
Abstract
Purpose of program:
In 2021, the Canadian Society of Nephrology (CSN) sent a needs assessment survey to nephrology residents, fellows, and program directors that identified a significant gap in Quality Improvement (QI) training. In response, the CSN’s Quality Improvement and Implementation Science (CSN-QUIS) committee launched a national nephrology fellow QI curriculum in 2022.
Methods:
The program integrates online learning with interactive virtual didactic sessions, including participation in a longitudinal QI project that is presented at the CSN Annual General Meeting (CSN AGM).
Key findings:
Since inception, the program has expanded to 13 nephrology training programs, including both adult and pediatric sites. Forty-one fellows have completed the full curriculum, with 76 trainees having completed at least one year and presented work at the CSN AGM. Feedback from participants has been overwhelmingly positive, particularly regarding the interactive format, real-world applicability, and national networking opportunities. Continuous fine-tuning of the curriculum itself has occurred in parallel with refinements made to session content, project scheduling, and presentation format based on learner input.
Limitations:
Barriers such as limited local QI mentorship have been mitigated through virtual faculty pairing, and resources such as software access and publication support have been provided to encourage project success.
Implications:
Herein, we report the development and initial experience of this national initiative, demonstrating that a structured, collaborative, and distributed QI curriculum is feasible, effective, and scalable across Canada.
Introduction
The Canadian Society of Nephrology’s Quality Improvement and Implementation Science (CSN-QUIS) committee was created to promote quality assurance and quality improvement (QI) within all aspects of nephrology care in Canada. With a national mandate, its core objectives are to: (1) establish and monitor key nephrology performance indicators, (2) increase the number and quality of nephrology QI projects completed, and (3) build QI capacity by educating nephrology health care providers on QI methodology. 1 In 2021, the Canadian Society of Nephrology sent a needs assessment survey to nephrology residents, fellows, and program directors to better understand the extent to which QI methodology was taught in local curriculums (Table 1). The results of the survey highlighted a significant gap; although 62% of respondents had never completed a QI project, 92% of respondents felt that QI education within nephrology training was either important or very important, and 96% of respondents expressed interest in participating in a web-based nephrology QI educational curriculum.
Selected Results of the CSN-QUIS Educational Stakeholder Survey Describing Quality Improvement Experience in Residency Training (Total Respondents = 24).

To help meet this educational need, the CSN-QUIS committee created a national nephrology fellow QI curriculum consisting of didactic and project-based learning. The national model was chosen to help ensure individuals with QI expertise were available to all participating sites, to help disseminate best practices in nephrology and QI across the country, and to create opportunities for networking, collaboration, and early-career development. The nephrology fellow QI curriculum was delivered to eight Royal College of Physicians and Surgeons of Canada Nephrology training programs beginning in 2022 and has since expanded to include 13 different adult and pediatric programs nationwide (Figure 1). This article describes the structure of the nephrology fellow QI curriculum and highlights the experiences and projects undertaken by Canadian nephrology trainees over the initial three years of this initiative.
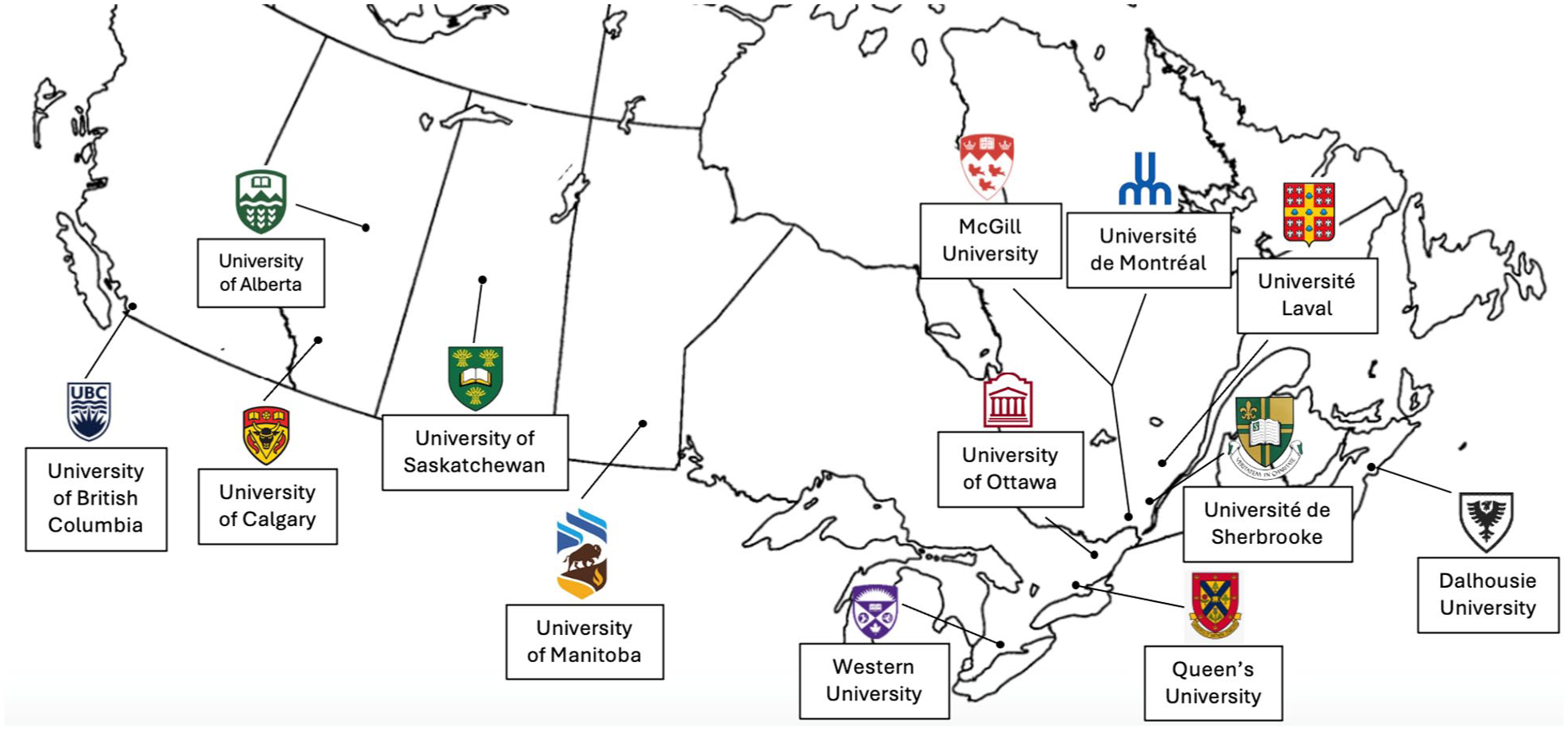
Location and names of participating nephrology training programs.
Nephrology Fellow QI Curriculum
The current CSN-QUIS nephrology fellows QI curriculum includes a combination of online modules, didactic sessions, participation in a QI initiative, and a project presentation to peers and colleagues at the Canadian Society of Nephrology Annual General Meeting (Figure 2).

CSN-QUIS nephrology fellow QI curriculum.
The initial phase of the curriculum focuses on teaching core QI methodology principles using available resources from the Institute for Healthcare Improvement (IHI) Open School for Hospitals and Healthcare systems. 2 The IHI Open School has been incorporated into medical training in the United States of America through the Association of American Medical Colleges and Accreditation Council for Graduate Medical Education. 3 It offers interactive online modules combining case studies, videos and featured articles to guide learners through a variety of QI courses. Specifically, the CSN-QUIS curriculum includes four IHI courses to be completed prior to a complementary virtual didactic session: QI 101: Fundamentals of Improvement, QI 102: The Model for Improvement: Your Engine for Change, QI 103: Measuring for Improvement and QI 104: Putting it all Together: How Quality Improvement Works in Real Health Care Settings.
At each didactic session, core principles from pre-assigned IHI modules are reviewed by session facilitators. Key concepts are reinforced using real world examples from prior nephrology QI projects and trainees have the opportunity to ask questions to help solidify their understanding of the content and resolve any misunderstanding they may have. Didactic sessions are designed to be interactive and often utilize virtual breakout rooms where smaller groups of trainees are provided an opportunity to apply these QI concepts in real time using a case-based approach with guidance from facilitators. Each session is facilitated by a different group of nephrologists to help ensure program sustainability through workload distribution and to provide trainees exposure to a wide variety of staff with different teaching styles and expertise. Facilitators have additional training in QI methodology and deliver sessions virtually from different sites nationwide to leverage available QI expertise and to help facilitate pan Canadian trainee involvement. The current didactic curriculum consists of six sessions, each approximately 1.5 hours in duration, delivered over an 18-month period via an online platform. Sessions are often incorporated into training program academic half-days, and held at 14:00 hours Eastern Standard Time to ensure trainees in different time zones are able to attend. The interactive nature of sessions provides trainees the opportunity to practice applying skills learned in the IHI modules such as generating and refining QI project ideas, creating aim statements, developing meaningful measures, constructing process maps and interpreting run and control charts. During each of these sessions, trainees are encouraged to further refine their own “Fellows Project,” which is a real-world QI project worked on during their Royal College training program that runs in parallel to their coursework. Projects from prior cohorts are often highlighted to reinforce key concepts, to celebrate success of prior years, and to help inspire trainees with their own projects. Throughout the curriculum, participating sites are asked to present a project update to the entire cohort following one of the didactic sessions to encourage sharing of ideas and to help troubleshoot project problems leading up to the abstract submission at the CSN Annual General Meeting (AGM).
Nephrology Fellow Projects
The incorporation of a longitudinal QI project into the CSN-QUIS curriculum provides an opportunity for trainees to gain real world QI experience through the application of knowledge gained throughout the curriculum. The structure of this project has been purposely designed to be flexible. Trainees have the option to work individually, or as a team, and can develop a novel QI project or take over a local QI project in progress. This provides ample opportunities for trainees to gain hands on experience and practice applying the skills learned during their didactic sessions. Participating sites receive formative feedback on their project at the CSN AGM in their PGY-four year (the halfway mark of the program). This consists of verbal feedback from peers and QI faculty following their project presentation as well as written comments from faculty. Written feedback is provided using a structured template focused on components of QI methodology (project background, aim statement, root cause analysis, change ideas etc.) to ensure that participants have incorporated elements from the IHI and didactic sessions appropriately.
Since its inception in 2022, three fellow cohorts have participated in the fellow project portion of the curriculum. Projects tend to vary in subject matter and scope as they aim to improve local care gaps, which may differ between institutions. Most projects focus on a quality issue relating to chronic kidney disease, kidney transplant, home dialysis, or in center hemodialysis and the CSN AGM presentations help ensure that QI work in these domains has the potential to spread nationally. A summary of past projects grouped by themes is included in Table 2. Below, we will describe one project in greater detail to provide an example of the type of work completed during the curriculum and show how projects are shaped by iterative feedback.
CSN-QUIS Fellows Projects Themes (2022, 2023, and 2024 Cohorts).

Note. SGLT2 = Sodium/glucose cotransporter 2; AVF = Arteriovenous fistula; GI = gastrointestinal; HD = hemodialysis, EMR = electronic medical record; ESA = erythropoietin stimulating agents; ACEi = angiotensin converting enzyme inhibitor, ARB = angiotensin II receptor blocker.
Project Example: Dialysis Modality Education for Chronic HD Patients who Start in Hospital
Step 1: identification of a problem—IHI courses QI 101/102
A group of trainees in Halifax, Nova Scotia identified that patients who start in-center hemodialysis (HD) acutely, as part of an admission, and go on to require chronic outpatient hemodialysis often receive substandard modality education compared with individuals who start dialysis through renal clinic. The trainees conducted a chart audit consisting of 20 patients who started in-center HD acutely during a hospital admission and had ongoing HD requirement at the time of discharge. Of these patients, 13 remained on dialysis three months post discharge and over half had no documented modality discussion.
Step 2: aim statement—IHI QI 101/102
Following discussions with multidisciplinary members of the nephrology care team, the trainees generated the following aim statement: To ensure that >90% of patients who start HD acutely during a hospital admission have a documented home modality discussion on the provincial nephrology EMR within two months of being deemed “chronic in-center patients” (requiring dialysis for at least three months on a continuous basis).
Step 3: root cause analysis—IHI QI 103
The trainees conducted a root cause analysis using an Ishikawa diagram to identify multiple patient, provider, environmental, and system factors potentially contributing to the lack of documented dialysis modality discussions. Relevant stakeholders, including the home dialysis modality education nurse, were included in the root cause analysis. Based on faculty feedback, the team decided to focus on underlying system factors including poor documentation of modality discussion in the electronic medical record (EMR), and the lack of a formal mechanism to alert the modality education nurse when a new start hemodialysis patient was discharged from hospital.
Step 4: national project update/change idea generation—IHI QI 103
The trainees presented their project progress to their peers and QI faculty at the CSN AGM which included their project background, root cause analysis, and a number of potential change ideas. Based on feedback from that session, the trainees decided to create a novel “Modality Selection Form” that could be integrated into their center’s hemodialysis start package to flag the modality selection nurse if a patient without contraindications to home therapies who started hemodialysis acutely during an admission was discharged from hospital requiring outpatient hemodialysis. The trainees actioned additional suggestions from the CSN AGM presentation by incorporating multidisciplinary feedback in the design of their modality selection form and using process measures to audit form completion rates.
Step 5: PDSA to test change ideas—IHI QI 104
After multiple iterations, the trainees finalized their one-page “Modality Selection Form.” It was incorporated into their program’s dialysis start package following an educational divisional round designed to provide education about the initiative. The form was to be completed by the discharging nephrologist and faxed to the modality selection nurses as part of the discharge process to help identify new inpatient dialysis starts who would benefit from modality education in the outpatient unit should they not recover renal function and go on to require chronic dialysis.
Between April 2024 and June 2025, the “Modality Selection Form” has been used 38 times for patients requiring an acute inpatient hemodialysis start who remained dialysis dependent at discharge. Eight of these patients had renal recovery post discharge, and eight patients passed away soon after discharge or were felt to have an absolute contraindication to home dialysis. Twenty of the remaining 22 patients (91%) had a documented modality discussion by the modality selection nurse and two of these patients ultimately switched to a home therapy. Barriers with respect to data capture and documentation associated with the project are current targets for improvement as accurately capturing the total number of acute hemodialysis starts requiring dialysis at the time of discharge has been difficult and most modality nurse conversations were captured in a handwritten logbook as opposed to the provincial EMR.
CSN Support and Program Outcomes
Recognizing that involvement in the CSN-QUIS nephrology fellow QI curriculum requires prioritization of time for scholarly activity during a busy clinical fellowship, trainees are incentivized to participate in the curriculum through a variety of mechanisms. This includes a certificate of completion from the CSN at the end of the program and an opportunity to receive an IHI certificate in quality and safety through the completion of additional IHI modules. Trainees are also eligible for an award if their project wins the best QI abstract at the CSN AGM. To help promote QI project development, trainees are provided with free access to QI Macros software and should a completed fellow project be accepted for publication in the Canadian Journal of Kidney Health and Disease, authorship fees are covered by the CSN-QUIS committee. Finally, trainees can satisfy their Royal College of Physicians and Surgeons of Canada’s (RCPSC) Core of Discipline Entrustable Professional Activity (EPA) 22 “Identifying and analyzing patient-level and/or system-level healthcare delivery for the purposes of quality assurance or improvement” through completion of the program as it requires trainees to identify gaps in patient care and develop ideas for improvement. Furthermore, program directors are incentivized to enroll their trainees in the CSN-QUIS curriculum as it helps fulfill the RCPSC’s QI accreditation mandate.
In total, 41 nephrology fellows have completed the full two-year curriculum and received their CSN-QUIS Certificates of Completion, and eight abstracts have been submitted to the CSN AGM. Completed projects are also logged online in the CSN-QUIS QI repository (https://www.csnscn.ca/quis/repository/view-the-repository) which is a comprehensive list of ongoing and completed nephrology related QI projects in Canada. At present, there are 26 nephrology related QI projects logged in the repository.
Program Feedback and Lessons Learned
Three fellow cohorts (n = 76) have completed at least the first year of the curriculum and have presented project updates at the CSN AGM, with a fourth cohort starting in July 2025 consisting of 13 programs. Feedback on the curriculum is sought regularly via evaluation of each session and has been instrumental in helping the CSN-QUIS modify the program to better meet learner needs. In general, the didactic sessions have received very positive feedback. Most presentations have been evaluated as “very good” to “excellent” overall, “about right” in duration, with speaker knowledge rated as “very good” to “excellent.” Written feedback regarding session strengths consistently highlights the collaboration between sites and application of QI theory with real world examples. This is shown through comments such as “information [is] presented in a structured and detailed manner [with] good examples provided,” “digestible, actionable sections then put into practice in breakout sessions,” “I liked the practicality in the presentation coupled with real life examples,” “nice to hear progress of other groups and feedback” and “[good] interaction with other sites, hearing about other programs ideas for QI projects.”
The didactic sessions have evolved over time based on learner feedback. They were initially designed to complement the IHI Open School QI curriculum and to provide more in-depth explanation of QI methodology and theory. Over time, and in keeping with trainee feedback, sessions evolved to focus less on didactic teaching and more on interactive elements supporting the application of knowledge attained from the IHI Open School. Strategies used to foster discussion, improve interactivity, and reinforce key learning principles included polling the audience, supervised breakout rooms, and case study analysis.
Fellow project updates have also evolved with subsequent cohorts. Initially, project updates were slotted at the end of each first-year didactic lecture. Participating programs were pre-assigned a presentation date and asked to provide a project update to facilitate project feedback and troubleshooting. Having the project update scheduled early in the curriculum may have served as motivation for trainees to start their project early and ensure they had ample time to complete it over their two years. While trainees appreciated the opportunity to receive feedback on their projects, not all site projects were developed enough by the time of their presentation to receive, or action, the feedback. To remedy this, project updates were scheduled at the midway point of the curriculum (CSN AGM) and beyond in subsequent cohorts to allow trainees enough time to develop a sound QI knowledge base and ensure they are underway in their project prior to presenting it to the group for feedback and troubleshooting. Another change made to the fellow project relates to project selection. In the inaugural year, fellow projects were chosen according to a pre-selected theme (e.g., cost reduction, improving patient experience etc.) with hopes of enhancing learning through the comparison of different sites’ work in a similar field. However, based on feedback, pre-selected project themes were removed from the curriculum to afford trainees the opportunity to choose a quality improvement project based on personal interest and local need to increase trainee engagement and the likelihood of completion.
The CSN annual general meeting presentation component has also been adapted over the last three years based on trainee and facilitator feedback. Strengths of the CSN AGM session identified by trainees included the provision of a safe space for trainees to present to peers, robust conversation pertaining to project improvement, and the exposure to challenges faced by other programs to assist with personal project troubleshooting. Following the inaugural CSN AGM session, trainee feedback identified that the most beneficial component of the session was peer to peer discussion and feedback from QI experts. To build on this strength, a one-page project outline form and structured Power Point slide deck was created for use at subsequent CSN AGMs. The project outline form is circulated prior to the presentation and helps facilitate a more interactive question and answer period. The structured slide deck is used to keep presentations on schedule to ensure adequate time for peer discussion. Finally, a structured faculty feedback form has recently been introduced to ensure all presenters receive high quality feedback on key aspects of their project (aim statement, root cause analysis, change ideas, measures, implementation and sustainability etc.).
While improvements have been made throughout the curriculum, a number of challenges persist. Lack of access to a local QI champion at every participating site can make it difficult for local trainees to received regular project feedback outside of the scheduled didactic sessions and CSN AGM. This barrier has been mitigated to a degree by virtually linking trainees without a site mentor to an expert faculty; however, it remains difficult to engage sites without local QI faculty. Highlighting and communicating local project successes has also been challenging as previously there was not an ideal medium for this. However, the newly created QI repository should help address this barrier by providing a storage database for previously completed QI projects that is easily accessible to CSN members. Additionally, trainees are encouraged and supported to publish their QI work in peer reviewed literature to help increase awareness. Finally, as the number of sites participating in the program grows, it has become increasingly difficult to incorporate all of the site project updates within the limited number of didactic sessions. If growth continues at its current rate a new project update format may be required.
Conclusion
The CSN-QUIS committee has successfully developed and implemented a national comprehensive QI curriculum for Canadian Nephrology trainees. This innovative program integrates a combination of online modules, interactive didactic sessions, participation in “real world” QI initiatives, and peer-to-peer teaching. Over the past three years, the CSN-QUIS nephrology fellow QI curriculum has been well received by trainees and faculty alike. Through continuous feedback with iterative refinements, the curriculum has been adapted to ensure it meets trainee learning needs, encourages meaningful participation and highlights trainee scholarly activity at the national level. The program also highlights best clinical practices across the country and how different programs can overcome similar QI challenges. As QI becomes increasingly integrated in medical education, additional changes will likely be required on an ongoing basis as learner needs evolve. Throughout this process, a number of barriers to delivering QI education in a distributed fashion have been identified and overcome through a collaborative approach using strategies which could be adapted by other international nephrology program and Canadian non-nephrology programs looking to strengthen QI education efforts (Table 3).
Strategies Used to Overcome Barriers to Establishing Formal QI Curriculum in Canadian Nephrology Training.
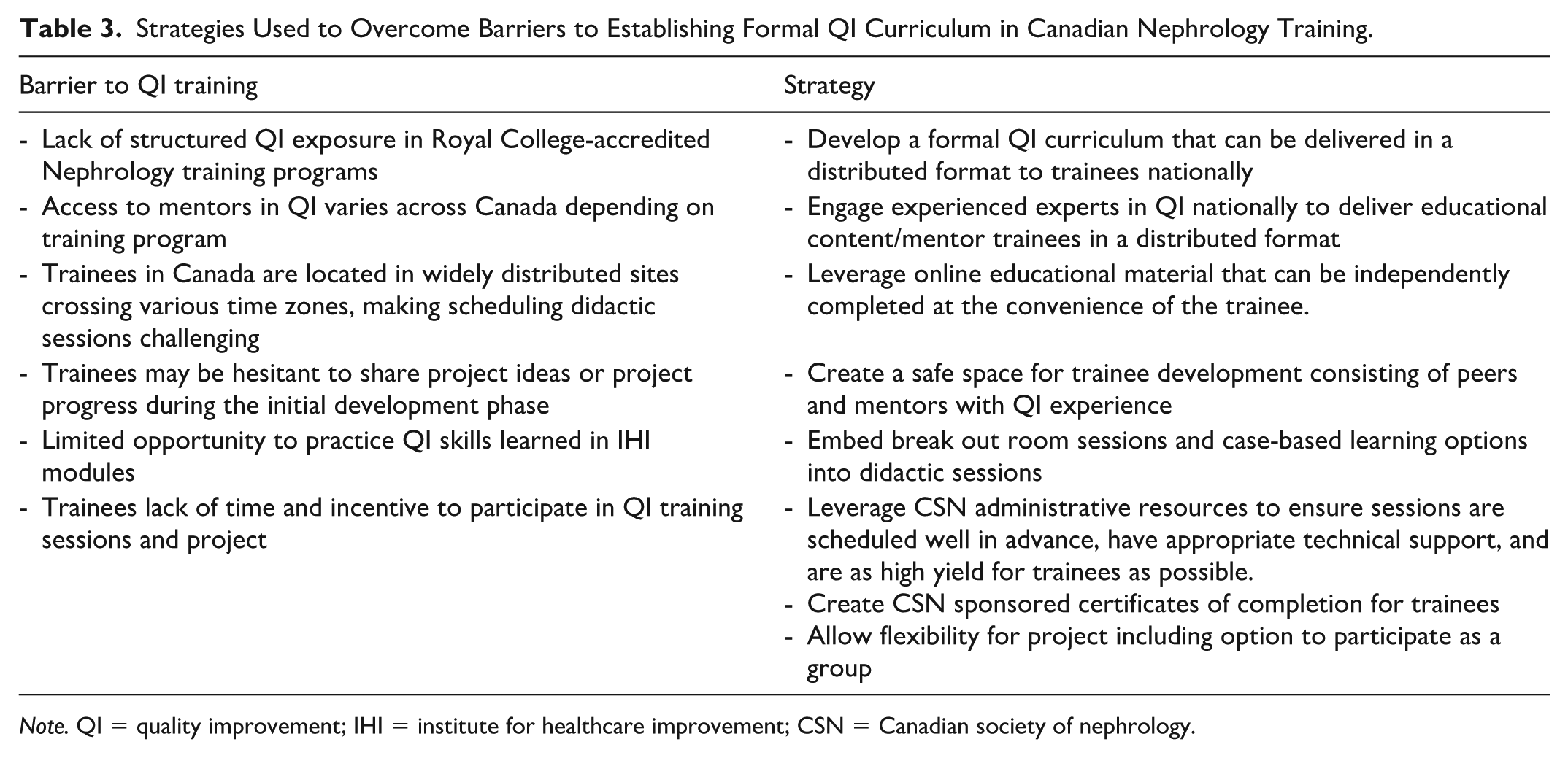
Note. QI = quality improvement; IHI = institute for healthcare improvement; CSN = Canadian society of nephrology.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.