
Abstract
Background:
Chronic kidney disease (CKD) represents a global health concern, with particular significance in Latin America due to socioeconomic inequalities and heterogeneous health care systems.
Objective:
To determine the prevalence of CKD in Latin American populations through a systematic review with meta-analysis.
Design:
Systematic review and meta-analysis of observational studies following the PRISMA guidelines.
Setting:
Twelve Latin American countries (Argentina, Brazil, Chile, Colombia, Cuba, Ecuador, El Salvador, Haiti, Mexico, Nicaragua, Panama, and Peru).
Patients:
A total of 72 486 participants from 21 observational studies reporting CKD prevalence in Latin American populations.
Measurements:
The CKD prevalence according to Kidney Disease: Improving Global Outcomes (KDIGO) or Kidney Disease Outcomes Quality Initiative (K/DOQI) criteria, stratified by age groups (<60-65 vs ≥60-65 years), sex, CKD categories (G1-G5), and country.
Methods:
Systematic search in PubMed, SCOPUS, Web of Science, and EMBASE databases. Observational studies using standardized CKD diagnostic criteria were included without language restrictions. A meta-analysis was conducted using random-effects models with a Freeman-Tukey double arcsine transformation. The risk of bias was assessed using the Munn et al tool. Meta-regressions examined temporal trends and the effects of sample size.
Results:
The pooled CKD prevalence was 17.14% (95% confidence interval [CI] = 13.40-21.23%) with high heterogeneity (I2 = 99.5%). Age-stratified analysis revealed a prevalence of 11.66% (95% CI = 8.09%-15.79%) in younger adults and 28.29% (95% CI = 22.34%-34.64%) in older adults. Women showed a higher prevalence (19.23%) compared to men (16.75%). Country-specific estimates ranged from 7.26% in Ecuador to 27.14% in Haiti. Meta-regression showed no significant temporal trend (P = .178).
Limitations:
High between-study heterogeneity, most studies used single measurements rather than confirming chronicity, potential publication bias favoring higher prevalence studies, and limited representation from certain countries, which restricts generalizability.
Conclusions:
The prevalence of CKD in Latin America exhibits marked age-related differences, with consistently higher rates in older adults. These findings support the need for age-specific prevention strategies and standardized diagnostic approaches across the region.
Trial registration:
Not registered prospectively (limitation acknowledged).
Introduction
Chronic kidney disease (CKD) represents a growing public health concern globally, with significant implications for morbidity, mortality, and health care-associated costs. 1 This disease is characterized by a progressive and generally irreversible reduction in kidney function, leading to an increased risk of cardiovascular complications, frequent hospitalizations, and decreased quality of life. Given this scenario, health authorities have recognized the need to develop strategies for prevention, early detection, and timely treatment to mitigate its impact. 2
In Latin America, CKD presents a complex epidemiological pattern influenced by social, economic, environmental, and genetic factors, as well as by the burden of chronic non-communicable diseases, particularly diabetes mellitus and hypertension. 3 The region is characterized by ethnic diversity, substantial heterogeneity in health care system organization, and socioeconomic inequalities, which complicate the collection of standardized and comparable data on CKD prevalence. 4 These disparities, in turn, limit the capacity to implement evidence-based health policies and optimize available resources.
Although individual studies have addressed CKD prevalence in various Latin American countries, the resulting information tends to be fragmented, with substantial methodological variations in diagnosis, definitions employed, and populations studied. This hinders the construction of a comprehensive overview to guide regional public health strategies. The absence of a consolidated and robust estimate of the CKD burden in the region constitutes a knowledge gap that must be addressed.5,6
Therefore, this systematic review (SR) with meta-analysis aims to determine the prevalence of CKD in Latin America, providing a comprehensive perspective that contributes to informed decision-making in public health. Consolidating this information will help guide prevention, early diagnosis, treatment, and care policies, aiming to improve the quality of life of affected populations in the region.
Methods
Research Design
This SR with meta-analysis was reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement guidelines. At the same time, the methodological design followed specific recommendations by Munn et al for systematic reviews focused on prevalence estimates.7,8
Search Strategy
The search strategy was conducted across 4 international databases, selected by the methodological recommendations of the Cochrane guidelines: SCOPUS, Web of Science (including the SciELO catalog), PubMed, and EMBASE. 9 This selection ensures comprehensive coverage of relevant literature in primary sources and region-specific publications. Keywords included the acronym CKD, the term “prevalence,” and the names of all Latin American countries, combined using Boolean operators and truncation strategies as needed. The complete details of the plan, including search equations used for each database, can be found in Supplementary Material 1.
Study Selection Criteria
Observational studies, primarily cross-sectional, reporting data on CKD prevalence in Latin American populations were included. For CKD diagnosis, studies using internationally recognized criteria, such as those established by the KDIGO (Kidney Disease: Improving Global Outcomes) guidelines, were considered. According to these guidelines, CKD is defined by either eGFR below 60 mL/min/1.73 m2 (categories G3-G5) or the presence of kidney damage markers (primarily albuminuria/proteinuria) with preserved eGFR ≥60 mL/min/1.73 m2 (categories G1-G2) for a period greater than or equal to 3 months. 10 We included studies reporting any CKD category (G1-G5), provided they followed these standardized diagnostic criteria. No language restrictions were applied.
In addition, probabilistic and non-probabilistic sampling studies were accepted, provided the design allowed valid prevalence estimation in the target population. We excluded studies whose target population consisted exclusively of individuals with specific conditions predisposing to CKD (such as diabetes mellitus or hypertension), as this could significantly overestimate the population prevalence by representing high-risk groups. Similarly, studies conducted exclusively in specific clinical settings (maintenance dialysis centers, kidney transplant clinics, hospitals), institutional environments (long-term care facilities, prisons), or groups selected by disease severity were excluded. In contrast, the studies included in this SR incorporated general populations, including individuals across the full spectrum of CKD (those with category G5D receiving maintenance dialysis or G1T-G5T with kidney transplants), with and without comorbidities, which coexisted, thus reflecting the actual epidemiological diversity of Latin American communities.
It is worth noting that studies focused on populations with specific ethnic or geographical characteristics (such as Indigenous groups or rural communities) were included, as long as they were not selected based on predisposing clinical conditions. These works provide valuable information on the distribution of CKD in important demographic subgroups in the region.
Furthermore, case reports, letters to the editor, SRs, bibliometric reviews, and qualitative studies that did not provide quantitative prevalence estimates were excluded. Thus, the selection criteria aimed to maximize the comparability and relevance of estimates included in the meta-analysis, providing solid evidence contextualized to the Latin American reality.
Study Selection Process
The search strategy was systematically applied to the selected databases, and the results were subsequently imported into the Rayyan platform to facilitate duplicate detection and initial screening. Two independent reviewers conducted the selection process simultaneously and anonymously, labeling studies as “include” or “exclude” according to previously established criteria. Upon completion of this stage, blinding was lifted, and decisions from both reviewers were compared. In cases of discrepancy, discussion and consensus were followed among the reviewers. If an agreement could not be reached, a third author acted as an arbiter, deciding on the study’s inclusion or exclusion. This methodology aimed to maximize the internal validity of the selection process, thereby minimizing the influence of individual bias.
Data Extraction and Narrative Synthesis
Data extraction was performed using a template designed in Microsoft Excel 2023, where detailed information about each included study was recorded. Two reviewers independently collected the following variables: author(s) and publication year, Latin American country(ies) involved, study design and data collection period, sample size and demographic characteristics (age, sex), sampling method used (probabilistic or non-probabilistic), diagnostic criteria employed for CKD detection, and reported prevalence estimation. In cases of discrepancies, consensus was sought; if agreement could not be reached, a third reviewer was consulted to resolve the situation.
Clear operational definitions and previously agreed-upon standardization criteria were established for each item to maintain the process’s validity and reliability. This minimized heterogeneity in information collection and the emergence of potential bias.7,8
Subsequently, a narrative synthesis of the characteristics of the selected studies was conducted. This analysis identified differences and similarities in methods, population contexts, diagnostic criteria employed, and reported prevalence magnitudes. It also facilitated understanding regional, subregional, and national dynamics and identifying possible contextual factors influencing prevalence estimates.
The narrative synthesis served as a foundation for subsequent quantitative integration (meta-analysis), providing a preliminary understanding of the epidemiological landscape of CKD in Latin America and offering a structured approach to interpreting results derived from subsequent statistical analysis.
Risk of Bias Assessment
Two independent reviewers employed the critical appraisal instrument developed by Munn et al, an internationally validated tool for prevalence studies, to evaluate the methodological quality of included studies.7,8 The instrument assesses 9 fundamental methodological aspects: sampling frame representativeness, appropriateness of participant selection methods, adequacy of sample size, comprehensiveness in context and participant description, coverage of data analysis, validity of diagnostic methods, standardization of measurement, and appropriateness of statistical analysis. The evaluation of each criterion was conducted using a trichotomous scale (“Yes,” “No,” “Unclear”), assigning 1 point for each affirmative response. Studies were stratified according to their total score into 3 risk of bias categories: low (7-9 points), moderate (4-6 points), and high (0-3 points).
Statistical Analysis
All quantitative analyses were performed using R statistical software, version 4.2.2. Studies reporting CKD prevalence data were included in the meta-analysis, and the total sample size (n) and number of cases (r) for each were extracted. These data provided the basis for calculating pooled prevalence estimates and their respective confidence intervals.
The metaprop function from the meta package in R was employed for the meta-analysis. The Freeman-Tukey double arcsine transformation (“sm = ‘PFT’”) was used to stabilize the proportion variance. Confidence intervals were calculated using the Clopper-Pearson method (“method.ci = ‘CP’”), which provides exact intervals for proportions.
Given the expected diversity among studies regarding population characteristics, CKD diagnostic criteria, and local contexts specific to Latin American countries, a random-effects model was used to integrate the results. Specifically, the DerSimonian and Laird method (“method.tau = ‘DL’”) and Hartung-Knapp correction (“hakn = TRUE”) were applied to adjust variance estimates and minimize heterogeneity impact on global estimation precision. Between-study heterogeneity was evaluated using the I2 statistic and Cochran's Q test, automatically calculated by the metaprop function.
Regarding age stratification, studies provided data in groups of <60 years and ≥60 years, or in some cases, <65 years and ≥65 years. To maintain consistency in comparison and considering that a 5-year difference would not produce a significant variation in prevalence, the groups <60-65 and ≥60-65 were unified into a single category. This decision aims to maximize comparability and minimize heterogeneity resulting from slightly different age intervals.
Meta-analysis results were presented with their respective 95% confidence intervals and visualized through forest plots generated using the forest function from the meta package. In addition, meta-regressions were performed on publication year and sample size to explore possible sources of heterogeneity and contextual factors' influence. These meta-regressions were conducted using mixed-effects models through the rma function from the metafor package, with weights inversely proportional to each study’s variance. To examine differential temporal trends across demographic subgroups, we conducted additional stratified meta-regressions by sex (male/female) and age groups (<60-65 years and ≥60-65 years). Results were represented through bubble plots, where each bubble’s size reflects the study’s weight in the analysis, thus allowing clear visualization of covariables’ impact on CKD prevalence and identification of divergent patterns across demographic subgroups over time.
Results
Eligible Studies
The initial search in electronic databases identified 15 370 records, with no additional records identified through other sources. After removing duplicates, 9638 unique records remained for initial screening. Of these, 9514 records were excluded for the following reasons: non-Latin American populations (n = 1245), research in specific populations such as patients with diabetes or hypertension (n = 3742), ineligible methodological designs (n = 2876), and unrelated topics (n = 1651). Of the 124 full-text articles assessed, 103 additional studies were excluded due to incomplete prevalence data (n = 42), a specific population not being declared in the abstract (n = 29), and non-standardized diagnostic criteria (n = 32). Non-standardized diagnostic criteria included studies that did not specify their diagnostic methodology or used definitions of CKD that did not follow KDIGO or K/DOQI criteria. Finally, 21 studies met the inclusion criteria and were included in the narrative synthesis and meta-analysis11-31 (Figure 1).
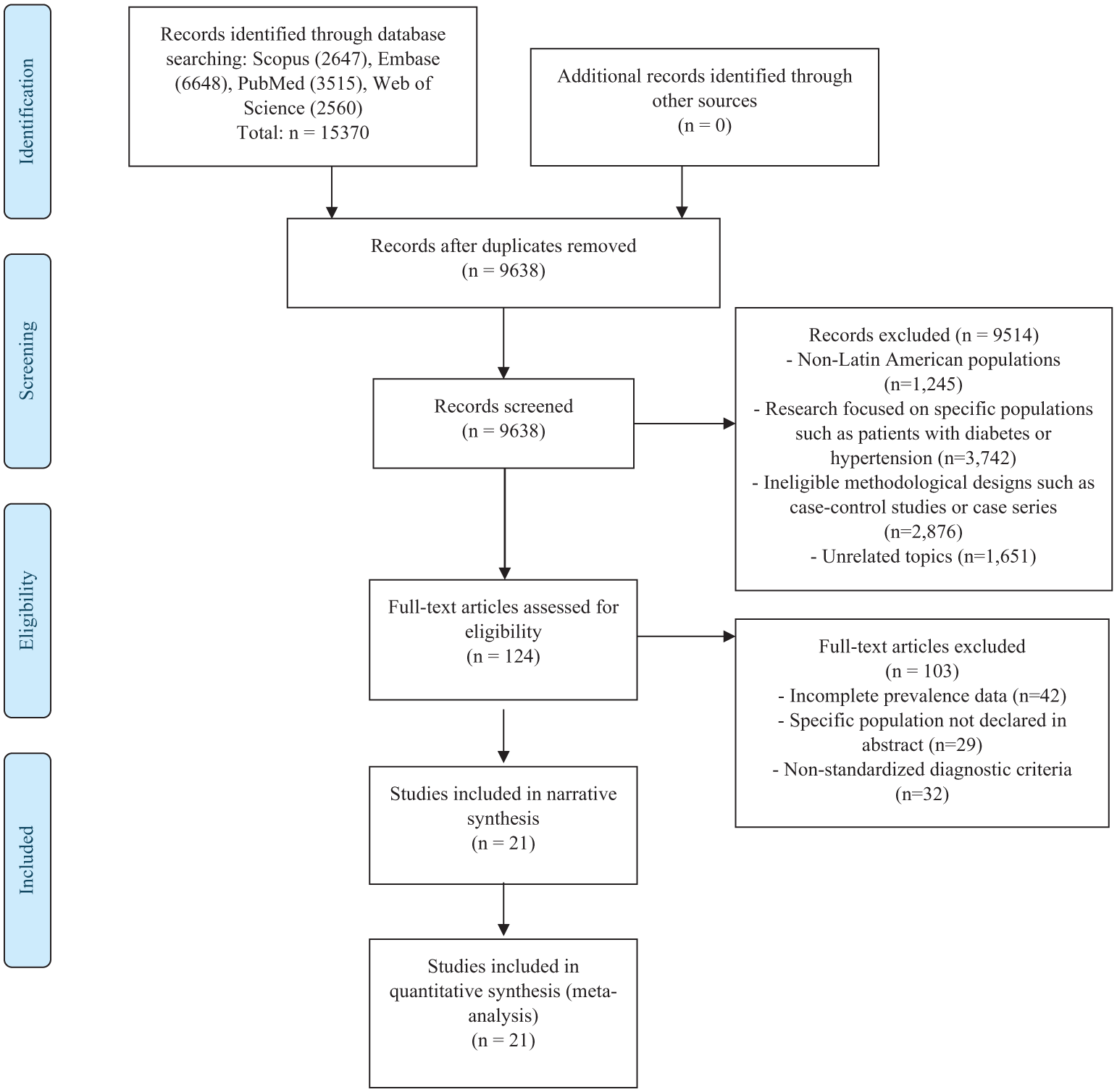
Flowchart of Study Selection.
Study Characteristics
Most investigations were conducted in Brazil,12,20,22,23,25 Mexico,13,17,31 El Salvador,14,15,27 and Chile,21,28 although evidence from Argentina, 11 Haiti, 16 Nicaragua, 18 Peru, 19 Panama, 24 Cuba, 26 and Ecuador 29 was also included (Table 1). This geographical distribution reflects the growing scientific interest in understanding the CKD burden across different national contexts, characterized by sociodemographic, economic, and environmental differences.
Summary of selected studies.

Abbreviations: CKD: Chronic Kidney Disease; eGFR: Estimated Glomerular Filtration Rate; KDIGO: Kidney Disease: Improving Global Outcomes; K/DOQI: Kidney Disease Outcomes Quality Initiative; MDRD: Modification of Diet in Kidney Disease; CKD-EPI: Chronic Kidney Disease Epidemiology Collaboration; ACR: Albumin-to-Creatinine Ratio; UACR: Urinary Albumin-to-Creatinine Ratio; UAE: Urinary Albumin Excretion; IMSS: Mexican Social Security Institute.
Regarding sampling, studies exhibit both probabilistic and non-probabilistic designs. Some works, such as Bastos and Kirsztajn 12 or Lebov et al, 18 employ probabilistic sampling that strengthens the representativeness of their findings at the population level. Conversely, investigations like Bianchi et al 11 or García-García o García-García et al 13 are based on non-probabilistic sampling, focused on specific populations, whether by ethnicity, geographic region, or residence pattern. Similarly, sample sizes vary significantly, from studies with just a few hundred participants (eg, Vela et al 14 ) to large samples with several thousand individuals (eg, Barreto et al 20 and Valdés et al). 26
Regarding studied population characteristics, the mean age ranges from young adults, with an average close to 35 to 40 years, as in Vela et al 14 or Gomes et al, 30 to older groups (eg, Ríos 2016, with a mean of 67 years). 21 The proportions of women vary widely, although many studies show greater female participation. Additionally, some investigations focus on Indigenous communities (Bianchi et al 11 and Gomes et al 30 ) or rural areas (Orantes et al 15 ) while others include large urban centers (Francis, 2015; Malta, 2019),19,25 contributing to a more diverse epidemiological map.
Most studies followed international guidelines, either K/DOQI or KDIGO, but employed different tools to eGFR and detect signs of kidney damage. For example, Bianchi et al 11 in Argentina and Bastos and Kirsztajn 12 in Brazil used K/DOQI-based definitions, although with different formulas: the former used the Levy formula and proteinuria ≥0.20, while the latter applied the Cockcroft-Gault formula adjusted for body surface area. García-García et al 13 in Mexico also based on K/DOQI but estimated eGFR with Modification of Diet in Kidney Disease (MDRD) and evaluated proteinuria (≥1+ on dipstick). Meanwhile, Vela et al 14 and Orantes et al 15 in El Salvador, along with other subsequent studies (eg, Burkhalter et al 16 in Haiti and Cueto-Manzano et al 17 in Mexico), adopted KDIGO guidelines, using formulas such as MDRD or Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI), plus proteinuria or albuminuria to confirm kidney damage.
A trend toward increased use of the CKD-EPI formula for eGFR estimation is observed over the years, as seen in Burkhalter, 16 Francis, 19 Barreto, 20 Rios, 21 Pereira, 22 or Valdés. 26 Some studies, such as Malta 25 in Brazil, relied exclusively on eGFR to define CKD without considering albuminuria, while others, like Barreto et al 20 and Velásquez et al, 24 included the albumin-creatinine ratio (ACR) criterion. In more recent works—Walbaum et al 28 in Chile, Eguiguren-Jiménez et al 29 in Ecuador, Gomes et al 30 in Brazil, and Paredes et al 31 in Mexico—KDIGO guidelines continue to predominate, with eGFR by CKD-EPI and detection of kidney damage markers such as albuminuria (ACR ≥30 mg/g or Urinary Albumin-to-Creatinine Ratio [UACR] ≥30 mg/g).
The risk of bias assessment showed favorable results, with all studies classified in the low-risk category (scores between 7 and 8 out of a maximum of 9 points). The variability in scores was primarily due to 2 factors: no study achieved the maximum score due to the absence of comparative analysis with non-responders, and the additional point of variation was attributed exclusively to those studies that implemented probabilistic sampling.12,14,18,19,22-29,31 For detailed information on the risk of bias assessment for each study according to the 9 criteria of the Munn et al tool, please refer to Supplementary Table 2.
Meta-analysis of Chronic Kidney Disease Prevalence in Latin America
The global meta-analysis presented in Figure 2, which integrates results from multiple studies conducted throughout Latin America, shows a pooled CKD prevalence of approximately 17.14% (95% CI = 13.40%-21.23%), accompanied by high heterogeneity (I2 = 99.5%, P < .001). Among the included works, the study by Vela et al 14 in El Salvador exhibited the highest prevalence (24.98%), while Bastos et al 12 in Brazil reported the lowest (6.7%).

Forest plot of the meta-analysis of the prevalence of CKD.
Meta-analysis of Chronic Kidney Disease Prevalence, Stratified by Sex, Age, and Country
The CKD prevalence stratified by sex, based on 15 studies,11,12,14-16,18-20,22-25,27,30,31 shows figures of 16.75% (95% CI = 11.58-22.64) for men and 19.23% (95% CI = 13.83-25.28) for women. When analyzed by age groups, the meta-analysis of 11 studies11,12,15,16,18-20,22,25,27,30 indicates that the prevalence for individuals under 60 to 65 years is 13.92% (95% CI = 9.35-19.22), while in the group of 60 to 65 years or older, also with 11 studies, the prevalence is 30.65% (95% CI = 25.97-35.53) (Table 2).
Sensitivity analysis of the prevalence of CKD in Latin America.

The pooled prevalence by CKD categories showed estimates ranging from 2.0% (95% CI = 0.50-3.40) for stage G5 to 8.79% (95% CI = 5.38-12.9) for stage G3. Categories G1 and G2 presented similar values (8.45% and 8.25%, respectively), with wide confidence intervals and high levels of heterogeneity (I2 > 98%) (Table 2).
Prevalence by country shows marked variation. Among individual studies, Argentina shows a prevalence of 24.16% (95% CI = 20.00-28.57), Haiti 27.14% (95% CI = 23.67-30.75), Nicaragua 9.14% (95% CI = 7.99-10.36), Peru 16.83% (95% CI = 13.33-20.65), Panama 12.00% (95% CI = 10.95-13.09), Cuba 9.63% (95% CI = 8.97-10.32), and Ecuador 7.26% (95% CI: 5.57-9.15). In countries with more than 1 study, Brazil (6 studies) shows 13.91% (95% CI = 9.65-18.79), Mexico (3 studies) 20.79% (95% CI = 11.18-32.43), El Salvador (3 studies) 24.98% (95% CI = 14.97-36.57), and Chile (2 studies) 20.58% (95% CI = 11.02-32.20) (Table 2). In addition, the distribution of CKD prevalence by country is presented in Figure 3.

Map of Latin America showing CKD prevalence by country.
Meta-regression Between Publication Year and Estimated Chronic Kidney Disease Prevalence
The meta-regression analysis (Figure 4A) showed no statistically significant temporal trend in overall CKD prevalence across publication years (β = −0.0096, P = .178), with prevalence estimates remaining relatively stable around 6% to 7% throughout the study period. Despite this overall stability, there is considerable heterogeneity among individual studies, as reflected by the marked dispersion of points around the trend line. In the bubble diagram, sphere size represents sample size, while different colors distinguish countries of origin, allowing observation that studies with larger numbers of participants, such as García-García et al 13 or Barreto et al, 20 show prevalence estimates within the expected range. Some outliers are identified, such as Bianchi et al 11 with relatively high prevalence, and Eguiguren-Jiménez et al 29 with markedly low prevalence, contributing to the observed heterogeneity. Brazil and Mexico contributed several studies throughout the period, providing representation across different time points.

Meta-regression of CKD prevalence by publication year in Latin America: (A) overall trend; (B) sex-stratified analysis showing parallel trends by sex; (C) age-stratified analysis showing differences between age groups.
When stratified by sex (Figure 4B), females and males showed relatively stable patterns over time, with women showing higher prevalence in more recent studies, while the difference was less apparent in earlier studies. Age-stratified meta-regression (Figure 4C) showed consistent differences between age groups across publication years. The <60/65 years group showed prevalence estimates ranging from approximately 8% to 15%, while the ≥60/65 years group consistently maintained higher prevalence rates (around 30%-32%) throughout the study period. This pattern demonstrates the well-established age-related difference in CKD prevalence, with older adults consistently showing substantially higher rates than younger populations across all studies.
Finally, the meta-regression analysis according to sample size (Supplementary Material 3) reveals a slightly decreasing trend in CKD prevalence based on the number of participants. The trend line, plotted with a logarithmic scale on the X-axis to span from samples of a few hundred to several thousand individuals, suggests that studies with smaller sample sizes present more variable and dispersed prevalences. In contrast, larger studies, such as Malta et al, 25 tend to concentrate on more moderate prevalences.
Funnel Plot Analysis
Regarding the funnel plot (Figure 5), which uses the Freeman-Tukey double arcsine transformed proportion on the x-axis and standard error on the y-axis, we observed a distribution pattern that suggests the presence of heterogeneity and potential publication bias. Most studies are scattered across a transformed proportion range between 0.3 and 0.6, with few conforming closely to the expected funnel shape around the central effect estimate. The vertical distribution of standard errors varies from approximately 0.005 to 0.033, with larger studies (smaller standard errors) showing considerable dispersion rather than concentrating tightly around the central line.

Funnel plots for the assessment of publication bias in CKD prevalence studies.
The asymmetrical distribution of studies, with several points falling outside the funnel boundaries, particularly in the regions of higher effect sizes (right side), suggests potential small-study effects where smaller studies with larger effect sizes are more likely to be published. Notably, 1 study with a very high transformed proportion (approximately 0.8) and relatively small standard error deviates substantially from the others, representing a potential outlier.
Discussion
Main Findings
This SR with meta-analysis fills the knowledge gap by providing a consolidated estimate of CKD burden in Latin America. Integrating data from 21 studies across 12 countries (72 486 individuals), we established an overall pooled prevalence of 17.14% (95% CI = 13.40%–21.23%). Our findings revealed marked differences by sociodemographic variables and geographical contexts. Women showed a higher prevalence (19.23%) compared to men (16.75%), with this difference becoming more pronounced in recent studies. Most importantly, older adults (≥60/65 years) showed a much higher prevalence (28.29%) compared to younger populations (11.66%), demonstrating the consistently higher CKD burden observed in this demographic group. Country-level estimates ranged from 7.26% in Ecuador to 27.14% in Haiti, showing regional dispersion.
Meta-regression analyses revealed no significant temporal trend in overall CKD prevalence across publication years (P = .178), indicating stable estimates over time. However, age-stratified analysis showed consistent differences between age groups throughout the study period. The high heterogeneity observed (I2 = 99.5%) suggests that the influence of diverse diagnostic methods, population settings, and sampling scales is significant.
When comparing our results with global estimates, the prevalence of CKD in Latin America tends to be equal to or higher than in other regions. The Global Burden of Disease Study 2017 reported global CKD prevalence around 9.1%, 1 while other reviews found ranges between 7.2% and 12%. 32 The recent ISN-Global Kidney Health Atlas 2024 reports a median CKD prevalence in Latin America of 10.15% (interquartile range [IQR] = 8.35%-12.28%). 33 Our SR complements this approach by integrating 21 population-based studies that used internationally recognized diagnostic criteria, despite methodological heterogeneity in their application, calculating a weighted regional prevalence of 15.9% (95% CI = 12.2%-19.9%), and providing detailed information to support local health care decision-making. Suriyong et al’s study found a prevalence of 11.2% in Asia, although this was specific to categories G3 through G5. 34 Similarly, Jha et al’s work 35 showed that the proportion of CKD can reach up to 16% in certain vulnerable populations. Compared to these values, the Latin American panorama shows figures that can greatly exceed these thresholds in certain countries or groups, evidencing the need for a more detailed evaluation of the region’s sociodemographic, methodological, and environmental factors.
Methodological differences greatly affected observed heterogeneity. Studies using probabilistic community-based sampling yielded more moderate prevalence estimates, such as Malta et al 25 with 6.7% and Velásquez et al 24 with 12.0%. In contrast, studies focused on high-risk communities reported higher figures, such as Bianchi et al 11 in Indigenous communities (24.2%) or Burkhalter et al 16 in Haitian outpatient clinics (27.1%). These patterns show the need for standardized approaches in future epidemiological studies.
Another determining factor of heterogeneity relates to sociodemographic and environmental characteristics of the included populations. The wide ethnic diversity, coexistence of rural and urban areas, and different comorbidity profiles affect CKD progression and diagnosis differently. 36 Furthermore, the unequal availability of primary care resources and varying degrees of implementation of early detection programs lead to biases in case identification.
The marked country-level variation was conditioned by study availability and sample size limitations. Some countries had only single studies, making it difficult to establish solid conclusions about the real magnitude of CKD in these contexts. This methodological limitation could explain the observed value disparity, as heterogeneity in diagnostic criteria may increase these divergences.
The observed stability in prevalence estimates over time should be interpreted cautiously, considering potential methodological influences such as improvements in study design, increasingly standardized diagnostic approaches, and more representative sampling strategies in recent studies. The progressive adoption of the CKD-EPI formula over older estimating equations may have led to more accurate categorization of kidney function, potentially resulting in more consistent prevalence estimates across periods.37,38 This methodological evolution may partially explain the observed stability in prevalence estimates, as improvements in diagnostic accuracy may have offset any true changes in disease burden.
Practical Public Health Implications
The relevance of this study for public health lies in the fact that CKD constitutes a significant problem affecting the quality of life and survival of millions of people while also generating a large economic impact on health care systems. The stable temporal patterns, with consistently higher prevalence in older adults, demonstrate the need for demographically tailored public health strategies. Since CKD is strongly associated with diabetes mellitus and hypertension, early identification and effective control are essential to reduce progression toward advanced categories requiring costly treatments such as maintenance dialysis or kidney transplantation. 35
In Latin America, socioeconomic inequalities, health system fragmentation, and geographic diversity hinder the implementation of homogeneous CKD prevention strategies. 4 Our stratified meta-analysis offers a foundation for designing targeted interventions, particularly for older adults who consistently show higher risk levels.
It is fundamental to encourage population studies that examine CKD prevalence uniformly, following standardized protocols and using consensus diagnostic definitions. 10 Such studies should systematically include age and sex stratification to track demographic disparities and monitor prevalence patterns across different population segments. Furthermore, coordinating efforts among Latin American countries can generate opportunities to develop regional databases and age-specific joint strategies, avoiding resource duplication and promoting greater efficiency in obtaining results.
We recommend developing differentiated prevention programs dealing with unique risk profiles of older adults while maintaining effective interventions for all age groups. For all age groups, continuing to prioritize modifiable risk factor control such as obesity, hypertension, and diabetes 10 remains essential. For older adults, implementing integrated care models that handle multimorbidity, age-appropriate screening protocols, and specialized kidney care pathways may be necessary to manage the consistently higher prevalence observed in this population. Adopting comprehensive primary care models, strengthening health education, and guaranteeing access to early diagnostic tests—particularly in rural populations—emerge as key elements to reduce CKD burden across demographic groups in the region.
Strengths and Limitations
Important strengths of this meta-analysis include the exhaustive search across multiple databases, the use of well-defined inclusion criteria and quality assessment, and the application of quantitative synthesis techniques that estimate CKD prevalence in the region with greater statistical robustness. The stratification by demographic variables and our analyses of prevalence patterns across different populations provide valuable insights that would not be apparent from individual studies or narrative reviews alone.
However, important limitations must be recognized. Our pooled prevalence estimate likely overestimates the true burden of CKD in the general Latin American population due to several systematic biases: most studies used single measurements rather than confirming chronicity through repeated assessments; there was overrepresentation of urban and health care-seeking populations; and publication bias may favor studies with higher prevalence findings. Studies with more rigorous methodologies consistently showed lower prevalence figures than our overall estimate, suggesting this upward bias. In addition, the inclusion of countries with limited representation (a single study) restricts the external validity of country-specific estimates. Despite these limitations, our findings represent the most comprehensive synthesis of available evidence to date and provide valuable baseline information to guide public health planning and future research.
Conclusions and Recommendations
In conclusion, the findings reveal stable temporal patterns in CKD prevalence in Latin America, with no significant changes over time, but notable demographic variations. Most importantly, there is a consistent and large difference between age groups, with older adults showing markedly higher CKD prevalence compared to younger populations. Similarly, the relationship between sex and prevalence varied across studies, with women showing higher rates primarily in more recent publications. These patterns, coupled with considerable methodological heterogeneity across studies, show the need for more standardized research approaches and age-specific public health strategies.
To strengthen the public health response, we recommend developing differentiated prevention and early detection programs that specifically handle the unique risk profiles of older adults while maintaining effective interventions for all age groups. In addition, implementing integrated care models for elderly patients, establishing longitudinal population studies with consistent methodologies, promoting regional collaboration to standardize diagnostic practices, and investing in targeted interventions for aging populations are essential. These approaches will help manage the demographic patterns of CKD in Latin America, reduce the disease burden across all demographic groups, and improve resource allocation in health care systems throughout the region.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251382479 – Supplemental material for Prevalence of Chronic Kidney Disease in Latin America: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-cjk-10.1177_20543581251382479 for Prevalence of Chronic Kidney Disease in Latin America: A Systematic Review and Meta-analysis by Víctor Juan Vera-Ponce, Joan A. Loayza-Castro, Luisa Erika Milagros Vásquez-Romero and Fiorella E. Zuzunaga-Montoya in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
Special thanks to the members of Universidad Nacional Toribio Rodríguez de Mendoza de Amazonas (UNTRM), Amazonas, Peru, for their support and contributions throughout the completion of this research.
Ethical Considerations and Consent to Participate
Since this manuscript is a secondary database study, it was not required.
Consent for Publication
Not applicable.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by Vicerectorado de Investigación de la Universidad Nacional Toribio Rodríguez de Mendoza de Amazonas.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon request to the corresponding author.
Informed Consent
Since this is a secondary data analysis, informed consent was not required.
Clinical trial number
Not applicable.
Use of AI and Language Assistance Tools
The authors used Grammarly and other language assistance tools to improve grammar, spelling, and sentence clarity during the writing and revision process. These tools were used solely for language enhancement and did not contribute to the scientific content, data analysis, or interpretation of results.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.