Practice Point 1.8.1), age-appropriate cancer screening, as well as attention to reproductive health with coordinated multidisciplinary pregnancy planning (Practice Point 1.15.1).
The benefit from SGLT-2i is from time accrued while on the medication, and therefore, risk likely outweighs benefit in those receiving induction immunosuppression regimens and SGLT-2i should not be concomitantly prescribed in this patient population. The priority for treatment of glomerular diseases remains addressing the underlying immunological issue. This is an important consideration if there is a “masked” decrease in proteinuria, which may exclude patients from clinical trials or disease-targeted treatment. Given the current data, it may be reasonable, however, to consider SGLT-2i for patients with glomerular diseases with residual proteinuria or those with chronic kidney disease (CKD) regardless of the degree of proteinuria who are on no or stable maintenance immunosuppression regimens.
Both dapagliflozin and empagliflozin are approved by Health Canada for non-diabetic CKD. Although a recent cross-sectional study from Alberta noted many adults with CKD would derive both cardiac and renal benefits with SGLT-2i, 11 many did not have access for various reasons, including being of a low socio-economic class. Hopefully the availability of generic options will limit cost as a reason for decreased uptake of SGLT-2i.
Chapter 2: Immunoglobulin A Nephropathy
An updated 2025 guideline for the treatment of IgAN 4 highlighted the role of novel therapies that impact disease pathogenesis (eg, nefecon) and progression (eg, sparsentan). Given the emergence of more targeted and less toxic therapies, the importance of prioritizing treatment of the underlying immunologic and inflammatory components was emphasized. To date, none of the novel therapies that have received full or conditional approval in the United States are approved or funded in Canada (ie, nefecon, sparsentan, and iptacopan). Looking to the future, immunosuppression is an explosive area of research in the IgAN space with ongoing phase 3 trials investigating complement inhibitors as well as anti-A Proliferating-Inducing Ligand (APRIL) and B-cell Activating Factor (BAFF) therapies. Unfortunately, the high costs of these medications will certainly be barriers to use in Canada, requiring ongoing physician and patient advocacy.
Since the publication of the KDIGO guidelines, sub-analysis of DAPA-CKD10 (Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease) and Empagliflozin in Patients with Chronic Kidney Disease (EMPA-Kidney 17 ) have suggested that SGLT-2i therapy may also provide significant benefit as it pertains to reducing the progression of kidney disease in patients with IgAN. This represents an area requiring further research in terms of the sequencing of therapy and how to interpret SGLT-2i-mediated proteinuria reduction when assessing risk, as well as making decisions about immunotherapy. Importantly, SGLT-2i therapy is not disease modifying and should not replace immunotherapy but should instead augment supportive therapy in addition to RAAS blockade.
Recently, phase 3 data have been published investigating the utilization of the dual endothelin angiotensin receptor antagonist (DEARA), sparsentan, 18 which resulted in proteinuria reduction, but provided only modest benefit on the rate of estimated glomerular filtration decline. Similarly, the selective endothelin receptor agonist (SERA), atrasentan demonstrated proteinuria reduction in IgAN, but estimated glomerular filtration rate (eGFR) data are yet to be reported. 19 Both medications carry a significant financial cost relative to SGLT-2i. Furthermore, whether there is added benefit as well as an acceptable risk profile when used with SGLT-2i remains unknown. In Canada, we presently cannot access these medications, but efforts are ongoing to make these medications more readily available for select patient populations.
At the time of publication of the 2021 guidelines, the complete Therapeutic Evaluation of Steroids in IgA Nephropathy Global (TESTING) trial, including the lower-dose protocol results, was not known. The trial suggested that lower-dose steroids do improve renal outcomes as effectively as higher-dose steroids, while reducing the risk of adverse events relative to higher doses. 21 Given the balance of benefit compared with harm in patients who are at high risk of progression, the lower-dose glucocorticoid regimen is a logical first choice for those patients deemed to require immunosuppression. The KDIGO guidelines suggested that more caution should be applied in those with glomerular filtration rates (GFRs) < 50 ml/min. However, those patients are also at a high risk to develop end-stage kidney disease (ESKD) and were enrolled in the TESTING trial (GFR > 20 ml/min in the high-dose protocol and 30 ml/min in the low-dose protocol). 21 Consideration of only one factor, such as GFR, in a disease as complex as IgAN, can lead to errors in decision making, as it pertains to treatment. In Canada, the adoption of lower-dose glucocorticoid regimens may present challenges. Due to the clinical equipoise that existed in this therapeutic domain, altering clinical inertia will be difficult. The addition of newer agents in the realm of supportive care, such as SGLT-2i, will further blur these lines, due to their anti-proteinuric effects. Also, application of these protocols to Indigenous populations and other equity deserving populations, who may be at higher risk of adverse events, is not well studied. Finally, there is no established immune therapy in patients who relapse or do not respond to glucocorticoid therapy. Acknowledging the above, glucocorticoids remain the only available immunosuppressive therapy in Canada with robust evidence.
In the recent KDIGO IgAN guideline revision, 4 it was suggested that targeted-release oral budesonide could be considered as an alternative to oral prednisone. The Efficacy and Safety of Nefecon in Patients with Primary IgA Nephropathy (NEFIgARD) trial was recently published along with 2-year durability results,22,23 demonstrating that targeted-release oral budesonide was effective at lowering proteinuria and reducing the progression of kidney disease as compared with standard of care, and was associated with less side-effects than high-dose systemic glucocorticoids. However, the relative tolerability of targeted-release budesonide compared with the low-dose steroid protocol from the TESTING trial remains unknown, and presently, targeted-release oral budesonide is not available in Canada.
Chapter 3: Membranous Nephropathy
Typically, the side-effect profile becomes the determining factor for the choice of first-line immunosuppression. For moderate- and high-risk MN patients, the preferred adverse effect profile of CNIs and rituximab may favor their use over cyclophosphamide-based regimens (eg, fertility and malignancy risk). 27 The oral dosing of CNIs may make treatment initiation easier, while vascular disease or a rising serum creatinine may be a contraindication for their use. In addition, data from the MENTOR trial, which compared rituximab with CNIs, suggested patients with very elevated serum anti-phospholipase A2 receptor (PLA2R) levels may respond better to rituximab, suggesting biomarkers may also guide the initial choice of immunosuppression. 28 Finally, higher relapse rates upon CNI discontinuation may be reason for concern for moderate-high risk patients with MN. 29 As the quality of remission determines risk factors for relapse (high residual proteinuria and low serum albumin), additional treatment may be needed with CNI therapy to reduce the risk of relapse. Combination therapy of CNI and rituximab has been described. 30 One possible advantage of this combination therapy is the faster initial proteinuria reduction with CNI therapy and the sustained reduction with rituximab. 31 Although combination therapy with rituximab and cyclophosphamide is being investigated, there remain concerns about the adverse side-effect profile and larger studies are needed for efficacy.32,33 Unfortunately, there is significant provincial variability with respect to rituximab coverage for MN, 34 limiting accessibility when rituximab is deemed the most appropriate immunosuppressive option. Based on the current guidelines, it is no longer appropriate for a patient to have to fail cyclophosphamide to gain access to rituximab.
Beyond diagnosis quantifying the anti-PLA2R level can guide treatment decisions. For example, a serum anti-PLA2R > 50 RU/ml is also listed as a feature of high-risk MN, while Barbour et al 36 have evaluated the change in serum anti-PLA2R at three and six months from baseline as a predictor of treatment response. The KDIGO working group identified changes in serum titers as a research priority to aid in risk assessment and treatment decisions. If further data continue to support changes in serum anti-PLA2R titers as correlating with disease progression, this biomarker will become an even more valuable tool in disease management.
Although this serological investigation is becoming more widely available outside of academic centers in Canada, the test is not available in all provinces, and the costs are not covered in any province. In addition, there is variability in the type of testing being used (eg, quantitative vs semi-quantitative), limiting its utilization.
Chapter 5: Minimal Change Disease
When choosing therapy for patients with contraindications to corticosteroids, clinicians should carefully consider patient demographics and medication safety profiles with particular attention given to baseline myelosuppression, propensity for malignancy, reproductive plans, and ability to monitor blood work. There are no studies to date elucidating a superior steroid-sparing agent for the treatment of MCD, but CNIs and mycophenolate mofetil (MMF) generally have a favorable safety profile compared with cyclophosphamide. Given the recent discovery of anti-nephrin antibodies, a marker of disease activity, among a sizable proportion of patients with MCD, including 44% of adults, 42 there is growing evidence to support the use of rituximab in the initial management of MCD in adults. Rituximab has been shown to clear anti-nephrin antibodies, resulting in sustained remission, 42 but further study is required to compare efficacy with that of glucocorticoids.43,44
Up to 33% of patients with MCD will become frequent relapsers (FRs) (> three per year) or steroid dependent (SD). Cyclophosphamide, rituximab, CNIs, and mycophenolic acid analogs (MPAAs) have been used as glucocorticoid-sparing agents to treat FR/SD MCD. These agents are supported by low-quality evidence for efficacy and questionable long-term benefit in adults with MCD. Furthermore, there is limited evidence to favor one drug class over another. However, the avoidance of prolonged or repeated glucocorticoid-associated morbidity supports their use. Unfortunately, the choice of therapy for FR/SD (frequently relapsing/steroid-dependent) MCD is impacted by accessibility and cost for non-glucocorticoid drugs in Canada, some of which are not covered by publicly funded provincial health care plans or restricted in access with rituximab typically being the drug most difficult to access despite the noted benefits in this patient population. Further studies, including economic analyses of maintenance rituximab given every six months compared with daily oral therapy of combination immunosuppression, should be prioritized to ensure similar access and coverage across all Canadian provinces.
Chapter 6: Focal and Segmental Glomerulosclerosis
Chapter 8: Immunoglobulin- and Complement-Mediated Glomerular Diseases With a Membranoproliferative Glomerulonephritis Pattern of Injury
Nephritic factors are autoantibodies that bind to and stabilize C3 or C5 convertases and are thought to be present in most patients with C3G.68,69 Of these, C3 nephritic factor is the most prevalent. Nephritic factors also define the site of complement dysregulation and may suggest treatment response to complement inhibitors. Additional autoantibodies to complement proteins, including anti-factor B autoantibodies, have been reported particularly in response to infections.70,71 The degree of terminal complement pathway activation has also been associated with worse renal prognosis in C3G/IC-MPGN. 72
Despite their ability to provide important insights into disease mechanisms that may alter treatment choices, these emerging complement assays are not Health Canada approved for clinical use, and are therefore not routinely available in most Canadian centers and provinces. Funding to send blood samples out of province or out of country is also not consistently available. Furthermore, some provinces rely on pharmaceutical industry funding for complement genetic testing and functional assays, which creates inconsistent access to these tests and the potential for a conflict of interest. Given IC-MPGN and C3G are rare diseases, expert Canadian centers for complement testing should be developed for clinical use and research, and these assays should be funded by provincial health authorities.
Chapter 9: Antineutrophil Cytoplasmic Antibody-Associated Vasculitis
The utility of maintenance therapy in patients with renal-limited disease who remain dialysis-dependent is dependent on the individual patient. Vasculitis is a systemic disease, and extrarenal manifestations may occur in dialysis-dependent patients. The relapse risk is lower in patients with ESKD than patients not on dialysis, and infectious complications are higher, making individual decision-making important. 92 Individual factors that may be important in weighing the risks versus benefits of maintenance therapy include the vasculitis subtype, comorbid conditions, and feasibility and timing of future transplantation.
Chapter 10: Lupus Nephritis
The guidelines also detailed recommendations for risk attenuation strategies spanning infection prevention to bone health, all critical in patients on prolonged courses of immunosuppression, and at times neglected. Proteinuria reduction using RAAS blockade, BP control, and avoiding a high-sodium diet was emphasized. Presently, the role of SGLT2 inhibitors to prevent renal progression is unclear, but is reasonable to consider in those on stable maintenance immunosuppression who are at less risk for AKI, pending further studies. 97
Although the clinical trials introduced belimumab and CNIs immediately at induction, the optimal timing of initiation is still debated. Post hoc studies have also highlighted that belimumab may not be effective in nephrotic patients or those with class 5 disease. 98 Furthermore, some patients may not require these add-on therapies to achieve complete remission, thereby exposing them to possible medication side effects. One alternative to adding on the new therapies to standard of care at induction is to consider triple therapy in the presence of clinical risk factors for poor kidney outcomes (eg, African or Hispanic ancestry, decreased eGFR, relapsing disease, or high-grade proteinuria). If add-on therapy is not started upfront, early assessment of treatment response at two to three months should be pursued to reassess the decision. 99
This add-on approach to therapy, however, is complicated by the Canadian funding structure and drug availability. Criteria for the use of belimumab, for example, directly mirror the inclusion criteria of the clinical trial. It is recommended that belimumab only be used within 60 days of initiating induction therapy even though other patient populations, such as those with relapsing disease could benefit from it as a steroid-sparing agent. Furthermore, it is only funded for one year thereafter, requiring yearly review by the funding agency to determine whether treatment can be continued, which is not aligned with the recommendation for 2.5 years of induction therapy.
Also contrary to the guidelines, voclosporin is not presently available in Canada, and therefore, cannot be used as first-line therapy. The benefits of voclosporin include no requirement for drug monitoring, no interaction with MPAA and less metabolic and electrolyte impacts. Tacrolimus and cyclosporine mandate drug levels, which are not universally reimbursed across Canada. Furthermore, some provinces also have restrictions on available CNI options. In Ontario, for example, cyclosporine is funded as first-line therapy. Through inhibition of enterohepatic recirculation, cyclosporine can reduce MPAA levels by 40%, which can result in undertreatment of severe disease. 100 Monitoring of MPAA levels is also typically not available in Canada potentially having a significant impact on patient outcomes. Therefore where available, tacrolimus is preferred pending approval of voclosporin. More recently, the phase 3 REGENCY trial investigated the addition of obinutuzumab to MMF versus placebo for patients with proliferative LN. 101 A greater rate of complete renal response was seen in the obinutuzumab group versus placebo (46.4% vs 33.1%). Presently, Health Canada approval is pending.
Canadian physicians are also reminded to use reduced-dose glucocorticoid regimens for initial treatment of LN. The AURA-LV trial involved participants receiving prednisone 0.4 mg/kg/day with a taper over three months to 2.5 mg/day. 102 This has led to an update for both KDIGO and the European League Against Rheumatism (EULAR) guidelines on corticosteroid dosing, 99 mirroring recommendations for other glomerular diseases wherein prolonged courses of high-dose steroids result in excessive risk. Although steroid pulses remain appropriate for patients presenting acutely with aggressive disease, subsequent oral steroid doses have been lowered and courses abbreviated.
Chapter 11: Anti-Glomerular Basement Membrane Disease
In addition to plasmapheresis, the mainstay of management for anti-GBM disease remains glucocorticoids and cyclophosphamide. Although rituximab instead of cyclophosphamide has been described, its use should be reserved for those with refractory anti-GBM disease (<10% of cases) given the low quality of evidence.103-105 However, in patients who decline treatment with cyclophosphamide or wherein there is a contraindication (eg, due to fertility concerns), rituximab in conjunction with corticosteroids and plasmapheresis can be offered. Alternatives to plasmapheresis, such as imlifidase, an IgG-degrading endopeptidase able to clear anti-GBM antibodies from the circulation, may help reduce barriers to plasmapheresis in the future. 106
Not present in the 2012 guidelines were recommendations with respect to the futility of treatment when there is advanced glomerulosclerosis. The 2021 guidelines note that the risks associated with immunosuppression may outweigh the benefit in those without pulmonary hemorrhage on dialysis at presentation with 100% crescents or >50% global glomerulosclerosis. Other histological features consistent with severe scarring such as interstitial fibrosis and tubular atrophy are not considered. In a study of 174 patients with anti-GBM disease, the renal risk score originally developed for ANCA-associated vasculitis was applied to predict kidney outcomes. 107 The study demonstrated that stratifying patients according to two key factors, the need for renal replacement therapy at diagnosis and the percentage of normal glomeruli in kidney biopsy (using a 10% cutoff), provided superior outcome prediction, creating four distinct risk groups with 36-month renal survival rates ranging from 96.4% (best prognosis: no dialysis needed, ≥10% normal glomeruli) to 14.1% (worst prognosis: dialysis needed, <10% normal glomeruli). As the quality of evidence supporting this recommendation is very low, a shared decision-making approach is necessary. Furthermore, plans for future kidney transplantation may also guide immunosuppressive therapies, as the recurrence rate is up to 50% in those with detectable anti-GBM antibodies compared with very low rates (<3%) in those with undetectable antibody titers at the time of transplantation. 108 With the evolution of glomerular disease registries, higher-quality risk estimation for both the prognosis of anti-GBM disease and the associated harms of treatment may help clinical decision-making even in the absence of further trials.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251409874 – Supplemental material for Canadian Society of Nephrology Commentary on the Evolving Kidney Disease Improving Global Outcomes Adult Glomerulonephritis Guidelines
Supplemental material, sj-docx-1-cjk-10.1177_20543581251409874 for Canadian Society of Nephrology Commentary on the Evolving Kidney Disease Improving Global Outcomes Adult Glomerulonephritis Guidelines by Arenn Jauhal, Reem Mustafa, Anna Mathew, Louis Girard, Sean Barbour, Bhanu Prasad, Lavanya Bathini, Penelope Poyah, Stephan Troyanov, Ratna Samanta, Jocelyn Garland, Todd Fairhead, Michael Walsh, Heather Reich, Shih-Han Huang, Jenny Ng, Judith Marin and Michelle Hladunewich in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
This working group would like to acknowledge the CSN for promoting the formation of this commentary and for providing administrative support and funding. The authors would also like to thank Dr Rohan John and Dr Virginie Royal for pathology input as well as acknowledge the valuable contributions of our patient partners, Marilyn Clemens and Kevin Allen.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Materials
Not applicable.
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the working group along with publlication fees were provided by the Canadian Society of Nephrology.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.