
Abstract
Background:
Previous studies conducted in publicly and privately funded health care systems suggest that access to kidney transplants may vary depending on where a patient receives their kidney care. It is poorly understood whether variability exists across the key steps required to receive a kidney transplant in a publicly funded health care system.
Objective:
To determine whether there is variation across Ontario’s regional renal programs (RRPs) in key steps completed toward receiving a kidney transplant.
Design:
Population-based cohort study from November 1, 2017, to December 31, 2021, using linked administrative health care databases with a maximum follow-up of March 31, 2023.
Setting:
This study includes 27 RRPs and independent health facilities in Ontario, Canada.
Patients:
Patients approaching the need for dialysis and patients receiving maintenance dialysis with no recorded contraindication to kidney transplant.
Measurements:
Key steps toward receiving a kidney transplant, including (1) referred to a transplant center for an evaluation; (2) had a potential living donor contact a transplant center to be evaluated; (3) deceased donor waitlist activation; and (4) received a transplant from a living or deceased donor.
Methods:
For each step toward receiving a kidney transplant, we reported a unique incidence rate per 100 person-years with a 95% confidence interval (95% CI), presented by Ontario’s RRPs, including the 27 RRPs and independent health facilities. We also presented results by 5 Ontario geographic regions. In an additional analysis, we examined the time to complete specific transplant steps.
Results:
We included 8319 individuals approaching the need for dialysis and 4869 individuals receiving maintenance dialysis. During follow-up, 2870 (34.5%) individuals approaching the need for dialysis initiated maintenance dialysis. In individuals approaching the need for dialysis, we found the rate of a potential living kidney donor contacting a transplant center to be evaluated varied more than 17-fold across RRPs from 0.67 (95% CI = 0.1, 4.8) to 11.7 (95% CI = 9.2, 14.9). In the dialysis cohort, the average number of steps completed toward receiving a kidney transplant varied almost 4-fold across RRPs from 11.7 (95% CI = 9.3, 14.8) to 44.0 (95% CI = 38.6, 50.1) steps per 100 person-years. The average rate of each step measured separately also varied widely, with the rate of referral to a transplant center for an evaluation (per 100 person-years) varying across RRPs from 6.0 (95% CI = 4.2, 8.5) to 47.9 (95% CI = 42.6, 53.8), the rate of a potential living kidney donor contacting a transplant center to be evaluated from 1.5 (95% CI = 0.78, 2.9) to 10.7 (95% CI = 7.9, 14.5), the rate of deceased donor waitlisting from 2.9 (95% CI = 1.9, 4.4) to 13.2 (95% CI = 11.0, 15.8), and the rate of kidney transplant from 2.0 (95% CI = 1.1, 3.4) to 12.6 (95% CI = 10.8, 14.8). When examining the results by 5 Ontario geographic regions, we found patients receiving maintenance dialysis in Northern Ontario had substantially lower rates of completing key steps toward receiving a kidney transplant. For example, the rate of transplant referral (per 100 person-years) was almost 3-fold lower in Northern Ontario (10.0, 95% CI = 8.3, 12.0) compared to Toronto (28.7, 95% CI = 25.7, 32.1).
Limitations:
We did not examine the reason for differences in access to kidney transplant across RRPs (eg, differences in physician practices and staff-to-patient ratio).
Conclusions:
Despite operating in a publicly funded health care system, there is substantial variability across the 4 key steps required to receive a kidney transplant.
Trial registration:
Not registered.
Introduction
The best treatment option for most patients with kidney failure is a kidney transplant.1-3 Compared to the alternative treatment of dialysis, a kidney transplant offers patients a better quality of life and improved life expectancy, at a fraction of the cost.3-5 Unfortunately, many barriers prevent eligible patients from receiving a transplant.5-8
In both privately and publicly funded health care systems, previous research has found variability in access to kidney transplant based on where a patient receives kidney care.9-17 In the United States, substantial variation in kidney transplant referral was found across 690 dialysis facilities, with referrals varying from 0% to 100%. 16 In Ontario, Canada, regional renal programs (RRPs) provide dialysis and kidney care services to patients. Substantial variation across RRPs in kidney transplant referral and kidney transplantation has been observed, with the 1-year cumulative probability of referrals varying from 6.4% to 34.5% 12 and the 10-year cumulative incidence of kidney transplant varying from 7.4% to 31.4%. 13 However, these studies were conducted using data that are several years old, and since that time multiple initiatives in Ontario, Canada, 18 have been implemented to improve access to kidney transplant (eg, performance review discussions on kidney transplantation, additional funding toward specific kidney transplant activities, and peer support).
To our knowledge, no previous studies have examined whether variability in several key steps toward receiving a kidney transplant exists across RRPs. It is important to understand if variability exists at each step in the transplant process, with previous work finding unique barriers at each step, 16 potentially requiring distinct solutions. If variability in access to transplant continues to exist across RRPs, this could inform opportunities for interventions to increase equitable access to transplant. Therefore, we conducted this study to determine whether there is variation across Ontario’s RRPs in key steps completed toward receiving a kidney transplant, including (1) referral to a transplant center for an evaluation; (2) having a potential living donor contact a transplant center to be evaluated; (3) deceased donor waitlist activation; and (4) receiving a transplant from a living or deceased donor. We also examined the average number of steps completed toward receiving a kidney transplant and the time to complete key steps in the kidney transplant process.
Methods
Design and Setting
We conducted a population-based cohort study using linked administrative health care databases from Ontario, Canada (population 15.8 million) 19 held at ICES (ices.on.ca/). These data sets were linked using unique encoded identifiers and analyzed at ICES. ICES is an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. ICES is a prescribed entity under Ontario’s Personal Health Information Protection Act (PHIPA). Section 45 of PHIPA authorizes ICES to collect personal health information, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of, the allocation of resources to or planning for all or part of the health system. Projects that use data collected by ICES under section 45 of PHIPA, and use no other data, are exempt from REB review. The use of the data in this project is authorized under section 45 and approved by ICES’ Privacy and Legal Office. We used the Reporting of studies Conducted using Observational Routinely-collected health Data (RECORD) Statement to report this study (Supplementary Table 1). 20
Data Sources
We used several linked administrative databases, including the Ontario Laboratories Information System, for information on serum creatinine and the urine albumin-to-creatinine ratio. We used the Ontario Renal Reporting System database to identify patients receiving care in a multicare kidney clinic and to identify patients receiving maintenance dialysis. The Registered Persons Database was used to determine vital status, while we used the Canadian Institute for Health Information Discharge Abstract Database to identify hospitalizations. The Ontario Health Information Plan (OHIP) was used to identify physician billings and diagnoses. We used data from the Trillium Gift of Life Network to characterize key steps toward receiving a kidney transplant. Further details on databases and coding definitions can be found in Supplementary Table 2.
Study Population
Approaching the need for dialysis
We included adults receiving care in a multicare kidney clinic (ie, a specialized clinic providing multidisciplinary kidney care) and satisfying at least one of the following kidney function criteria: (1) 2 estimated glomerular filtration rate (eGFR) estimates < 15 mL/min/1.73 m2 (estimated using the 2021 CKD-EPI equation without race) 21 or (2) 2 Kidney Failure Risk Equation (KFRE) measures ≥25% (estimating the 2-year probability of kidney failure). 22 The eGFR and KFRE measures had to be separated by at least 90 days but no more than 365 days. The cohort entry date was either (1) the date of the multicare kidney clinic visit (kidney function criteria had to be satisfied within 1-year prior to the visit date) or (2) the date the kidney function criteria was satisfied. If an individual had multiple cohort entry dates, we selected the first qualifying date. We excluded individuals with a recorded contraindication to kidney transplant, as defined in our data sources, including end-stage kidney disease-modified Charlson Comorbidity Index score ≥7 (a higher score represents greater comorbidity), home oxygen use, dementia, living in a long-term care facility, receiving at least one physician house call in the last year, or a history of cancer (ie, lung, lymphoma, cervical, colorectal, liver, active multiple myeloma, and bladder cancer). 23 Based on the previous work, we found that over 97% of individuals who had one or more of the aforementioned transplant contraindications never received a kidney transplant. 23 Last, we excluded individuals who received maintenance dialysis in the 6 months prior to cohort entry.
Maintenance dialysis
We included incident adult patients (18-75 years of age; care for pediatric patients is commonly provided by different health care providers than adults, and after age 75 a kidney transplant is relatively uncommon) 23 receiving maintenance dialysis (either at home or in-center) between November 1, 2017, and December 31, 2021. To ensure we were not capturing patients receiving acute dialysis, the cohort entry date was 90 days after dialysis initiation. We excluded individuals who had a recorded contraindication to transplant as described above. To ensure patients were eligible for the outcome of transplant referral, we excluded individuals who received a kidney transplant referral prior to cohort entry (ie, generally patients are only referred once for transplant). Similarly, when examining the outcome of deceased donor waitlist activation, we excluded individuals who were on the deceased donor waitlist prior to cohort entry.
The cohorts of patients approaching the need for dialysis and patients on maintenance dialysis were not mutually exclusive. If individuals approaching the need for dialysis initiated maintenance dialysis during follow-up, we censored them, and thereafter they started to contribute person-time to the maintenance dialysis cohort, provided they met the maintenance dialysis eligibility criteria.
Outcomes
Steps completed toward receiving a kidney transplant
In Ontario, Canada, there are multiple steps that need to be completed in the process toward receiving a kidney transplant (Figures 1a and b). The primary outcomes were the rate of several key steps in the process toward receiving a kidney transplant, including (1) referral to a transplant center to be evaluated; (2) a potential living donor contacting a transplant center for evaluation (if multiple donors began evaluations for a certain individual, we only counted the first donor); (3) deceased donor waitlist activation; and (4) receiving a living or deceased donor kidney transplant. Each step was examined separately, with each step having its own rate. In the cohort of patients approaching the need for dialysis, we only evaluated 1 step (ie, potential living donor contacting a transplant center for evaluation). In Ontario, Canada, patients approaching the need for dialysis are encouraged to find a living donor, and it is suggested they are referred for transplant when they have found a potential donor; 24 pre-emptive deceased donor transplant is uncommon.
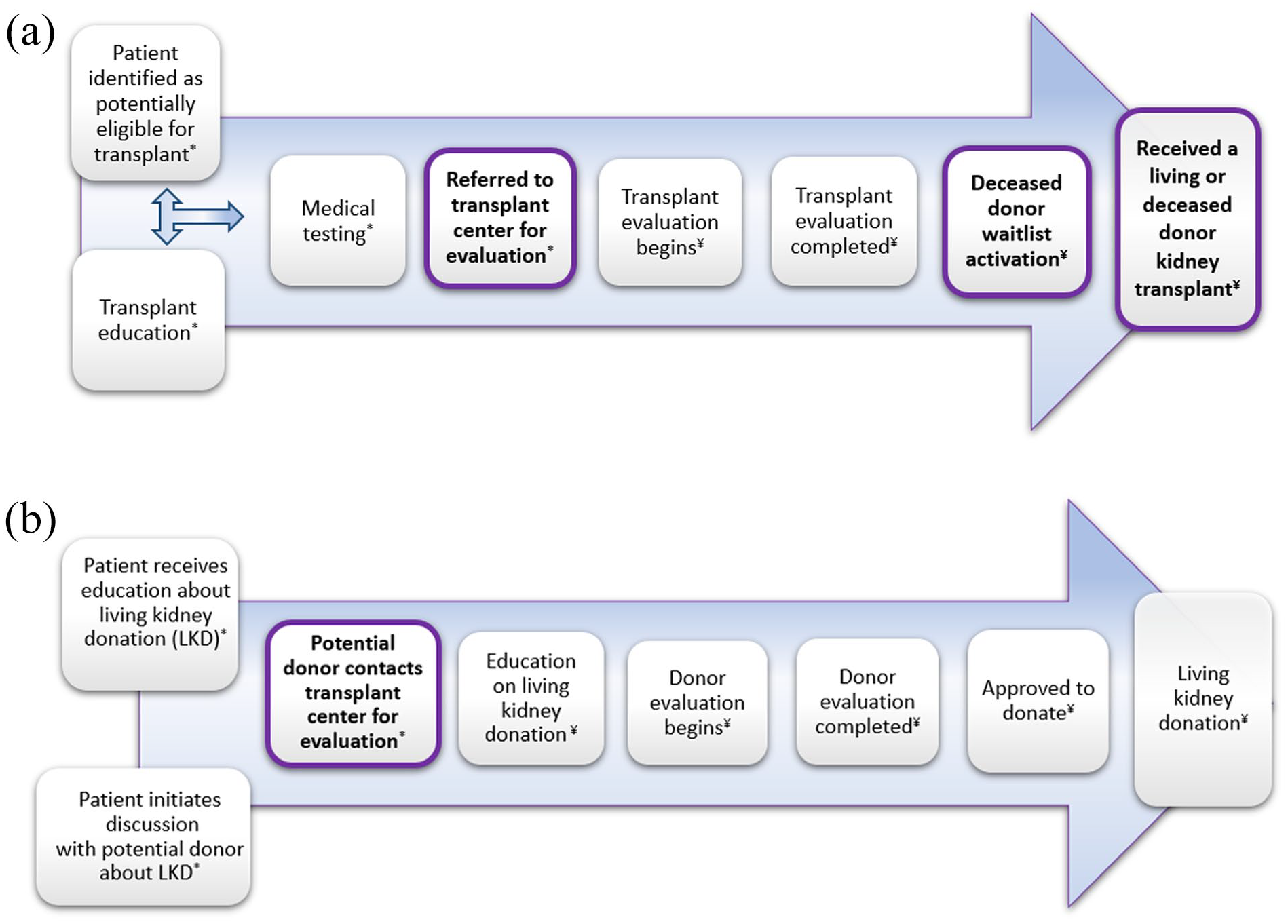
(a) Steps to receiving a living or deceased donor kidney transplant for patients in Ontario, Canada.
In the maintenance dialysis cohort, we also examined the average number of steps completed during the study period toward receiving a kidney transplant (per 100 person-years) (maximum of 4 steps could be completed per individual). Each step could only be counted once.
Time to complete key steps in the kidney transplant process
In an additional analysis, we examined the time to complete specific transplant steps. The details are described in Supplementary Table 3.
Regional Renal Programs
The delivery of kidney services across Ontario is managed by a provincial government agency, the Ontario Renal Network (part of Ontario Health). Twenty-seven RRPs oversee 27 multicare kidney clinics, 27 home dialysis programs, and more than 100 dialysis facilities. All our results are presented by the 27 RRPs. For patients receiving maintenance dialysis, we included a 28th category, independent health facilities (ie, facilities that provide hemodialysis services and are independently owned and operated); at the time of the analysis, there were 7 independent health facilities across Ontario. 26 For simplicity, we describe the results by the 28 RRPs.
We assigned patients to the RRP where they first received their multicare kidney clinic care or initiated maintenance dialysis. We found in previous work that <10% of patients switch RRPs over 1-year of follow-up. 13 To ensure anonymity, we assigned a random number to each RRP.
To better understand the impact of geography on access to kidney transplant, we grouped the 27 RRPs (excluding independent health facilities) into 5 regions that provide integrated health care services, including North, East, West, Central, and Toronto. 27
Statistical Analysis
We reported continuous variables as means (± standard deviation) or medians (25th, 75th percentiles) and categorical variables as proportions. For all outcomes, we reported the rate per 100 person-years (95% confidence interval [CI]). We censored individuals at death, loss to follow-up (ie, no longer eligible for Ontario Health Insurance Plan services), end of study period (March 31, 2023; date of data availability at the time of analysis), or developed a contraindication to transplant (described above), except for age, with individuals who became older than 75 years in follow-up remaining in the study. We reported the time to complete key steps in the kidney transplant process as medians (25th, 75th percentile). In an additional analysis, we allowed individuals to have more than 1 potential living donor contact a transplant center for an evaluation, reporting the mean (standard deviation), median (25th, 75th percentile), and the number of contacts (0, 1, 2, 3+).
Data for baseline information was largely complete except for the following variables: income quintile (<0.5% missing; imputed quintile 3), rural residence (<0.5% missing; imputed urban residence), KFRE (2.5% missing, approaching the need for dialysis cohort only; kept missing category), and body mass index (6.6% missing). While our outcome data were largely complete, some information on referral to a transplant center for an evaluation, a potential living donor contacting a transplant center to be evaluated, and deceased donor waitlist activation was imputed. For example, in Ontario, Canada, a patient cannot be waitlisted without evidence of referral for transplant. If a patient was waitlisted but had no evidence of a prior referral, we imputed the referral date. Less than 1.5% of steps in the transplant process were imputed. The handling of the missing outcome data has previously been described. 18
The widths of confidence intervals were not adjusted for multiple testing. We conducted all analyses using SAS version 9.4 (SAS Institute, Cary, North Carolina).
Additional Analysis
In a post-hoc analysis of the maintenance dialysis population, we examined the rate of each key step completed toward receiving a kidney transplant and the average number of steps completed toward receiving a kidney transplant (per 100 person-years) stratified by RRPs located with an adult transplant center vs RRPs not located with a transplant center. The six RRPs located with a transplant center, included London Health Sciences Center, St. Joseph’s Healthcare Hamilton, University Health Network (Toronto), St. Michael’s Hospital (Toronto), The Ottawa Hospital and Kingston General Hospital. It was hypothesized that patients receiving care in an RRP located with a transplant center may have higher rates of progressing through the steps to kidney transplant. To further understand access to kidney transplant, in the maintenance dialysis cohort, we presented results by tertile of patient volume (ie, highest, middle, and lowest number of patients cared for by a RRP).
To aid in the interpretation of the results, we used the Kaplan-Meier product limit estimator to determine the 2-year cumulative probability of completing each step toward receiving a kidney transplant; a 2-year timeframe was selected to allow enough time for individuals to complete multiple steps in the kidney transplant process.
Results
Baseline characteristics
We included 8319 individuals in the approaching the need for dialysis cohort (Supplementary Figure 1) and 4869 individuals in the maintenance dialysis cohort (Supplementary Figure 2). During follow-up, 2870 (34.5%) individuals in the approaching the need for dialysis cohort had initiated maintenance dialysis, resulting in a total of 7739 patients receiving maintenance dialysis (Supplementary Figure 2). Table 1 provides the baseline characteristics for the approaching the need for dialysis cohort and the maintenance dialysis cohort. In the approaching the need for dialysis cohort, the median age was 62 years, 61.8% had diabetes, and 3.9% had a prior kidney transplant. In the maintenance dialysis cohort, the median age was 61 years, 54.8% had diabetes, 5.7% had a prior kidney transplant, and 70.5% were receiving in-center hemodialysis at cohort entry.
Baseline Characteristics for Individuals Approaching the Need for Dialysis and Individuals Receiving Maintenance Dialysis.

Baseline characteristics for the maintenance dialysis cohort are presented for individuals who qualified fore the maintenance dialysis at cohort entry.
Neighborhood-level income was used to construct income quintile. In total, <0.5% of individuals had missing data, and missing data were imputed into category 3.
In total, <0.5% of individuals had missing data, which were imputed into urban.
Most recent outpatient estimated glomerular filtration rate within 1 year of the cohort entry date.
Most recent outpatient estimated 2-year risk of kidney failure within 1 year of the cohort entry date. In total, 2.5% of individuals had missing data.
Greater comorbidity is indicated by a higher end-stage kidney disease-modified Charlson Comorbidity Index score.
Approaching the need for maintenance dialysis
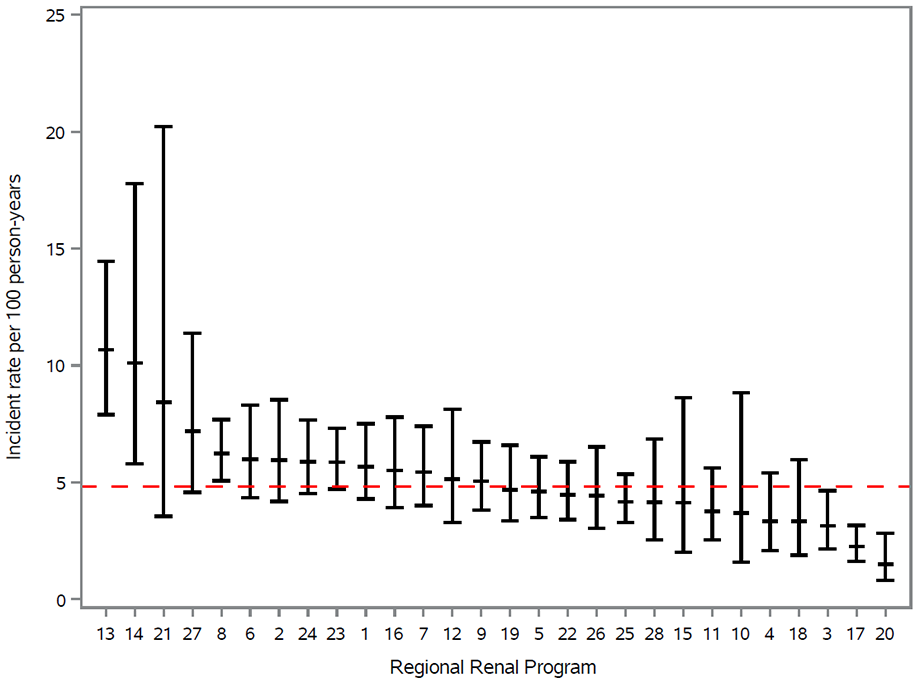
In individuals approaching the need for maintenance dialysis, we found there was substantial variability in the rate of a potential donor contacting a transplant center to be evaluated, varying more than 17-fold across RRPs from 0.67 (95% CI = 0.1, 4.8) to 11.7 (95% CI = 9.2, 14.9) (Figure 2). The proportion of individuals who had no living donor contact during the study period was 88.0% (Table 2).

Incidence rate of having a potential living donor contact a transplant center for an evaluation in patients approaching the need for dialysis (n = 8319) by regional renal program. Median follow-up 1.49 years (0.73, 2.42).
Summary of the Mean, Median, and Number of Potential Living Donors Contacting a Transplant Center for an Evaluation in the Approaching the Need for Dialysis and Maintenance Dialysis Cohorts.

Maintenance dialysis cohort
Depending on the step in the transplant process, the median follow-up varied from 1.38 years (0.55, 2.4) (transplant referral) to 2.21 years (1.28, 3.45) (living donor contact). For the outcome of kidney transplant referral, 2285 (38.4%) were referred, 1046 (17.6%) died, 813 (13.7%) developed a contraindication to transplant, 1787 (30%) reached the end of follow-up with no event, and 16 (0.3%) were no longer eligible for OHIP services.
In the maintenance dialysis cohort, we found substantial variability across the 28 RRPs in the average number of steps completed toward kidney transplant and in the rate of each step examined separately (Figures 3-7). For example, Figure 3 demonstrates the incidence rate of referral to a transplant center for evaluation in patients receiving maintenance dialysis by RRP, with the overall incidence rate in Ontario being 23.6 per 100 person-years (95% CI = 22.7, 24.6), and varying almost 8-fold across RRPs from 6.0 (95% CI = 4.2, 8.5) to 47.9 (95% CI = 42.6, 53.8). Figure 7 demonstrates the average number of steps completed toward receiving a kidney transplant, which varied from 11.7 (95% CI = 9.3, 14.8) to 44.0 (95% CI = 38.6, 50.1) steps per 100 patient-years across RRPs.
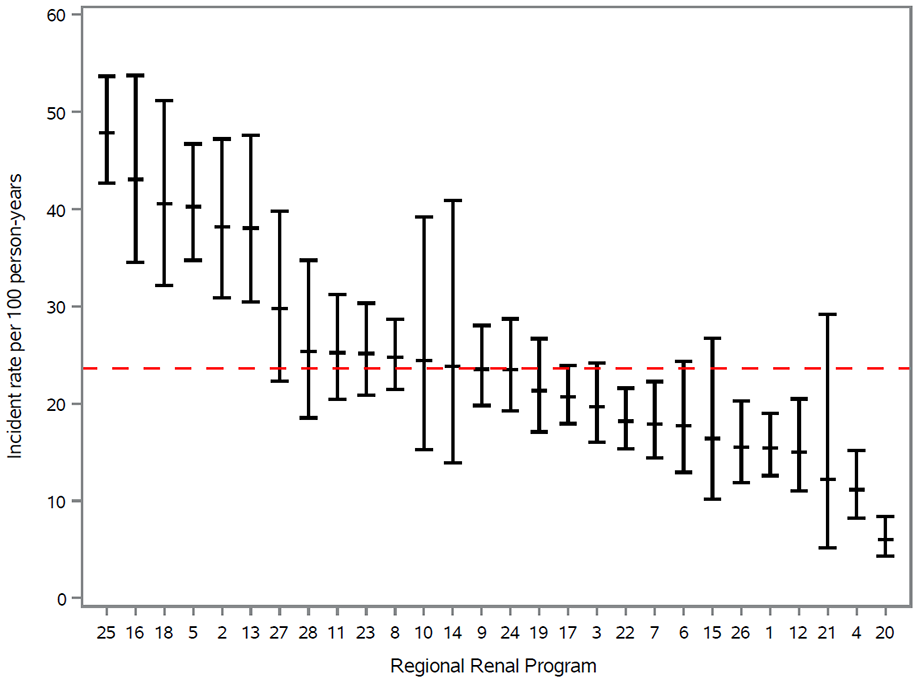
Incidence rate of referral to a transplant center for an evaluation in patients receiving maintenance dialysis (n= 5 947) by regional renal program. Median follow-up was 1.38 years (0.55, 2.4).
Incidence rate of having a potential living donor contact a transplant center for evaluation in patients receiving maintenance dialysis (n = 7739) by regional renal program. Median follow-up was 2.21 years (1.28, 3.45).

Incidence rate of being added to the deceased donor waitlist in patients receiving maintenance dialysis (n = 7505) by regional renal program. Median follow-up was 2.09 years (1.3, 3.2).
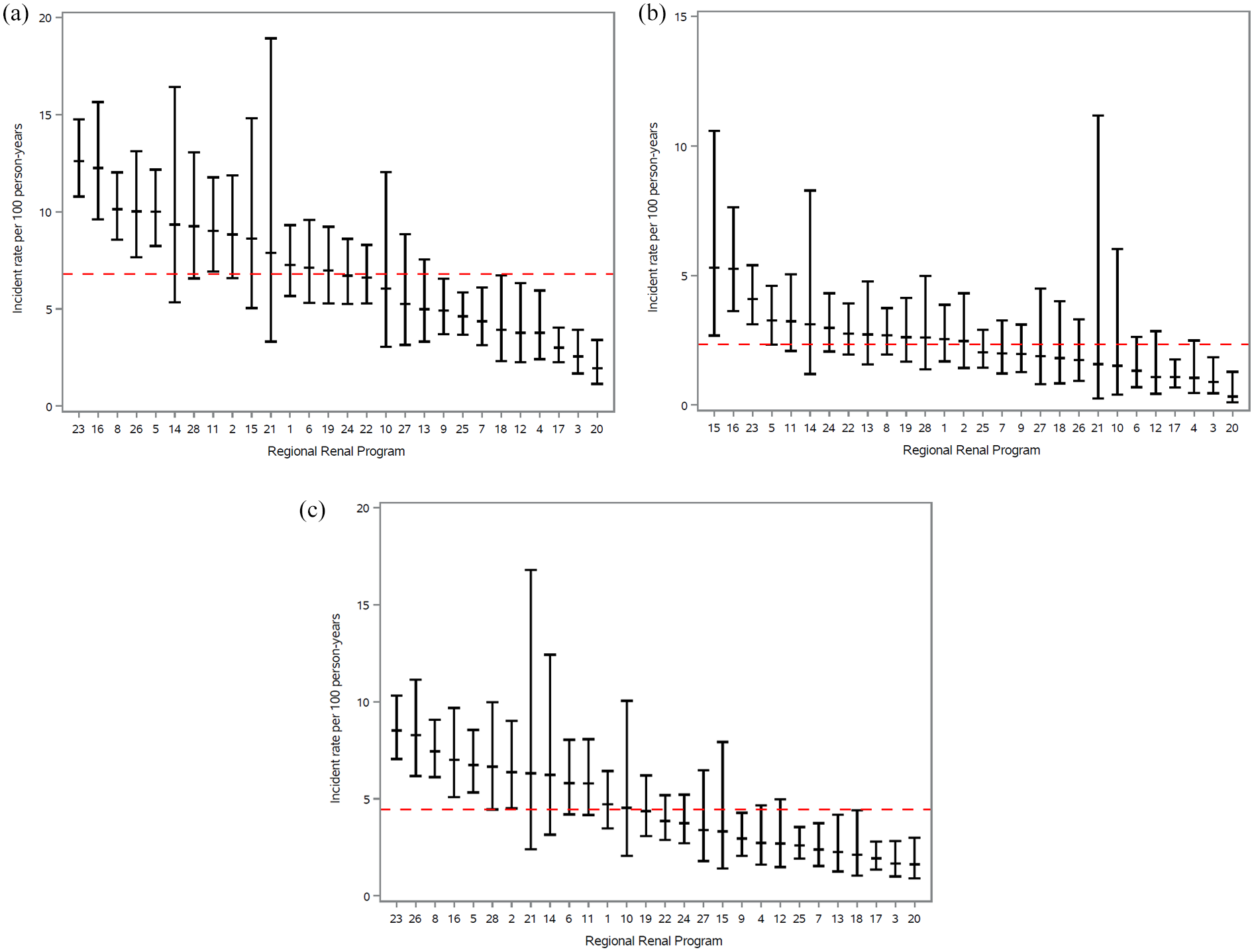
(a) Incidence rate of receiving a transplant from a living or deceased kidney donor in patients receiving maintenance dialysis (n = 7739) by regional renal program. Median follow-up was 2.21 years (1.38, 3.3).
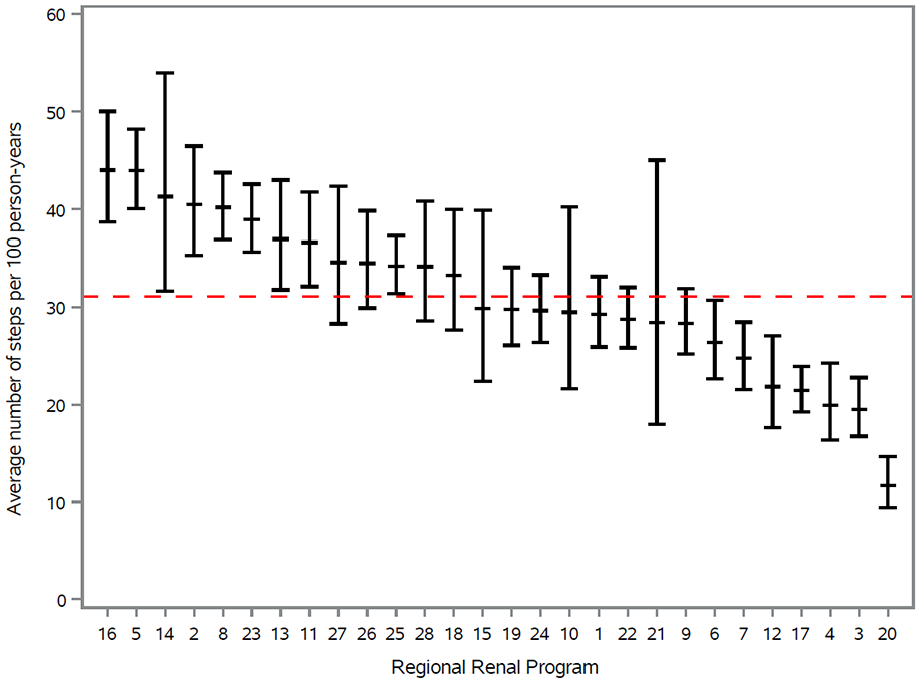
Rate of steps completed toward receiving a kidney transplant (per 100 person-years) in patients receiving maintenance dialysis presented by regional renal program. Each patient could complete up to 4 steps: step 1, referred to a transplant center for evaluation; step 2, had a potential living donor contact a transplant center for evaluation; step 3, deceased donor waitlist activation; and step 4, received a transplant from a living or deceased donor.
Table 3 demonstrates the key steps completed toward receiving a kidney transplant presented by the RRP with the highest incidence rate and the RRP with the lowest incidence rate. The average rate of each step varied widely, with non-overlapping confidence intervals for each step (Table 3). For example, the rate of a potential living donor contacting a transplant center to be evaluated varied from 1.5 (95% CI = 0.78, 2.9) to 10.7 (95% CI = 7.9, 14.5), deceased donor waitlist activation from 2.9 (95% CI = 1.9, 4.4) to 13.2 (95% CI = 11.0, 15.8), and kidney transplantation from 2.0 (95% CI = 1.1, 3.4) to 12.6 (95% CI = 10.8, 14.8). The proportion of individuals who had no potential donor contacting a transplant center for an evaluation during the study period was 88.6% (Table 2).
Key Steps Completed toward Receiving a Kidney Transplant for the Maintenance Dialysis Cohort Presented by the Province of Ontario, the Regional Renal Program (RRP) with the Highest Incidence Rate, and the Regional Renal Program with the Lowest Incidence Rate. a
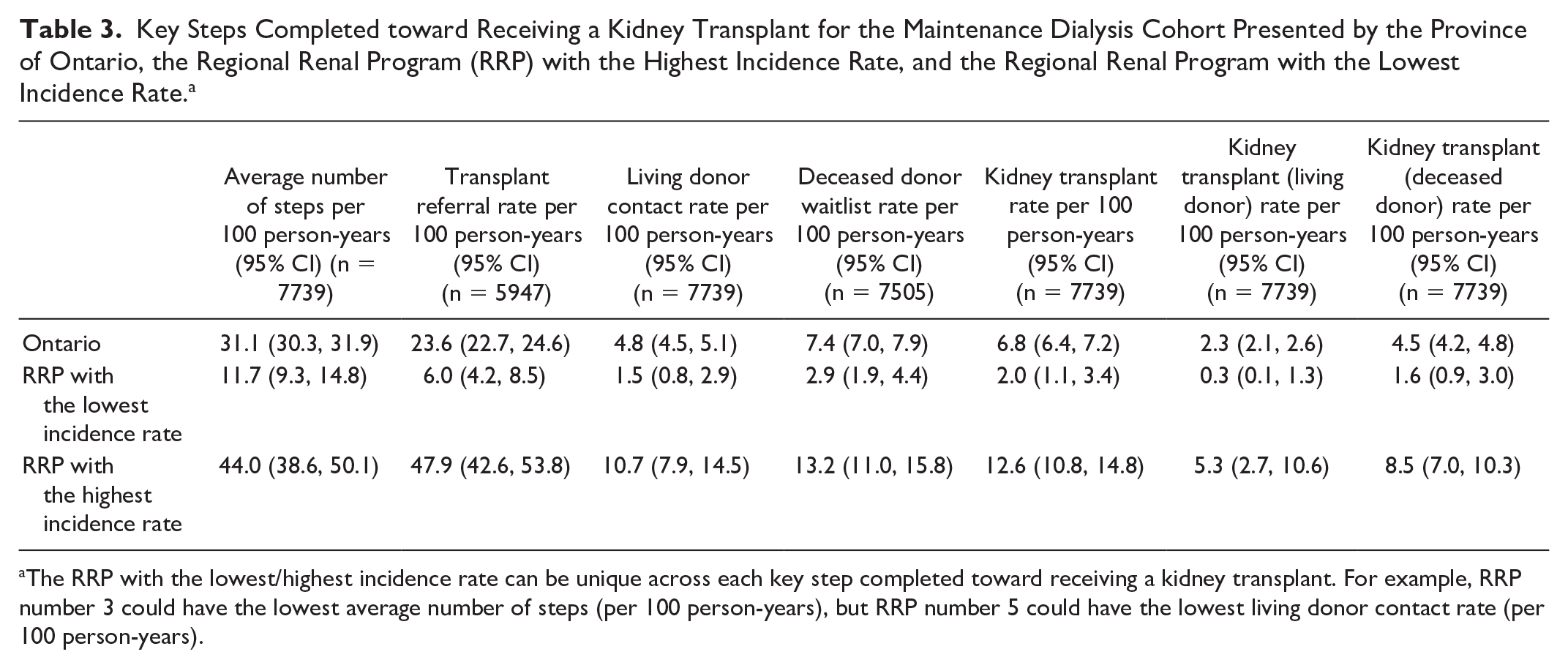
The RRP with the lowest/highest incidence rate can be unique across each key step completed toward receiving a kidney transplant. For example, RRP number 3 could have the lowest average number of steps (per 100 person-years), but RRP number 5 could have the lowest living donor contact rate (per 100 person-years).
When examining RRPs’ access to kidney transplants by the step in the kidney transplant process, we found several RRPs simultaneously had one of the higher incidence rates for 1 step but one of the lower incidence rates for another step. For example, some RRPs would have one of the highest incidence rates of kidney transplant referral but then would have one of the lowest rates of a living donor contacting a transplant center to be evaluated.
When examining the results by 5 Ontario geographic regions, RRPs located in Northern Ontario consistently ranked as the lowest-performing geographic region in all steps in the transplant process (Table 4). For example, the rate of transplant referral varied almost 3-fold from 10.0 (95% CI = 8.3, 12.0) in Northern Ontario to 28.7 (95% CI = 25.7, 32.1) in Toronto. The Toronto and Western Ontario regions generally had the highest rates of steps completed toward receiving a kidney transplant.
Key Steps Completed toward Receiving a Kidney Transplant in Patients Receiving Maintenance Dialysis Presented by 5 Ontario Geographic Regions.
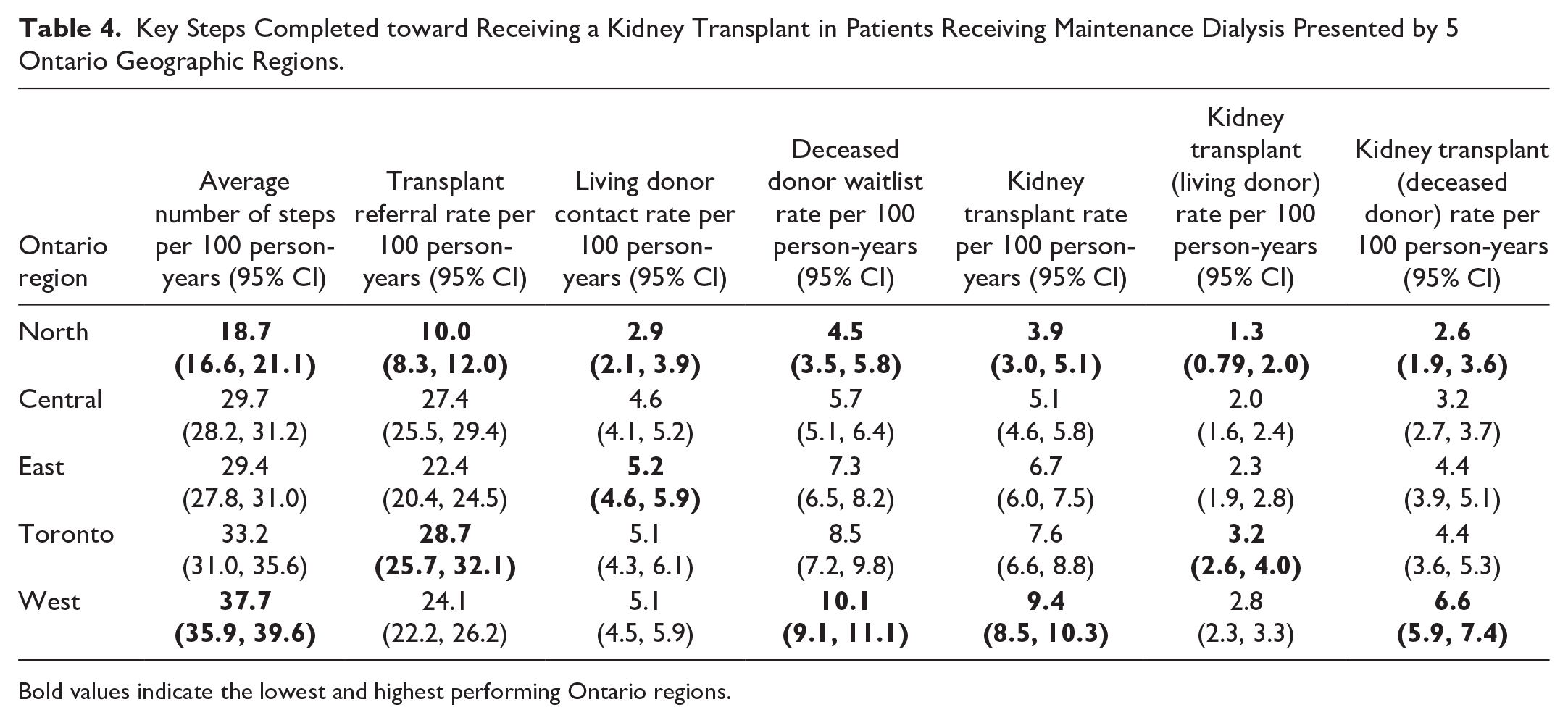
Bold values indicate the lowest and highest performing Ontario regions.
Time to complete key steps in the kidney transplant process
When we examined the time to complete key steps in the transplant process, there was substantial variability across RRPs (Tables 5). For example, the time from entering the approaching the need for dialysis cohort to a potential living donor contacting a transplant center to be evaluated varied from a median of 159 days (48, 438) to 830 days (692, 922). The time from entering the approaching the need for dialysis cohort to referral to a transplant center (restricting to patients who had a living donor contact) varied across RRPs from a median of 125 days (70, 385) to 701 days (503, 874). Similarly, the time from starting maintenance dialysis to referral to a transplant center for an evaluation varied widely across RRPs from a median of 104 days (56, 178) to 508 days (185, 749).
Time to Complete Key Steps in the Kidney Transplant Process, Presented by the Median Number of Days in Ontario, Median Number of Days for the RRP with the Shortest Time, and Median Number of Days for the RRP with the Longest Time.

Assessed in patients approaching the need for dialysis who received their referral to a transplant center and who had a potential living kidney donor begin their evaluation during the study period.
Assessed in patients who had at least 1 potential living kidney donor begin their evaluation during the study period (restricted to the first contact).
Assessed in patients receiving maintenance dialysis who received a transplant referral after starting maintenance dialysis during the study period.
Assessed in patients receiving maintenance dialysis who were added to the deceased donor waitlist during the study period.
Assessed in patients receiving maintenance dialysis who were referred to a transplant center for an evaluation and who were added to the deceased donor waitlist during the study period.
Assessed in patients approaching the need for dialysis and in patients receiving maintenance dialysis who were referred to a transplant center for an evaluation and received a living or deceased donor kidney transplant during the study period. Presented by all kidney transplants and by living vs deceased donor kidney transplants separately.
Assessed in patients approaching the need for dialysis and in patients receiving maintenance dialysis who had a potential living donor contact a transplant center for evaluation and received a living or deceased donor kidney transplant during the study period.
Note. Several timing indicators for steps in the kidney transplant process had RRPs with <6 patients contributing to the follow-up time.
Additional Analysis
In the maintenance dialysis population, we found the rate of each step completed toward kidney transplant was substantially higher in RRPs located with a transplant center compared to RRPs not located with a transplant center (Supplementary Table S4). For example, when examining the rate of referrals (per 100 person-years), RRPs located with a transplant center had a rate of 26.2 referrals (95% CI = 24.2, 28.3) vs 22.8 (95% CI = 21.7, 23.9) for RRPs not located with a transplant center. Similarly, the average number of steps (per 100 person-years) completed toward receiving a kidney transplant was higher in RRPs located with a transplant center vs those who were not (36.1 vs 28.9).
When we analyzed steps toward receiving a kidney transplant by RRP patient volume, we found that RRPs with a middle volume of patients often had the lowest rate of access to kidney transplant, including for the average number of steps toward kidney transplant, transplant referral rate, and living donor contact rate, while RRPs with the highest volume of patients had the highest rates of deceased donor waitlisting and kidney transplantation (including living and deceased) (Supplementary Table 5). However, confidence intervals often overlapped.
The 2-year cumulative probability of completing each step toward receiving a kidney transplant is presented in Supplementary Figures S3 to S7. In the maintenance dialysis population, the 2-year cumulative probability of referral to a transplant center for an evaluation ranged from 11.4% (95% CI = 7.6, 16.8) to 63.1% (95% CI = 58.2, 68.0), living donor contacts from 3.6% (95% CI = 1.8, 7.2) to 22.4% (95% CI = 13.2, 36.5), deceased donor waitlist activation from 4.4% (95% CI = 2.5, 7.9) to 28.1% (95% CI = 17.0, 44.2), and kidney transplant from 1.1% (95% CI = 0.3, 4.6) to 20.4% (95% CI = 11.4, 35.2).
Discussion
In this study, we found a substantial variation in the rate of key steps required for kidney transplant across RRPs in patients with kidney failure who had no contraindications to kidney transplant. We found that patients residing in Northern Ontario consistently had the lowest rates of steps completed toward receiving a kidney transplant. Our results suggest that despite universal access to health care and recent province-wide initiatives to improve access to transplants, substantial disparities in access to kidney transplant remain in Ontario.
Similar to previous studies conducted in both public and private health care systems, we found substantial variation in access to kidney transplant depending on where a patient received their kidney care.9-17 There are several potential explanations. Despite a provincial priority to improve access to kidney transplant, variability may exist across RRPs in the amount of transplant education provided, provider transplant knowledge, and staff-to-patient ratio. Previous work has demonstrated that the aforementioned factors can impact transplant rates.9,28-30 Although we attempted to restrict our denominator to individuals who were transplant eligible, there are still unmeasured facility- and patient-level factors that could influence variability. For example, we were not able to measure patient preference to receive a kidney transplant.
Of the 4 key steps in the kidney transplant process, kidney transplant referral and living donor contacts are under the direct control of the RRPs. Our results provide RRPs with information on which step in the kidney transplant process needs the most improvement. For example, a RRP could be doing well at referring their patients for a kidney transplant but need to improve helping patients find living kidney donors. This work highlights the need to understand the reasons for variability in access to kidney transplant across RRPs. Focus groups, interviews, and surveys are a good starting point to understand barriers to accessing kidney transplantation. One potential barrier may be that nephrologist and RRP remuneration in Ontario for transplant-related activity is lower than that for dialysis-related activities. Modifying financial incentives for nephrologists to manage kidney transplant recipients and providing incentives to RPPs for getting their patients transplanted may improve access to kidney transplants. Once barriers are identified, patients and providers can co-design solutions to target them. These results also highlight the importance of continued measurement and regular reporting by RRPs of key steps in the transplant process to drive system improvement. Given variability in access to transplant has been found in both public and private health care settings,9-17 jurisdictions beyond Ontario would benefit from continued measurement and reporting and the development of associated quality improvement initiatives.
A kidney transplant from a living donor offers advantages over a deceased donor, including improved graft and patient survival.31,32 The favorable treatment option for patients with kidney failure is a pre-emptive kidney transplant (ie, no maintenance dialysis prior to transplant) from a living donor. 33 Timely identification of a living donor is key to enabling pre-emptive living kidney donor transplantation; however, in the approaching the need for dialysis cohort, we found that the median time from entering the cohort to a potential living donor contacting the transplant center was 243 days, with a range of 159 to 830 days across RRPs. In both the approaching the need for dialysis and maintenance dialysis cohorts, we found that 88% of individuals had no potential living donor contact the transplant center for an evaluation. Approximately 6% to 7% of individuals had a single potential living donor contact the center to be evaluated. This is concerning, as often multiple potential donors must be evaluated before finding a suitable donor eligible to donate to the intended recipient. 34 Furthermore, once a living donor contacts a transplant center for an evaluation, it takes the patient a median of 433 days for their intended recipient to receive a kidney transplant. This suggests there may be inefficiencies in the recipient and/or living donor workup process that warrant improvement.
Our results highlight an opportunity to improve kidney transplant rates in Northern Ontario, since these patients consistently completed fewer steps toward receiving a kidney transplant. Patients in the North may face several unique barriers to accessing transplants, such as long travel distances to the nearest transplant center, accommodation costs, and less access to the tests and consultations required to complete the transplant evaluation. There is also a large Indigenous population in Northern Ontario, who may face additional barriers including a lack of language interpreters, 35 inadequate educational resources, and mistrust in the health care system due to their colonial history.36,37
We found the rate of each step completed toward receiving a kidney transplant was substantially higher in RRPs located with a transplant center. Previous work in the United States has demonstrated significantly higher rates of transplant when there were more transplant centers per 10 000 patients with kidney failure. 9 Future work should explore the potential benefits of having a kidney transplant center located within a given geographic region.
The strengths of our study include restricting our cohort to individuals with no recorded contraindications to kidney transplants, making patients more similar across RRPs, and providing a comprehensive examination of access to kidney transplants by evaluating four distinct steps in the process toward receiving a kidney transplant.
Despite these strengths, there are limitations worth noting. First, several RRPs had a small number of patients, resulting in wide confidence intervals. Similarly, due to the small number of patients at some RRPs, the median time to complete key transplant steps was often based on a small number of events. Second, while our definition of no recorded contraindications to kidney transplant has been found to be accurate, 23 administrative databases cannot capture all the complexities of transplant eligibility. Third, our results may not be generalizable to kidney failure populations outside of Ontario. Fourth, we did not examine the reason for the differences in access to kidney transplant across RRPs. Unmeasured differences in patient characteristics across RRPs could have contributed to some of the observed variation (eg, differences in the proportion of patients who smoke). Future qualitative work should focus on understanding barriers and enablers to kidney transplantation across RRPs.
Conclusions
Our study demonstrates variability in the rate of steps completed toward receiving a kidney transplant across RRPs in Ontario, Canada. The RRPs and provincial kidney and transplant agencies need to continue to work to understand barriers to kidney transplant access and co-design potential solutions to target these barriers so that more patients with kidney failure can benefit from this life-saving treatment.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251346048 – Supplemental material for Variation in Kidney Transplant Referral, Living Donor Contacts, Waitlisting, and Kidney Transplant Across Regional Renal Programs in Ontario, Canada: A Population-Based Cohort Study
Supplemental material, sj-docx-1-cjk-10.1177_20543581251346048 for Variation in Kidney Transplant Referral, Living Donor Contacts, Waitlisting, and Kidney Transplant Across Regional Renal Programs in Ontario, Canada: A Population-Based Cohort Study by Kyla L. Naylor, Seychelle Yohanna, Graham Smith, Amit X. Garg, Lori Elliott, Gregory Knoll, S. Joseph Kim and Matthew Weir in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors thank the Executive Committee of Can-SOLVE CKD (Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease), a patient-oriented research network to transform the care of people affected by kidney disease (![]() ). K.L.N. is supported by a Health System Impact Embedded Early Career Researcher Award Canadian Institutes of Health Research. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). The study was completed at the ICES Western site, where core funding is provided by the Academic Medical Organization of Southwestern Ontario, the Schulich School of Medicine and Dentistry, Western University, and the Lawson Health Research Institute. The research was conducted by members of the ICES Kidney, Dialysis, and Transplantation team at the ICES Western facility. The authors acknowledge that the data used in this publication were obtained through the Ontario Renal Reporting System, collected and provided by Ontario Health and Ontario Renal Network. Parts of this material are based on data and information provided by Ontario Health (OH). This report was conducted with the support of Ontario Health (Ontario Renal Network) through funding provided by the Ontario Ministry of Health. The opinions, results, views, and conclusions reported in this paper are those of the authors and do not necessarily reflect those of OH. No endorsement by OH (Ontario Renal Network) is intended or should be inferred. This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from Canada Post Corporation and Statistics Canada. The authors acknowledge that the data used in this study were provided by the Trillium Gift of Life Network (Ontario Health), 2022, Toronto, Ontario. The researcher’s interpretations and statements in this publication are those of the researcher only and not those of Trillium Gift of Life Network (Ontario Health). Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information and the Ontario Ministry of Health. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
). K.L.N. is supported by a Health System Impact Embedded Early Career Researcher Award Canadian Institutes of Health Research. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). The study was completed at the ICES Western site, where core funding is provided by the Academic Medical Organization of Southwestern Ontario, the Schulich School of Medicine and Dentistry, Western University, and the Lawson Health Research Institute. The research was conducted by members of the ICES Kidney, Dialysis, and Transplantation team at the ICES Western facility. The authors acknowledge that the data used in this publication were obtained through the Ontario Renal Reporting System, collected and provided by Ontario Health and Ontario Renal Network. Parts of this material are based on data and information provided by Ontario Health (OH). This report was conducted with the support of Ontario Health (Ontario Renal Network) through funding provided by the Ontario Ministry of Health. The opinions, results, views, and conclusions reported in this paper are those of the authors and do not necessarily reflect those of OH. No endorsement by OH (Ontario Renal Network) is intended or should be inferred. This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from Canada Post Corporation and Statistics Canada. The authors acknowledge that the data used in this study were provided by the Trillium Gift of Life Network (Ontario Health), 2022, Toronto, Ontario. The researcher’s interpretations and statements in this publication are those of the researcher only and not those of Trillium Gift of Life Network (Ontario Health). Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information and the Ontario Ministry of Health. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from Ontario Health (Ontario Renal Network). The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding source; no endorsement is intended or should be inferred.
Ethics Approval and Consent to Participate
The ICES is an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board.
Consent for Publication
Consent for publication was obtained from all authors.
Availability of Data and Materials
The data set from this study is held securely in coded form at ICES. While legal data-sharing agreements between ICES and data providers (eg, health care organizations and government) prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at ![]() (email:
(email:
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.