
Abstract
Background:
People with advanced chronic kidney disease (CKD) and secondary hyperparathyroidism (sHPT) refractory to medical therapy often require surgical parathyroidectomy. Severe and prolonged hypocalcemia immediately following parathyroidectomy for sHPT is often termed “hungry bone syndrome” (HBS).
Objective:
To systematically review the effect of pre-operative interventions on post-operative hypocalcemia, HBS, and other related outcomes in patients with CKD and sHPT undergoing parathyroidectomy.
Design:
This is a systematic review study.
Setting:
Diverse study designs conducted in any country.
Patients:
Adult patients with CKD complicated by sHPT undergoing parathyroidectomy.
Measurements:
Post-operative hypocalcemia, HBS, symptomatic hypocalcemia, and other related outcomes.
Methods:
We searched Ovid MEDLINE, Embase, and Cochrane Controlled Trials Registry from inception until June 2024 for trials and observational studies of adults with CKD and sHPT that evaluated pre-operative interventions aimed at reducing the risk of hypocalcemia following parathyroidectomy. After 2 phases of study screening conducted in duplicate, we extracted data on study design, patient characteristics, interventions, and outcomes. Hypocalcemia was defined as serum calcium <2.1 mmol/L and HBS as calcium <2.1 mmol/L for ≥4 days post-operatively. We evaluated the risk of bias and completed a narrative synthesis of the available literature across intervention types.
Results:
We identified 3616 studies; 35 underwent full-text review, and 9 met final eligibility criteria. Interventions included pre-operative calcitriol (n = 2), pre-operative cinacalcet (n = 3), pre-operative alkaline phosphatase (ALP) measurement to guide intravenous (IV) calcium administration (n = 3), and pre-operative pamidronate (n = 1). All studies reported on at least one of: median/mean post-operative calcium (n = 7), incidence of post-operative hypocalcemia (n = 3), HBS (n = 1), and symptomatic hypocalcemia (n = 4). Interventions that reported on the risk of post-operative hypocalcemia included pre-operative pamidronate (n = 1, 37 participants, odds ratio [OR] = 0.003, 95% confidence interval [CI] = 0.000-0.072) and IV calcium guided by pre-operative ALP (n = 1, 271 participants, OR = 0.292, 95% CI = 0.175-0.488). There were insufficient data to meta-analyze study-specific effects for any intervention or outcome.
Limitations:
Our study was limited by significant heterogeneity in outcome reporting, which resulted in substantial outcome reporting bias and prevented pooled analyses. Furthermore, no randomized control trials met our inclusion criteria, which limited assessment of publication bias.
Conclusions:
Pre-operative risk factors for HBS have been established in patients with CKD undergoing parathyroidectomy. However, limited research has evaluated pre-operative interventions to reduce the risk of HBS, and due to heterogeneity in outcome reporting across studies, there is still uncertainty about the effectiveness of such interventions. These findings support the need for future clinical trials.
Introduction
Secondary hyperparathyroidism (sHPT) is a common complication of severe chronic kidney disease (CKD). When sHPT is refractory to medical therapy, surgical management with parathyroidectomy is often required.1,2 Despite robust medical management and advancements with calcimimetics, approximately 15% of patients treated with maintenance dialysis will require parathyroidectomy within 10 years of dialysis initiation, and 38% will require it within 20 years. 3
After parathyroidectomy and following the sudden reduction of parathyroid hormone (PTH), patients are at risk of post-operative hypocalcemia, which occurs in more than three quarters of patients.4,5 When the hypocalcemia is severe and prolonged, this is known as Hungry Bone Syndrome (HBS), which has been reported in 27% to 58% of patients.6-10 Severe hypocalcemia may result in life-threatening complications including seizures, arrhythmias, and heart failure,9,10 all of which may contribute to adverse outcomes such as prolonged hospital length of stay and re-hospitalization.
Various studies have established risk factors for developing post-operative hypocalcemia and HBS, most notably elevated pre-operative alkaline phosphatase (ALP), PTH, and low pre-operative serum calcium.10-15 Some studies have investigated pre-emptive strategies to reduce the risk of hypocalcemia and HBS. However, heterogeneity remains in clinical practice with no established guidelines on strategies to prevent post-operative hypocalcemia and HBS. In this systematic review, we aimed to summarize the effect of pre-operative interventions on post-operative hypocalcemia, HBS, and other outcomes in patients with CKD and sHPT undergoing parathyroidectomy.
Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines 16 (checklist in Supplemental Table 1). The review protocol was registered in the PROSPERO international registry (ID CRD42023432922). Ethics approval was not required given the secondary use of published literature.
Eligibility Criteria
This systematic review included diverse study designs (retrospective, prospective, interventional, and comparative studies) of adults ≥18 years old with CKD (defined as estimated glomerular filtration rate <60 mL/min/1.73 m2 or kidney failure treated with dialysis) complicated by sHPT refractory to medical therapy undergoing parathyroidectomy. The sHPT was defined as the presence of persistently elevated PTH concentrations together with hypercalcemia and/or hyperphosphatemia or associated with clinical symptoms such as bone pain and pruritus, or as defined by the authors. 17 To be included, studies were required to investigate a pre-operative intervention such as (but not limited to) supplementation with activated vitamin D or vitamin D analogues, calcium, bisphosphonates, or another pre-operative intervention in isolation or in combination; all must have been examined in a study where the risk of post-operative calcium-based outcomes was estimated. Studies with protocols or interventions only initiated intra-operatively or post-operatively were excluded from our review. Additional exclusion criteria included studies performed in non-human participants, studies enrolling pediatric patients, studies including patients with primary hyperparathyroidism, surgeries apart from parathyroidectomy (such as full thyroidectomy), and studies that did not report on any calcium-based outcomes. The full database-specific search strategies can be found in Supplementary Item 1.
Databases, Search Strategy, and Study Selection
We identified peer-reviewed articles from MEDLINE, Embase, and Cochrane Controlled Trials Registry from database inception until June 2023, and this was updated in June 2024. Conference abstracts available in EMBASE from the past 3 years, and relevant studies within the ClinicalTrials.gov trial registration registry were also identified. The search was supplemented by scanning relevant references from studies that met the inclusion criteria and from related reviews.
Our search strategy was designed collaboratively with input from an information specialist and health sciences librarian (C.M.). We used medical subject headings and text words with related terms to identify the population of “kidney disease” and “parathyroidectomy.” The intervention search concept included multiple terms combined with Boolean Operator “OR.” Database specific search strategies can be found in Supplementary Item 1.
Using COVIDENCE (https://www.covidence.org/), 2 authors (A.L. and N.K.B.) independently screened titles and abstracts in duplicate that were retrieved using the defined inclusion criteria described above. The initial 100 abstracts were reviewed as a group to calibrate the reviewer’s interpretation of the inclusion criteria. If either reviewer identified an article as potentially eligible, it was advanced to the full-text review stage. Next, the 2 authors (A.L. and N.K.B.) independently reviewed full-text articles for inclusion. If there was disagreement, the 2 authors reached consensus by discussing with a third reviewer (T.G.H.).
Data Extraction and Risk of Bias
Data were extracted from eligible studies by 1 reviewer (A.L.) and reviewed in duplicate. Extracted data included study characteristics, patient characteristics, intervention details, and outcomes. The primary outcome of interest, post-operative hypocalcemia, was defined based on the literature as serum calcium <2.1 mmol/L or ionized calcium <0.95 mmol/L,6,9,10,18,19 with severe hypocalcemia as <1.8 mmol/L11-14,19 and critical hypocalcemia as <1.5 mmol/L.20,21 The post-operative median or mean serum calcium was also recorded. Secondary outcomes included incidence of HBS (defined as serum calcium <2.1 mmol/L for 4 days or more post-operatively), symptomatic hypocalcemia, length of hospital stay, and duration and quantity of post-operative intravenous (IV) or oral calcium or vitamin D provided. For each outcome indexed, the number of participants who experienced the event in each treatment group was recorded, as well as effect estimates with odds ratios (ORs) and accompanying 95% confidence intervals (CIs), where available. If ORs were not reported but the data required to calculate them were provided, we calculated ORs and accompanying 95% CIs. Where outcome data were not reported in the included studies, we attempted to contact corresponding authors of included studies at least twice to obtain missing information.
The quality of included studies was assessed using the Cochrane Collaboration recommendations. 22 Risk of bias was assessed using the ROBINS-I tool, 23 by 2 independent reviewers (A.L. and T.G.H.). Potential confounding domains included age, sex, dialysis dependency, and pre-operative ALP, calcium, and PTH levels. Risk of outcome reporting bias was assessed using the ORBIT tool. 24
Data Synthesis
The number and type of articles included in the study as well as the reasoning for exclusion are described in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram. 16 The primary and secondary outcomes were reported as ORs where available. We planned to meta-analyze study-specific effect estimates if there were at least 3 primary studies that investigated the same intervention and reported the same outcome. The certainty of the evidence was summarized using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. 25 One reviewer (A.L.) used the tool to narratively summarize the overall certainty, which was reviewed in duplicate (by T.G.H.) to ensure agreement.
Results
Study Selection
In this review, we initially identified 3726 studies (Figure 1); 313 duplicates were removed. In total, 3413 study abstracts were screened and 35 underwent full-text review. In total, 26 studies were excluded, leaving 9 studies that met final eligibility criteria. Reasons for study exclusion included lack of full-text article (n = 8), wrong outcomes (n = 1), wrong comparator (n = 2), and wrong intervention (n = 15).

PRISMA figure.
Among the 9 included studies, there were 898 participants included in total (range = 37–271 participants for each study). Study interventions included pre-operative calcitriol (n = 2),26,27 pre-operative cinacalcet (n = 3),28-30 pre-operative ALP to guide IV calcium administration (n = 3),18,31,32 and pre-operative pamidronate (n = 1) 33 (Table 1). The designs of the included studies included retrospective cohort study (n = 6), prospective pre-post interventional study (n = 2), and retrospective study with no control (n = 1). There were no randomized controlled trials (RCTs) that met eligibility criteria. There was 1 RCT in the full-text review, which was subsequently excluded because the intervention was initiated post-operatively.
Summary of Included Studies.

Note. Values are expressed as mean ± SD, median (interquartile range), and proportions with outcome. Age is expressed in years. HBS = Hungry bone syndrome; HD = hemodialysis; PD = peritoneal dialysis, I = intervention group, C = comparator group.
Study and Participant Characteristics
The average age reported for each study ranged from 35 to 55 years old. Most studies (n = 6) had a male predominance among participants. The patients predominantly had end-stage kidney disease, with the majority requiring hemodialysis or peritoneal dialysis (>90% across 7 studies), and a small subset having undergone kidney transplant. Among the small subset of patients not on dialysis, none of the studies reported the mean eGFR. With regard to pre-operative laboratory values, most studies reported PTH (n = 9), calcium (n = 9), phosphate (n = 6), and ALP (n = 6). Patient comorbidities were not commonly reported (n = 2). Apart from the 3 cinacalcet studies, none of the other studies reported on the details of medical therapy for sHPT pre-operatively.
Pre-operative calcitriol
Alsafran et al 26 and Ferreira et al 27 studied pre-operative oral calcitriol. In Alsafran et al, the effect of oral calcitriol given 0.5 mcg twice daily for 5 days prior to surgery (n = 41) on post-operative IV calcium requirement was compared to no pre-operative calcitriol (n = 40). The need for post-operative IV calcium was determined by symptoms of hypocalcemia, serum calcium <1.75 mmol/L, or surgeon preference. Those who received pre-operative calcitriol required post-operative IV calcium less often than controls (34% vs 90%, OR = 0.06, P < .001). In Ferreira et al, 2 mcg of oral calcitriol was given daily for 10 days prior to surgery and was continued post-operatively (n = 45); there was no comparison group. The outcome of interest was incidence of HBS, defined as serum calcium <2.1 mmol/L for 4 or more days post-operatively, which occurred in 28.3% (n = 13) of the participants. While risk factors for developing HBS including high pre-operative PTH, ALP, and longer duration of pre-operative kidney replacement therapy were identified, the treatment effect could not be measured due to lack of a control group. Pre-operative calcium level was not associated with risk of HBS. We were unable to meta-analyze study-specific effects for this type of intervention due to the low number of included studies.
Pre-operative cinacalcet
Three studies evaluated the impact of pre-operative cinacalcet on post-operative calcium outcomes.28-30 In Baker et al, pre-operative treatment with cinacalcet (n = 34) with a median dose of 60 mg (interquartile range [IQR] = 30, 90) and median duration 1 year (IQR = 1, 2 years) was compared to no pre-operative cinacalcet (n = 68). There was no difference in the median post-operative serum calcium (2.02 ± 0.3 mmol/L vs 2.05 ± 0.27 mmol/L, P = .72), nor in the number requiring IV calcium post-operatively (42% vs 25%, P = .07) in the cinacalcet vs no cinacalcet group; however, risk of hypocalcemia and HBS were not reported. In Meyers et al, pre-operative cinacalcet (n = 14) was compared to traditional medical therapy (no further clarifying information) (n = 63). There was no difference in the mean nadir serum calcium post-operatively (1.55 ± 0.32 mmol/L vs 1.65 ± 0.32 mmol/L; P > .05). More individuals receiving pre-operative cinacalcet required IV calcium post-operatively (64% vs 40%), but this was not statistically significant (P = .09) and did not translate to any difference in length of hospital stay (5.3 ± 2.7 days vs 5.5 ± 5.5 days). Need for IV calcium post-operatively was determined by symptomatic hypocalcemia or profound hypocalcemia (defined as serum calcium <1.5 mmol/L). Wirowski et al examined pre-operative treatment with cinacalcet (n = 56) with a median dose of 60 mg (IQR = 30, 90) and a mean duration 18 months (±14), compared to a control (n = 54). While the lowest post-operative serum calcium was lower in the cinacalcet group (1.75 ± 0.37 mmol/L vs 1.86 ± 0.35 mmol/L, P = .048), there was no difference in the number requiring IV calcium (14% vs 11%, P = .776) or symptomatic hypocalcemia (25% vs 22%, P = .824).
Pre-operative alkaline phosphatase to guide intravenous calcium administration
Three studies used pre-operative ALP levels to develop equations to guide IV calcium administration following parathyroidectomy.18,31,32 Ge et al studied a prediction equation using pre-operative PTH and ALP levels to establish IV calcium supplementation regimen initiated immediately post-operatively for 66 hours (n = 74), compared to a strategy where IV calcium dose was titrated based on post-operative serum calcium (n = 22). The mean pre-operative ALP levels were 423.9 ± 351.7 U/L in the intervention group and 449.5 ± 434.4 U/L in the control group. While the cumulative amount of IV calcium received and median post-operative serum calcium at 42 hours were comparable between the 2 groups, the occurrence of post-operative hypocalcemia <2.1 mmol/L at 42 hours was only reported in the intervention group (n = 19, 25.7%). In Liu et al, a preventive calcium supplementation regimen according to pre-operative ALP (n = 126) was compared to conventional calcium supplementation according to post-operative serum calcium levels (n = 145). Patients in the intervention group were stratified into low-risk (pre-operative ALP <500 U/L) and high-risk (pre-operative ALP >500 U/L) to predict their daily calcium requirements, which were started immediately post-operatively. Compared to the control group, the intervention group had a lower risk of hypocalcemia <2 mmol/L (46.0% vs 74.5%, P < .001; OR = 0.292, CI = 0.175-0.488) and severe hypocalcemia <1.875 mmol/L (31.7% vs 64.1%, P < .001) within 48 hours. Goh et al compared a calcium infusion protocol based on pre-operative ALP (stratified by ALP <500 U/L, 500-700 U/L, and >700 U/L) started immediately after surgery (n = 34) with an oral calcium titration based on post-operative calcium levels (n = 44). They reported on mean length of hospital stay (3 days vs 5 days, P < .001) and occurrence of symptomatic hypocalcemia (0% vs 4.55%), which were both lower in the intervention group compared to control group.
Pre-operative pamidronate
Only 1 study investigating bisphosphonate therapy was identified. 33 Davenport et al investigated the effect of pamidronate administration (30 mg disodium pamidronate in patients <80 kg, and 45 mg in patients >80 kg) at 24 to 48 hours before surgery (n = 27) in addition to standard peri-operative management, compared to no pamidronate (n = 10) on severe post-operative hypocalcemia. The pamidronate group had a lower rate of post-operative hypocalcemia, defined as serum calcium <2.1 mmol/L and ionized calcium <0.95 mmol/L (3.7% vs 100%; OR = 0.003, CI = 0.000-0.072), symptomatic hypocalcemia (0% vs 20%), requirement of IV calcium (7.4% vs 100%), and length of hospital admission (5.4 ± 2.3 days vs 9.2 ± 1.9 days) compared to the control group.
Summary of Effect on Risk of Hypocalcemia
ORs for the risk of post-operative hypocalcemia (defined as serum calcium <2.1 mmol/L or ionized calcium <0.95 mmol/L) could only be identified or calculated for 2 of the studies. In Lui et al, using IV calcium guided by pre-operative ALP, the OR was 0.292 (CI = 0.175-0.488). In Davenport et al, using pamidronate pre-operatively, the OR was 0.003 (CI = 0.000-0.072). Due to the lack of similar outcome reporting in studies with comparable interventions, a meta-analysis of study-specific effects was not possible. We received no responses to requests made to corresponding authors for additional data to enable meta-analysis.
Risk of Bias
Risk of bias was assessed using the ROBINS-I tool, 23 as per recommendations from the Cochrane Collaboration for non-randomized studies (Table 2). One study was assessed as low risk of bias, 33 7 were moderate risk of bias,18,26-28,30-32 and 1 was serious risk of bias. 29 Among the studies that provided comparisons between intervention and control groups, only 3 performed measures to control for baseline characteristics,26,28,32 while the others did not explicitly address potential confounders. Risk of outcome reporting bias was assessed using the ORBIT tool 24 (Table 3). Outcomes included in the assessment were incidence of hypocalcemia, HBS, and symptomatic hypocalcemia. Overall, there was a high risk of outcome reporting bias for these outcomes.
ROBINS-I Tool for Risk of Bias.
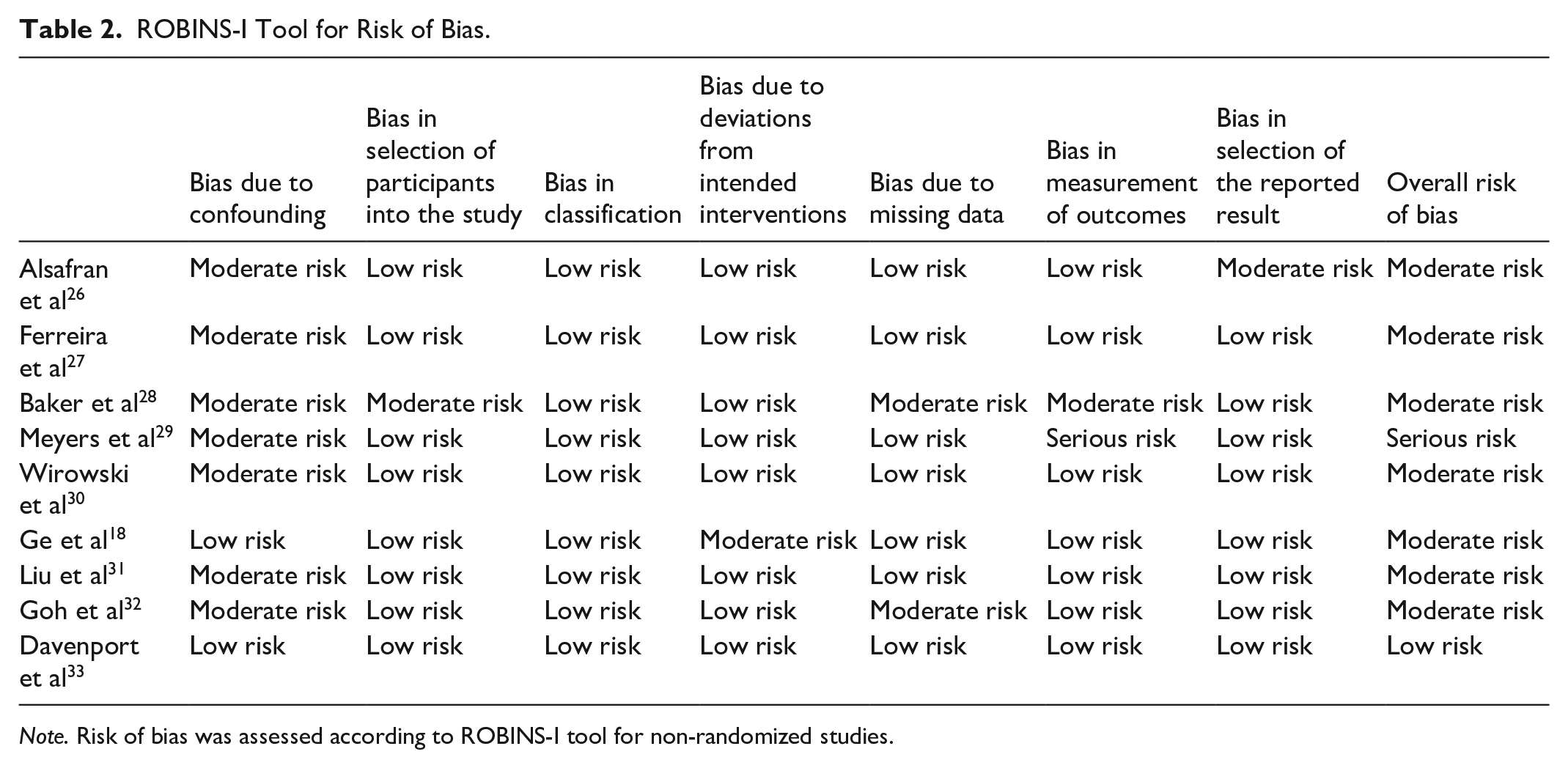
Note. Risk of bias was assessed according to ROBINS-I tool for non-randomized studies.
ORBIT Tool for Risk of Outcome Reporting Bias.

Legend: full reporting ( ), partial reporting (
), partial reporting ( ), not measured (
), not measured ( ), or study did not report the outcome but it is not clear whether the outcome was measured or not (
), or study did not report the outcome but it is not clear whether the outcome was measured or not ( ).
).
Classifications: A: Trial report states that outcome was analyzed but only reports that the result was not significant (typically stating P > .05). B: Trial report states that outcome was analyzed but only reports that the result was significant (typically stating P < .05). C: Trial report states that outcome was analyzed but insufficient data were presented for the trial to be included in meta-analysis or to be considered to be fully tabulated. D: Trial report states that outcome was analyzed, but no results reported. E: Clear that the outcome was measured. Judgment says outcome likely to have been analyzed but not reported because of non-significant results. F: Clear that the outcome was measured. Judgment says outcome unlikely to have been analyzed. G: Not mentioned but clinical judgment says likely to have been measured and analyzed but not reported on the basis of non-significant results. H: Not mentioned but clinical judgment says unlikely to have been measured at all. I: Clear that the outcome was not measured.
Certainty of Evidence
The certainty of evidence was evaluated using the GRADE approach (Supplemental Figures 1-4). Data were summarized narratively, given heterogeneity in outcome reporting. 34 The outcomes of interest for each intervention type had at least 1 domain with serious concern in the certainty assessment. This translated to a low certainty of evidence overall.
Discussion
In this systematic review, we summarized the available evidence of pre-operative interventions aimed at reducing the risk of post-operative hypocalcemia or HBS after parathyroidectomy in patients with kidney disease and sHPT. Of the 9 included studies, interventions had mixed effects on post-operative hypocalcemia and HBS. Whereas pre-operative cinacalcet was not associated with these outcomes, findings suggest possible benefit with pre-operative calcitriol, ALP-guided calcium therapy, and pamidronate. However, few studies were included overall and had high heterogeneity in outcome reporting; therefore, it was not appropriate to meta-analyze study-specific effects. Most of the studies (7 of 9) were assessed as being at moderate risk of bias, and the overall certainty of evidence was low. These findings support a need for further research, optimally with randomized trials.
Studies have recommended use of pre- and post-operative calcitriol and elemental calcium in those with sHPT undergoing parathyroidectomy. 6 A study by Niramitmahapanya et al 35 examined different calcitriol replacement strategies started immediately post-operatively and found that a loading dose regimen (starting dose of 2.25-4 mcg/day) significantly reduced the amount of IV calcium gluconate required compared to a fixed or titrated dose (P = .001). Similarly, a small RCT of 14 patients found the group that received immediate post-operative calcitriol supplementation had higher mean calcium and lower mean calcium replacement. 36 Among patients with primary hyperparathyroidism, an RCT found the group that received pre-operative calcitriol had a significantly higher calcium level at 48 hours post-operatively compared to the control group and had lower rates of symptomatic hypocalcemia (P = .002 and <.001, respectively). 37 Our review included 2 studies of pre-operative calcitriol loading, one of which was a retrospective cohort study, and the other was a retrospective study with no control. The former found the intervention significantly reduced the need for post-operative IV calcium, while the latter reported the incidence of HBS but had no comparison group.26,27 Future RCTs of calcitriol loading in patients with sHPT are needed, perhaps with alternate dosing strategies of pre-operative calcitriol loading.
Calcimimetics have become a standard medical therapy for patients with CKD-related sHPT;38-41 therefore, many patients with medication-refractory sHPT requiring a parathyroidectomy are on a calcimimetic pre-operatively. There are no guidelines to our knowledge on the timing of discontinuation of these agents pre-operatively. While there have been case reports of cinacalcet-induced HBS,42,43 others postulate that cinacalcet my attenuate the severity of HBS. 30 Furthermore, those on cinacalcet who require surgical management due to failure of medical therapy may have greater disease duration and severity. Three studies in our review examined the post-operative course in patients treated pre-operatively with cinacalcet, compared to no cinacalcet. Two studies found no difference in post-operative calcium levels28,29 while 1 study found the nadir post-operative calcium was lower in the cinacalcet group but there was no difference in the number of patients requiring IV calcium or rate of symptomatic hypocalcemia. 30 Overall, in the limited literature we identified, pre-operative cinacalcet does not seem to significantly alter the post-operative course of those undergoing parathyroidectomies.
Elevated pre-operative ALP is an established risk factor for post-operative hypocalcemia and HBS.6,9,11 Our review identified 3 studies that utilized pre-emptive calcium infusion strategies guided by pre-operative ALP levels, often compared to reactive strategies based on post-operative calcium levels.18,31,32 These studies employed equations using ALP as a continuous variable, 18 ordinal variable, 32 and a dichotomous variable. 31 While these studies reported on different outcomes and employed different infusion algorithms, their findings that pre-operative ALP could predict post-operative calcium requirements suggest this may be an effective pre-emptive strategy for management.
The role of pre-operative bisphosphonates in preventing HBS has been proposed; 44 however, studies remain limited. While seemingly paradoxical, given bisphosphonates are known to lower serum calcium, it is hypothesized that through osteoclast inhibition pre-operatively, there may be fewer remodeling spaces on the bone and therefore less unopposed mineralization post-operatively. 6 Although physiologically different than sHPT, a study of patients with primary hyperparathyroidism concluded that pre-operative administration of bisphosphonates was associated with reduced risk of developing HBS post-operatively; however, this was a case-control study with inferential limitations. 45 Our review only identified 1 study investigating the use of pre-operative pamidronate for patients with sHPT undergoing parathyroidectomy. 33 They found, among the group treated with pamidronate compared to no pamidronate, that there was a significant reduction in post-operative hypocalcemia, symptomatic hypocalcemia, IV calcium requirements, and length of hospitalization. More studies are needed to corroborate these findings and to explore the long-term effect on bone mineral density in patient with advanced CKD treated with bisphosphonates.
To our knowledge, this is the first systematic review of pre-operative interventions aimed to reduce the risk of hypocalcemia and HBS among patients with sHPT undergoing parathyroidectomies. While conducted in a comprehensive and methodologically rigorous manner, our study has several limitations that should be considered when interpreting its results. There was significant heterogeneity of outcome reporting among the studies, which limited the ability for any pooled analyses and contributed to substantial outcome reporting bias. Given this, the GRADE analysis had to be summarized narratively rather than numerically. Although all but 2 included studies measured and reported on the average post-operative serum calcium level, only 3 studies reported on the risk of post-operative hypocalcemia. Furthermore, only 1 study reported on but did not include a comparison group. There were 4 studies that reported on symptomatic hypocalcemia; however, only 2 provided definitions for it. We hypothesize that many of these issues could have been ameliorated with more complete reporting. There were no RCTs that met the inclusion criteria for our review, and thus, assessment of publication bias using methods designed for RCTs such as a funnel plot or Egger’s test could not be performed.
In conclusion, post-operative hypocalcemia and HBS are serious and potentially life-threatening consequences following parathyroidectomy in patients with CKD and sHPT. In this review, we identified 4 different pre-operative treatment strategies described in existing literature, including oral calcitriol loading, cinacalcet, IV calcium infusions guided by pre-operative ALP levels, and pamidronate. While some of these treatments have promising post-operative effects, available evidence is not sufficient to inform practice recommendations, and future randomized trials are needed in this population.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251358144 – Supplemental material for Interventions to Reduce the Risk of Hypocalcemia After Parathyroidectomy for People With Advanced Chronic Kidney Disease: A Systematic Review
Supplemental material, sj-docx-1-cjk-10.1177_20543581251358144 for Interventions to Reduce the Risk of Hypocalcemia After Parathyroidectomy for People With Advanced Chronic Kidney Disease: A Systematic Review by Adina Landsberg, Nicole K. Brockman, Emir Sevinc, Caitlin McClurg, Meghan J. Elliott, Louis-Philippe Girard, Matthew T. James, Alexander A. Leung, Neesh I. Pannu, Meghann Pasternak, Paul E. Ronksley, Marcello Tonelli and Tyrone G. Harrison in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
None.
ORCID iDs
Author Contributions
N.B. and T.G.H.: contributed to research idea and study design. A.L., N.B., and T.G.H. contributed to study screening and selection. A.L. and T.G.H. contributed to data extraction. E.S., A.L., and T.G.H. contributed to statistical analysis. All authors contributed to data analysis and interpretation and drafting of manuscript. Each author contributed important intellectual content during manuscript drafting or revision and agrees to be personally accountable for the individual’s own contributions and to ensure that questions pertaining to the accuracy or integrity of any portion of the work, even one in which the author was not directly involved, are appropriately investigated and resolved, including with documentation in the literature if appropriate.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: T.G.H. is supported by a Kidney Research Scientist Core Education and National Training Program New Investigator Award (cosponsored by the Kidney Foundation of Canada and Canadian Institutes of Health Research) and is supported as a new investigator by the Roy and Vi Baay Chair for Kidney Research and the Kidney Health and Wellness Institute at the University of Calgary. These funding sources had no role in study design, data collection, analysis, reporting, or the decision to submit for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data have been summarized and provided in detail in the main manuscript and supplementary material. If there are additional data of interest, the authors will provide if feasible.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.