
Abstract

Why Nephrology and Why Now?
In Canada, more than 40 000 patients are receiving dialysis or transplant care, and an additional 4 million are estimated to have chronic kidney disease (CKD).1,2 The provision of health care for this population is complex and expensive. Patients seen by nephrologists were rated as the most complex based on a 9-marker measure of complexity, 3 and the annual direct costs for dialysis treatments alone total approximately $1.9 billion. 4 This environment exerts pressure on the health care system to provide both high-quality and cost-effective care for patients with CKD, at a time when the incidence and prevalence of patients receiving dialysis and transplant care in Canada are steadily increasing. 4 Therefore, it is not surprising a recent survey found that more than 40% of nephrologists reported burnout, one of the highest proportions of all specialties. 5
Quality improvement (QI) may provide the framework and tools to meet these challenges. While the concept of health care QI may seem abstract to some, it can be easily visualized as the combined and unceasing efforts of everyone—health care professionals, patients and their families, researchers, payers, planners, and educators—to make the changes that will lead to the quadruple aim of better patient outcomes, better patient/provider experiences, and better value for money.6,7 Currently though, nephrology in Canada operates as “islands of excellence”; each province/program has its own strengths and weaknesses due in part to the variability in how nephrology care is structured and delivered. This pattern will likely continue unless efforts are made to transition Canadian nephrology into a learning health care system, whereby QI methodology and national partnerships help generate and share best practices through the natural outgrowth of innovative patient care. 8
Herein, we apply the joint perspectives of a new nephrology graduate, nephrologist with formal QI training, and leader of a provincial kidney agency to propose the formation of a Canadian Nephrology Quality Improvement and Implementation Science Collaborative (CN-QUIS) that will organize QI measurement and execution in response to growing patient numbers, complexity, provider burnout, and costs. We will outline the potential benefits of QI, describe nephrology-specific enablers of the proposed collaborative, and introduce a program of work for CN-QUIS with short-term and long-term deliverables by which to measure success.
QI in Nephrology: Possibilities and Challenges
Nephrology has several examples of QI initiatives that have affected each component of the quadruple aim (better patient outcomes, better patient/provider experiences, and better value for money) across multiple nephrology domains (ie, CKD, dialysis, and transplantation). For CKD, a meta-analysis of 21 studies in more than 30 000 patients demonstrated that multifaceted QI strategies targeted at health systems and patients (eg, case management, team changes) reduced dialysis incidence by 15%, lowered low-density lipoprotein cholesterol by 0.45 mmol/L, and increased use of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers by 16%. 14 In the dialysis unit, a regional hemodialysis program reduced the frequency of time-consuming routine blood work review by health care providers from every 4 weeks to every 6 weeks; in the process, direct laboratory costs decreased by $85 per patient-year with no difference in mortality or achievement of clinical targets for anemia and phosphate. 15 Regarding kidney transplantation, adoption of a 1-day donor assessment model improved both the rates of living kidney donation and the patient experience without increasing workup costs. 16 Clearly then, QI activities have the potential to influence all aspects of nephrology care across all elements of the quadruple aim—health outcomes, provider experiences, patient experiences, and health care costs.
However, nephrology still seems to lag behind other specialties in actual and published QI initiatives.14,17 In Canada, particular challenges to QI include (1) individual provincial and program quality-of-care indicators with little centralization in measurement or coordination of QI strategy, and (2) lack of frontline staff training in microsystem QI (ie, small-scale projects that test iterative changes in the hopes of improving local performance). A recent environmental scan of nephrology quality indicators demonstrated close to 140 different metrics in use across Canada, with little overlap between provinces outside of transplantation (Figure 1).11-13 This lack of coordination contributes to “islands of excellence” between provinces and different nephrology domains, which may make it difficult for individual programs to identify which quality indicators and initiatives should be prioritized among the large number that exist (a form of analysis paralysis). In addition, a recent survey of 127 Canadian nephrologists demonstrated that only 29% self-identified as having training in QI methodology. 18 This leads to an environment where many health care professionals lack the skills to independently design a local QI project that will help move a quality-of-care indicator, despite the presence of nephrology-specific step-by-step guides. 19 These key challenges contribute to the suboptimal use of QI resources and limit the ability of QI to reach its full potential.

Environmental scan of nephrology quality indicators currently in use across Canada. Validity was determined using a modified version of the Delphi consensus technique with a rating method adopted from the American College of Physicians/Agency for Healthcare Research and Quality.9–13 Common measures refer to indicators used in more than one province.
Overcoming Challenges by Using Existing Nephrology Networks
We propose that these challenges could be addressed through leveraging existing provincial and local nephrology structures and practices to collaborate on the prioritization of quality-of-care indicators and project execution. In this way, there are fewer indicators, and personnel trained in QI can be shared across regional silos to develop collective QI frameworks and initiatives. Examples of current structures and practices that enable QI collaboration include the following:
Provincial nephrology organizations that administer kidney care and are responsible for quality indicator development, measurement, and program reimbursement (eg, BC Renal Agency, Ontario Renal Network);
A growing Canadian nephrology workforce with advanced training in QI, exemplified by each province now having at least 1 nephrologist with certificate or MSc-level QI expertise;
Daily involvement from interdisciplinary and interprofessional providers in the care of patients with kidney disease (eg, dedicated nurses, dieticians, and pharmacists for patients on dialysis), who will be vital to the execution of frontline QI initiatives;
The recent creation of national patient networks to drive research and improve patient-centered outcomes in nephrology (Can-SOLVE CKD) 20 ;
Existing national networks focused on collaborative efforts in research (Canadian Nephrology Trials Network) and knowledge translation (Canadian Kidney Knowledge Translation and Generation Network).
Therefore, Canadian nephrology certainly possesses the infrastructure, growing QI expertise, and patient involvement required to realize the full benefits of QI methods. What is needed next is to collate and integrate these different elements into a national vision and organization that supports and permits ongoing collaboration in the future.
Our Vision: CN-QUIS
We propose that a national QI group, coined CN-QUIS, should be created to accomplish the following:
To establish and monitor key nephrology performance indicators (ie, quality assurance);
To educate and act as a resource for nephrology health care providers and patients on QI methods;
To increase the number of nephrology QI initiatives and spread best practices nationally to avoid QI project redundancy.
We envision 3 separate workgroups, each assigned a health care provider and patient lead, with deliverables mapped to each objective by which to measure success (Table 1). The performance indicator workgroup will ensure development of pan-Canadian nephrology quality indicators and review this list quarterly for progress and curation. The education workgroup will develop and execute a nephrology QI curriculum, not only for physician trainees but also for other health care providers, community sites, and patients. The Royal College of Physicians and Surgeons of Canada and Canadian Society of Nephrology will be key stakeholders in the development and dissemination of this curriculum, which will help ensure all nephrology stakeholders (ie, trainees, physicians, interdisciplinary providers, patients) have the baseline knowledge and skills required to design QI initiatives that target the quality indicators developed by the performance indicator workgroup. The improvement project workgroup will be charged with project execution, acting as a troubleshooting resource for local projects and cataloging past and current projects to avoid repetition and redundancy. Including community centers on a multidisciplinary webinar series will allow national sharing of local and/or regional QI initiatives that otherwise may have gone unnoticed. This group will also organize an annual national project that targets a prioritized national indicator. To promote progress, accountability, and transparency, we envision an annual workgroup update at the Canadian Society of Nephrology meeting with subsequent publications in the Canadian Journal of Kidney Health and Disease.
Canadian Nephrology Quality Improvement and Implementation Science Collaborative (CN-QUIS) Proposed Workgroups with Example Deliverables by Which to Measure Success.
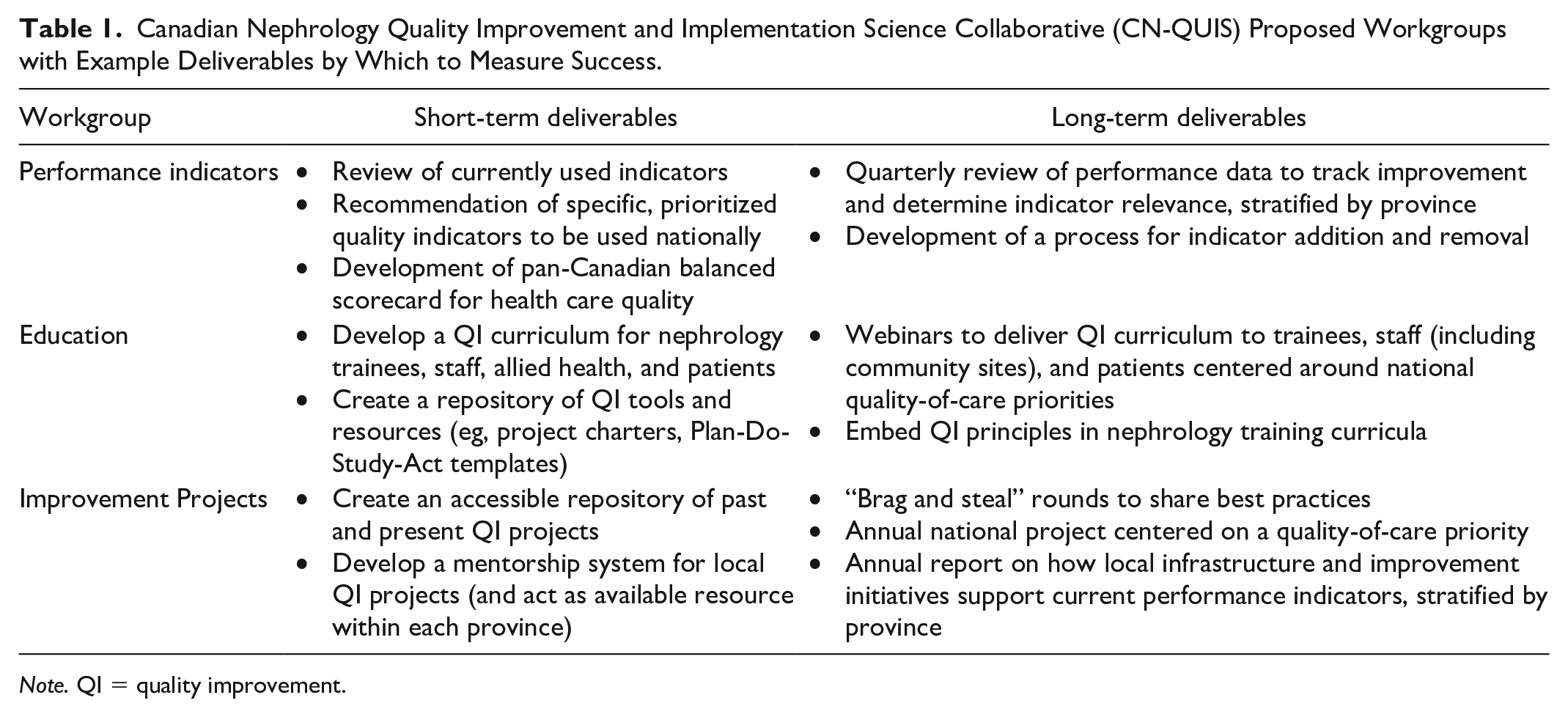
Note. QI = quality improvement.
Several challenges to the creation of CN-QUIS do exist, including different provincial contexts, data infrastructure capabilities, and reimbursement models. Accordingly, it will be important for CN-QUIS to develop indicators and QI work plans that consider and mitigate these potential barriers of success. Leveraging existing resources from the Canadian Society of Nephrology and provincial bodies to help support CN-QUIS will be important to ensure uptake and growth of this initiative nationally. For example, securing funds to hire a dedicated QI administrator (whose role exists in several provinces) would allow each workgroup more time to focus on their underlying deliverables as well as help promote cohesion and communication between groups. Such changes in workflow may not be easy, but large-scale QI collaboratives facing similar challenges have been successful in nephrology and other medical specialties,21-23 demonstrating the breadth and potential of what can be accomplished.
In QI, it is often said that every system is perfectly designed to deliver the results it gets. 24 This currently means “islands of excellence” and variability in nephrology outcomes across Canada. In response to growing patient numbers, complexity, provider burnout, and costs, the time is now to collaborate on QI measurement and execution. Canadian nephrology already involves regional and provincial evaluation of health care quality in some capacity, but usually without the specialized expertise that can be provided by health care professionals trained in QI methods. These nephrology providers are willing to donate their time and knowledge toward national efforts such as CN-QUIS, so a natural partnership opportunity exists between regional/provincial organizations that possess the QI infrastructure and frontline nephrology providers with QI training. When combined with emerging patient and research networks, it will be exciting to see whether CN-QUIS can become a reality and help Canadian nephrology move beyond “islands of excellence” toward a learning health care system perfectly designed for continual improvement and better patient outcomes.
Footnotes
Acknowledgements
The authors would like to recognize those who contributed to the quality indicator environmental scan: William Beaubien-Souligny, Daniel Blum, Lisa Dubrofsky, Tamara Glavinovic, Claire Harris, Jay Hingwala, Ali Ibrahim, Amber Molnar, Priya Mysore, Krishna Poinen, Sachin Shah, Karthik Tennankore, Alison Thomas, Amanda Vinson, and Seychelle Yohanna. S.A.S. is supported by a Kidney Research Scientist Core Education and National Training (KRESCENT) Program New Investigator Award (co-funded by the Kidney Foundation of Canada, Canadian Society of Nephrology, and Canadian Institutes of Health Research).
Ethics Approval and Consent to Participate
No ethics approval or consent to participate was required for this publication.
Consent for Publication
The authors have consented publication of this article.
Availability of Data and Materials
Data and materials are available by contacting the corresponding author.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.A.S. has received speaking fees from Baxter and Sanofi Canada. The remaining authors have no relevant conflicts of interest to declare. All authors approved the final version of the submitted manuscript. We certify that this manuscript nor one with substantially similar content has been published or is being considered for publication elsewhere.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.