
Abstract
Background:
There are limited data on the outcomes following medical management alone versus revascularization (percutaneous coronary intervention [PCI] or coronary artery bypass grafting [CABG]) after coronary angiography in kidney transplant recipients.
Objective:
The objective was to compare survival and graft loss in kidney transplant recipients treated with medical therapy alone versus coronary revascularization following coronary angiography.
Design:
We conducted a retrospective, population-based cohort study using linked health care databases.
Setting:
This study was conducted in Alberta, Canada.
Patients:
We included adult, kidney-only transplant recipients between January 1997 and March 2015 who survived at least 1-year post-transplant with a functioning graft and had a coronary angiography during follow-up.
Measurements:
The outcomes were all-cause mortality, death-censored graft failure, death with a functioning graft, and all-cause graft failure.
Methods:
We ascertained baseline characteristics, covariate information, and outcome data from the Alberta Kidney Disease Network (AKDN) and Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (APPROACH) databases. We used Cox proportional hazards models to compare mortality and graft loss between recipients treated with medical management versus revascularization (PCI or CABG) following angiography.
Results:
We identified 142 kidney transplant recipients who received a coronary angiography: 69 (49%) were treated with medical management, and 73 (51%) were treated with revascularization (PCI n = 52, CABG n = 21). The median age was 60 years (interquartile range [IQR] 50-66), 76% were male, the median baseline estimated glomerular filtration rate (eGFR) was 54 mL/min/1.73 m2 (IQR 41-69), and the median follow-up was 5 years (IQR 2-8). Compared to medical management, recipients treated with revascularization did not have statistically higher risk of all-cause mortality (55% vs 62%; 80 vs 102 events/1000 person-years; adjusted hazard ratio [aHR] 1.32, 95% CI 0.86-2.02; P = .21). There was no significant difference in death-censored graft failure between the two treatment groups (20% vs 22%; 33 vs 40 events/1000 person-years; aHR 1.22, 95% CI 0.58-2.58; P = .60).
Limitations:
The clinical indications for medical management alone versus revascularization might influence the choice of these interventions. Due to the smaller sample size, we could not present the outcomes by PCI versus CABG. We also did not have complete data on blood pressure, body mass index, or medication usage which might have influenced our outcomes.
Conclusions:
In kidney transplant recipients undergoing coronary angiography, the rate of mortality was more than double that of graft failure, regardless of post-angiography management of coronary artery disease. The high overall risk for both groups requires further exploration in larger cohorts with longer follow-up.
Introduction
Cardiovascular disease is the leading cause of morbidity and mortality in kidney transplant recipients, largely driven by an increased risk of coronary artery disease. 1 Although, transplantation provides a long-term survival benefit compared to maintenance dialysis, cardiovascular events cause up to 25% of all deaths in transplant recipients.2-4 As a standard of care, the pre-transplant workup usually includes a non-invasive evaluation for coronary artery disease; therefore, the risk of coronary artery disease in transplant recipients is likely different than that of the general population.
Coronary artery disease is usually treated either with medical management or revascularization with percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). However, for kidney transplant recipients with coronary artery disease, the optimal approach for management has not been established, as this population has often been excluded from clinical trials and is not addressed in current clinical practice guidelines. 5 Prior observational studies that have assessed revascularization in kidney transplant recipients are limited by a lack of a comparative medical therapy group, short follow-up durations (e.g. median follow-up ranging from 21-42 months),6-8 small sample sizes, and missing data on relevant confounders, including coronary anatomy and left ventricular ejection fraction.
One study from Alberta, Canada showed that for patients with chronic kidney disease, revascularization with CABG was associated with better survival compared with medical therapy. 9 However, this study did not include kidney transplant recipients. In this population-based study, we compared survival and graft loss following coronary angiography in kidney transplant recipients in Alberta treated with medical therapy alone versus coronary revascularization.
Methods
Design, Setting, and Data Sources
We followed a pre-specified protocol approved by the research ethics board of the University of Calgary, including a waiver of patient consent to use routinely collected health data. We reported this study according to STROBE and RECORD guidelines for observational studies using routinely collected data (Supplemental Table S1). This retrospective, population-based cohort study used linked healthcare datasets within the Alberta Kidney Disease Network (AKDN) database, which incorporates data from Alberta Health, Alberta Kidney Care programs, and the provincial health ministry. 10 Over 99% of Alberta residents are registered with Alberta Health and have universal access to hospital care and physician services. The AKDN database was linked with the Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (APPROACH) registry, which prospectively collects detailed information on all patients undergoing coronary angiography in Alberta since 1995. The registry includes the indication and results of cardiac catheterization. 11 We ascertained baseline characteristics, covariate information, and outcome data from the AKDN database and APPROACH records. These databases have been used extensively to look at outcomes in kidney transplant recipients and in patients with chronic kidney disease, including those treated with dialysis.9,12-17
Population
We included all incident adult, kidney-only transplant recipients who received their transplant between January 1, 1997 and March 31, 2015 in Alberta, Canada. We identified kidney transplant recipients from 1997-2000 using diagnostic and procedural codes and from 2001 onwards using data from the Alberta Kidney Care (AKC) North and South programs, which provide care to all patients in the province treated with kidney replacement therapy, including maintenance dialysis and kidney transplantation. We excluded pediatric recipients (<18 years old) and recipients of a previous non-kidney organ transplant or a simultaneous multi-organ transplant, including kidney-pancreas. Recipients were excluded if they died or experienced graft failure (defined as return to maintenance dialysis or re-transplant) within the first year of their transplant. Thus, recipients included in our study must have survived at least 1-year post-transplant with a functioning graft.
From the APPROACH database, we identified kidney transplant recipients who had a coronary angiography at 1 year or later from their transplant date. This 1-year timeframe would exclude unstable recipients who might have an outcome from immediate or delayed transplant-related complications rather than from our exposure of interest. For recipients with multiple angiographies during follow-up, analyses were based on the first angiography after transplant.
Exposure
Recipients were categorized as receiving medical management alone versus treatment with revascularization, including PCI or CABG, defined by the first procedure occurring within 1 year of the first coronary angiography. 9 The cohort creation is shown in Supplemental Figure S1 and the study design is shown in Supplemental Figure S2.
Baseline Characteristics
Baseline characteristics were ascertained on the date of the angiography (index date). Demographic data, including age and sex, were determined from the Alberta Health administrative database. We used the Alberta Health database (1994-2000) and the AKC North and South program databases (from 2001 onwards) for transplant-related data, including pre-transplant dialysis duration. Relevant comorbidities were defined using validated algorithms, whenever possible (Supplemental Table S2), and identified by the presence of one or more diagnostic codes using the AKDN database from April 1994 up to and including the index date, using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and International Statistical Classification of Diseases, Tenth Revision (ICD-10) coding algorithms for physician claims and hospitalization data.18,19 Graft function, including estimated glomerular filtration rate (eGFR) and albuminuria, was ascertained using laboratory data available from 2002 onwards as laboratory data prior to this year were not available from the AKDN database. The baseline eGFR (using the Chronic Kidney Disease Epidemiology Collaboration [CKD-EPI] 2009 equation) was calculated using the mean of all outpatient serum creatinine measurements in the three months prior to and including the index date.10,20
Hyperlipidemia and smoking status were obtained from the APPROACH database at the time of coronary angiography.9,11,21 The indication for coronary angiography was also obtained from APPROACH, as previously described,22-24 as was information on left ventricular ejection fraction and the affected coronary vessels (a coronary vessel was considered to have disease if there was at least 50% stenosis).
Outcomes
Participants were followed from the date of first angiography (index date) until the first of death, graft failure, with censoring for emigration, or at the end of study period (March 31, 2019). In Alberta, the rate of emigration was <1% during the study. 25 The outcomes were all-cause mortality and death-censored graft failure (defined as return to maintenance dialysis or re-transplant identified from Alberta Health and Alberta Kidney Care programs). We also examined death with a functioning graft (defined as post-transplant death without evidence of return to maintenance dialysis or re-transplant) and all-cause graft failure (defined as post-transplant death with a functioning graft, return to maintenance dialysis, or re-transplant).
Statistical Analysis
We described the baseline characteristics using medians and frequencies where appropriate. We compared baseline characteristics between transplant recipients treated with medical management only versus revascularization using comparative statistics (Chi-square or Kruskal-Wallis, where appropriate). Cumulative incidence curves were plotted for all four outcomes by treatment groups (Figure 1).

Cumulative incidence curves by revascularization versus medical management alone for (A) all-cause mortality; (B) graft failure; (C) death with a functioning graft and (D) all-cause graft failure (composite).
Cause specific Cox proportional hazards models were used to compare survival across the treatment groups (medical management versus revascularization) for each outcome adjusting for age and sex (adjusted hazard ratio [aHR] with 95% confidence intervals [CI]). Given the variable time from the index coronary angiography to PCI or CABG, revascularization was modeled as a time-varying exposure to avoid immortal time bias. 26 We performed a sensitivity analysis excluding the recipients with normal coronary anatomy and minimal coronary artery disease and presented cumulative incidences and aHR. Statistical analyses were performed using R version 4.2.0 (R-project.org).
Results
Cohort Formation and Characteristics
Of the 2346 kidney transplant recipients identified during the study period, 45 recipients who experienced graft failure before their angiography and 1 recipient who experienced graft failure between their angiography and revascularization were excluded (Figure S1). As such, 142 recipients with a post-transplant angiography were included in the study. The baseline characteristics are shown in Table 1. Overall, the median age was 60 years (interquartile range [IQR] 50-66) and 76% were male. The median eGFR was 54 mL/min/1.73 m2 (IQR 41-69) at the time of cohort entry. Of the 142 recipients who received an angiography, 69 (49%) were treated with medical management alone and 73 (51%) were treated with revascularization (PCI n = 52, CABG n = 21). The median time from kidney transplant to angiography was 5.3 years (IQR 2.7-8.4). The median time from angiography to coronary revascularization was 1 day (IQR 1-1) for the PCI group and 45 days (IQR 9-64) for the CABG group. Recipients treated with medical management only were more likely to have heart failure at baseline compared to recipients treated with revascularization (48% vs 27%, P = .01).
Baseline Characteristics of Kidney Transplant Recipients at the Time of Coronary Angiography.

Note. Data are presented as number (%) or as median [interquartile range]. APPROACH = Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease; CABG = coronary artery bypass graft; eGFR = estimated glomerular filtration rate; NSTEMI = non-ST segment elevation myocardial infarction; PCI = percutaneous coronary intervention; pLAD = proximal left anterior descending coronary artery; PVD = peripheral vascular disease; STEMI = ST segment elevation myocardial infarction; TIA = transient ischemic attack.
Laboratory data was available from 2002 onwards.
Assessed by the presence of diagnostic or procedural codes, based on validated algorithms, where applicable, from April 1994 and/or identified from the APPROACH database, from January 1995 up to and including the index date (Supplemental Table S2).
For recipients treated with medical management only, the most common indication for angiography was stable angina (42%), whereas for recipients treated with revascularization, the most common indication was myocardial infarction (45%). Compared to recipients treated with medical management only, the recipients treated with revascularization were more likely to have left main or 3 vessel disease (medical management vs revascularization: 30% vs 53%). There was no significant difference in left ventricular ejection fraction between the two groups, although there was a high proportion of recipients in both groups without measurements (74% vs 68%).
Outcomes
Study participants had a median follow-up of 5 years (IQR 2-8) and a maximum follow-up of 19 years. For the 142 recipients, 61 (43%) died (medical management vs revascularization: 27 vs 34), 30 (21%) experienced graft failure (14 vs 16), 6 (4%) emigrated from the province (2 vs 4), and 45 (32%) were event-free at the study end date (26 vs 19). During follow-up, 91 (64%) kidney transplant recipients experienced all-cause graft failure.
Compared to recipients in the medical management group, the 1- and 5-year cumulative incidence of all-cause mortality was higher in recipients treated with revascularization (1-year incidence, medical management versus revascularization: 6% vs 16%; 5-year incidence: 28% vs 35%); however, by 10 years, the cumulative incidence was similar in both groups (10-year incidence: 62% vs 68%; Figure 1). Similar differences were noted for death with a functioning graft and all-cause graft failure. For graft failure, there was no difference in the cumulative incidences between the medical management and revascularization groups throughout the study period (5-year incidence: 12% vs 11%; 10-year incidence: 24% vs 23%).
Compared to recipients treated with medical management, those treated with revascularization had no statistically significant difference in incidence of all-cause mortality (55% vs 62%; 80 vs 102 events/1000 person-years; aHR 1.32, 95% CI 0.86-2.02; P = .21). Death-censored graft failure was less common, with no significant difference between treatment groups (20% vs 22%; 33 vs 40 events/1000 person-years; aHR 1.22, 95% CI 0.58-2.58; P = .60). All-cause graft failure was similar in both groups (59% vs 68%, 98 vs 126 events/1000 person-years; aHR 1.38, 95% CI 0.91-2.08; P = .12) (Table 2 and Figure 2).
Outcomes for Kidney Transplant Recipients According to Revascularization or Medical Management Alone.
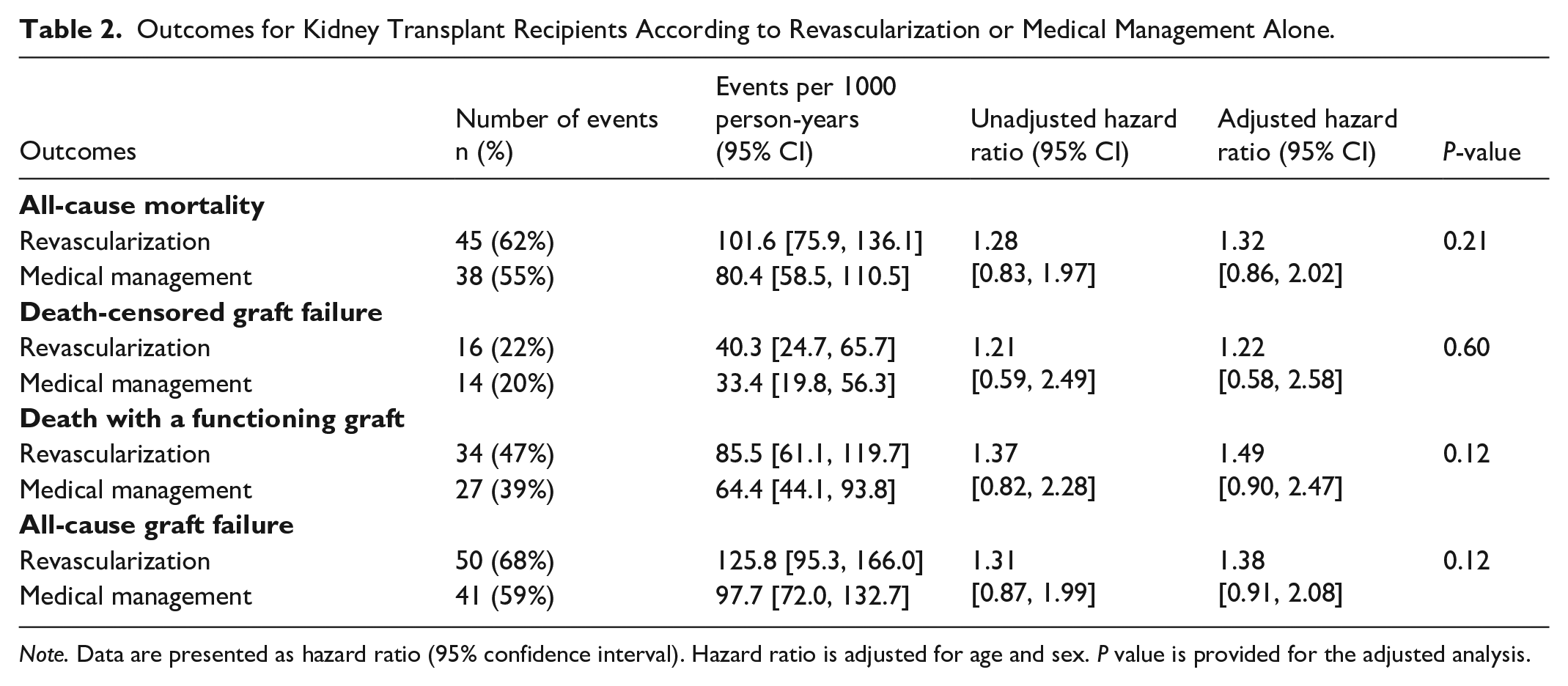
Note. Data are presented as hazard ratio (95% confidence interval). Hazard ratio is adjusted for age and sex. P value is provided for the adjusted analysis.

The relative hazards of outcomes with revascularization compared to medical management alone following coronary angiography among kidney transplant recipients.
Sensitivity Analysis
We excluded the recipients with normal coronary anatomy (n = 13) and minimal coronary artery disease (n = 14) resulting in 115 participants with moderate-to-severe coronary artery disease who were included in the sensitivity analysis. Compared to recipients treated with medical management only, the 1-year cumulative incidence of all-cause mortality was higher in recipients treated with revascularization (1-year incidence, medical management vs revascularization: 6% vs 17%); however, by 5 and 10 years, the cumulative incidence was similar in both groups (5-year incidence: 35% vs 34% and 10-year incidence: 67% vs 69%). Cumulative incidences were similar for graft failure at 5 years and 10 years (Supplemental Figure S3). There was no statistically significant difference while comparing recipients treated with medical management with those treated with revascularization for all-cause mortality (aHR 1.23, 95% CI 0.76-2.00) or death-censored graft failure (aHR 1.25, 95% CI 0.49-3.19) (Supplemental Figure S4).
Discussion
In this retrospective, population-based cohort study of 142 adult kidney transplant recipients who received coronary angiography, we found that approximately half of the recipients were treated with medical management alone, and the other half received revascularization with either PCI or CABG. All-cause mortality was more than twice as common as graft failure at 5 years following angiography. There were important differences between transplant recipients who received medical management versus revascularization, including a higher prevalence of heart failure and a lower burden of coronary disease in the medical management group. In the first 5 years of follow-up, kidney transplant recipients treated with revascularization had a higher incidence of all-cause mortality than the medical management group; however, this difference became similar between the two groups after 10 years of follow-up. There was no significant difference in graft failure between the medical management group and the revascularization group. The results were similar when we restricted our analyses to recipients with moderate-to-severe coronary artery disease.
Our findings suggest that patients treated with revascularization may be at higher risk of early mortality than those who received medical management. This differs from what has been reported in some observational studies of non-transplant patients with kidney disease. For example, Hemmelgarn et al 9 found a lower risk of mortality for non-transplant patients with kidney disease treated with revascularization compared to those who received medical therapy alone, including patients who were dialysis-dependent. Due to the anticipated small number of events, we combined recipients treated with PCI and CABG in the revascularization group, rather than examining them separately. Thus, we did not explore differences in outcomes between patients treated with PCI or CABG. Early mortality post-revascularization could be due to the more frequent presentation with an acute coronary syndrome or more extensive coronary disease in this group, or mediated by re-stenosis post-PCI or post-procedure complications, such as acute kidney injury, bleeding, and infection.8,27 In a single-center retrospective study of kidney transplant recipients, the incidence of bleeding complications was 26% for the combined PCI and CABG group. Following CABG, 46% of recipients had re-operations due to bleeding complications, wound infections, and compartment syndrome, while in the PCI group, 48% of recipients had repeated PCI due to in-stent re-stenosis and de-novo lesions. 8 In the general population, the incidence of re-operation due to bleeding complications following CABG has been reported to be 2.3% to 8.0% while the incidence of re-stenosis following PCI has been reported to be 20% to 30%, suggesting that post-revascularization complications may be higher in kidney transplant recipients compared to the general population.28,29
Our cohort of kidney transplant recipients differed from the patients with chronic kidney disease included in the study by Hemmelgarn et al 9 which may explain the higher incidence of mortality in our study. The transplant recipients in our study were younger, but were more likely to have cardiac risk factors, such as hypertension, diabetes, and dyslipidemia. Also, transplant recipients who received coronary angiography were more likely to have myocardial infarction as the indication for angiography, and less likely to have minimal (less than 50%) stenosis compared to the dialysis-dependent patient population. Therefore, transplant recipients receiving invasive coronary procedures may have more frequent acute coronary syndromes and coronary artery burden contributing to poor outcomes.
We did not find any statistically significant differences in mortality or graft failure in recipients treated with medical management or revascularization. The ISCHEMIA-CKD randomized controlled trial, which randomized 777 patients with CKD and moderate-to-severe ischemia to invasive versus conservative management for stable coronary artery disease, found that revascularization did not lower the risk of death in comparison to the medical therapy alone; 30 however, this trial included only 24 (3%) kidney transplant recipients, limiting its generalizability to this population. The lack of significant difference in graft failure in kidney transplant recipients treated with medical management or revascularization in our study could be due to advanced surgical and percutaneous practices resulting in reduced graft losses. 27 These include the use of off-pump CABG to reduce the risks associated with cardiopulmonary bypass, less invasive coronary bypass surgery techniques to eliminate the use of extracorporeal circulation, and minimizing the amount of contrast agent used in well hydrated patients to reduce the incidence of potential kidney injury and graft loss.31-33 Most of the kidney transplant recipients in our study were dialysis-dependent prior to transplant, and transplant recipients are generally a healthier sub-segment of the dialysis population given the thorough transplant evaluation and screening process. Kidney transplant recipients undergo pre-transplant cardiac testing for transplant suitability; therefore, they are likely different from patients on maintenance dialysis with respect to atherosclerosis, plaque pathophysiology or degree of vascular calcification. Thus, those with severe untreated cardiac disease or poor prognosis or life expectancy would be unlikely to receive a transplant and be included in our study.
Our study findings have useful clinical implications. The overall age- and sex-adjusted risks of mortality and graft loss were not significantly different between the revascularization and medical management groups; however, mortality was more than 2-fold more common than graft loss. This finding, that the risk of death is much more common than graft failure, can inform clinical decision-making since the majority of deaths in kidney transplant recipients are due to cardiovascular events. This may help discussion of risks with patients, support informed choices, and facilitate shared decision-making between physicians and kidney transplant recipients considering coronary angiography and revascularization decisions. Our results also suggest a need for future studies that include other relevant outcomes following angiography, such as acute kidney injury and major adverse cardiovascular events. The high risk of mortality in both the revascularization and medically treated group highlights the need for further studies to better understand the drivers of this risk and identify interventions that can mitigate this risk in the kidney transplant population.
Our study has a number of strengths. This is a population-based study of kidney transplant recipients who received coronary angiography post-transplant and characterized outcomes in recipients treated with revascularization and with medical management, with a median follow-up time of 5 years and a maximum follow-up of almost 20 years. There are limitations worth noting. First, we acknowledge treatment selection bias is likely present due to the initial clinical decision to proceed with coronary angiography and in the subsequent decision to proceed to revascularization versus medical therapy alone based on the results of the angiography. The recipients treated with revascularization were more likely to receive a coronary angiography due to an acute coronary syndrome, more likely to have severe coronary artery disease, and less likely to have heart failure compared to recipients treated with medical management and our study was too small to effectively adjust for these differences. However, we performed a sensitivity analysis and the results were similar for recipients with moderate-to-severe coronary artery disease. Our study was underpowered to detect clinically important differences in the outcomes studied which may have limited our precision to detect statistically significant differences between the comparison groups. The sample size limited our ability to further examine the outcomes by PCI versus CABG. Third, hypertension is considered as one of the major risk factors for graft loss, cardiovascular disease, and death with a functional graft; however, we did not have available data on blood pressure to include this variable in our analysis. Similarly, we lacked granular data such as body mass index and concurrent medication use that may influence outcomes; there were missing data for left ventricular ejection fraction as ventriculography was likely avoided to reduce contrast volumes in patients at risk of acute kidney injury. Lastly, we did not have complete or reliable data on cause of mortality or cause of graft loss in our datasets.
Conclusions
In conclusion, kidney transplant recipients who received coronary angiography had high mortality that was 2-fold more common than graft failure, whether they were treated with medical management alone or revascularization. An appreciation of these comparative risks of these outcomes can help inform coronary artery disease management decisions in this high-risk population.
Supplemental Material
sj-pdf-1-cjk-10.1177_20543581251358143 – Supplemental material for Mortality and Graft Failure With Medical Management Alone Versus Revascularization After Coronary Angiography Among Kidney Transplant Recipients: A Population-Based Study
Supplemental material, sj-pdf-1-cjk-10.1177_20543581251358143 for Mortality and Graft Failure With Medical Management Alone Versus Revascularization After Coronary Angiography Among Kidney Transplant Recipients: A Population-Based Study by Labib I. Faruque, Robert R. Quinn, Pietro Ravani, Tyrone G. Harrison, Brenda Hemmelgarn, Stephen Wilton, Alix Clarke, Matthew T. James and Ngan N. Lam in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
This study is based in part on data provided by Alberta Health and Alberta Health Services. The interpretation and conclusions contained herein are those of the researchers and do not necessarily represent the views of the Government of Alberta or Alberta Health Services. Neither the Government of Alberta nor, Alberta Health or Alberta Health Services express any opinion in relation to this study. APPROACH received support from Alberta Health Services (Calgary Zone, Edmonton Zone), the Libin Cardiovascular Institute and Mazankowski Alberta Heart Institute.
List of Abbreviations
aHR, adjusted hazard ratio; AKC, Alberta Kidney Care; AKDN, Alberta Kidney Disease Network; APPROACH, Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease; CABG, coronary artery bypass grafting; CI, confidence intervals; CKD-EPI, Chronic Kidney Disease–Epidemiology Collaboration; eGFR, estimated glomerular filtration rate; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; ICD-10, International Statistical Classification of Diseases, Tenth Revision; IQR, interquartile range; PCI, percutaneous coronary intervention.
Ethics Approval and Consent to Participate
This study was approved by the research ethics board of the University of Calgary, including a waiver of patient consent.
Consent for Publication
The authors have consented to publication of this manuscript.
Author Contributions
LIF and NNL participated in the study design and drafted and revised the manuscript. AC performed the data analysis. All authors were involved in data interpretation and final approval of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.