
Abstract
Background:
Organ and tissue donation and transplantation (OTDT) policies and practices lead to differential care for sexual and gender minorities (SGMs). The experiences of SGM patients and caregivers in the transplantation system have not been published. The perspectives of SGMs on how to best address existing inequities are not understood.
Objective:
To characterize the lived experiences of SGM patients and caregivers in solid-organ transplant health systems, as well as the perspectives and priorities of these individuals regarding SGM-relevant policies, practices and targets for system improvements.
Methods:
We conducted a series (N = 12) of one-on-one semi-structured interviews with a convenience sample of SGMs with lived experience of the OTDT system. We transcribed interviews verbatim and performed a formal qualitative analysis combining a best-fit framework synthesis and inductive thematic analysis.
Results:
We revealed novel targets for action to improve inclusive care in the transplantation system directly informed by the lived experiences of SGM patients and caregivers. Targets for improvement included (1) enhancements to shared decision-making between OTDT providers and patients, (2) transparent communication from OTDT organizations, (3) data-driven donor risk assessments, (4) expanded healthcare worker training, (5) inclusive physical care spaces, (6) recommendations for transgender and gender-diverse health system planning, (7) integrated sexual and reproductive healthcare services for transplant recipients, (8) increased SGM representation in medical education and care settings, (9) SGM and OTDT intersectional support networks, and (10) structural facilitation of SGM community advocacy efforts.
Limitations:
While thematic saturation was achieved with our sample, we recognize that not all SGM identities were represented. It remains likely that additional experiences, beliefs, and priorities exist in the SGM community.
Conclusions:
The emergent priorities and perspectives of SGMs with lived experience of transplant systems should inform patient-centered equitable health system advancements.
Background
Sexual and gender minority (SGM) populations face differential policies and practices in organ and tissue donation and transplantation (OTDT) systems compared to heterosexual and cisgender populations. 1 SGMs, including Two-Spirit, Lesbian, Gay, Bisexual, Transgender, Queer, Questioning, Intersex and more identities (2SLGBTQI+) make up at least 10% of the global population with increasing proportions of people self-identifying as 2SLGBTQI+ in younger generations. 2 SGMs receive a lower quality of healthcare with poorer outcomes than the general population. 3 We have previously described OTDT system inequities, harms, and knowledge gaps relevant to SGMs. 4 OTDT systems do not routinely collect relevant socioeconomic data to routinely quantify or monitor SGM-specific inequities. 5 This leads to under-representation of SGM identities in observational research and health system planning. 6 A lack of precision regarding self-identified gender vs. sex assigned at birth and under-representation in research make transgender and gender-diverse (TGD) patients particularly vulnerable to variable practice. 6 Heterogenous regulations regarding SGM patients in OTDT systems between the United States and Canada expose an opportunity to update and standardize SGM-relevant policies and practices using contemporary evidence. 7 We performed in-depth semi-structured interviews with members of an SGM OTDT research advisory team composed of SGM organ donors, transplant recipients and the caregivers of deceased organ donors. In this manuscript we describe SGM patient and caregiver experiences, perspectives and recommendations to improve the care of SGM patients in transplantation health systems. The experiences of SGMs in the organ and tissue donation (OTD) system are described separately.
Methods
Qualitative Methodology
We used best-fit framework synthesis and paired inductive thematic analysis methods to analyze interview transcripts.
Participants, Recruitment, Sample Size, and Thematic Saturation
We recruited 12 participants representing living and registered donors, caregivers of deceased donors and transplant recipients from a pre-existing SGM OTDT research advisory team (Table 1). We performed semi-structured interviews with each. The University of Manitoba Research Ethics Board provided approval for this study (HS26020(H2023:172)).
Participant Characteristics.
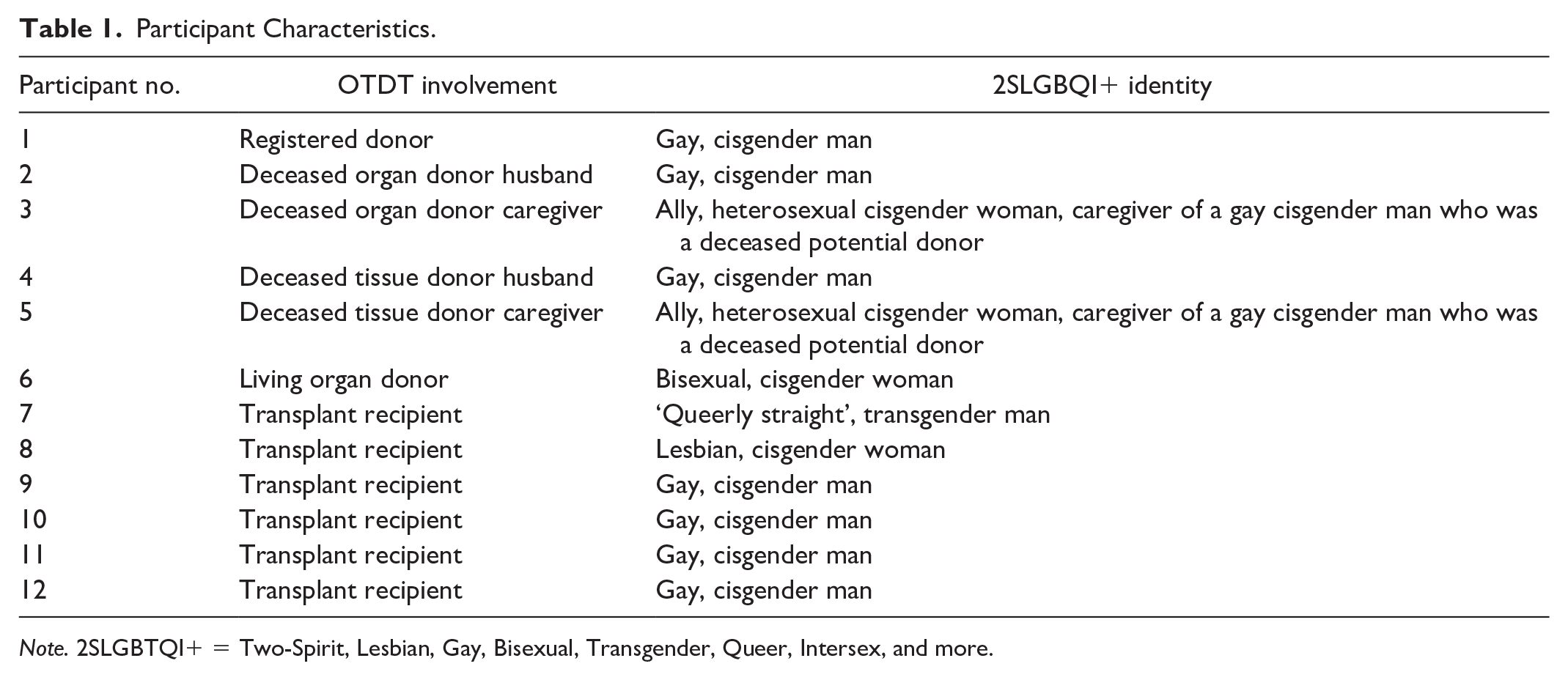
Note. 2SLGBTQI+ = Two-Spirit, Lesbian, Gay, Bisexual, Transgender, Queer, Intersex, and more.
We interviewed 12 out of 13 members of our advisory team as a convenience sample, with 1 member not being able to participate due to competing demands on their time. Thematic saturation was determined according to the Guest method which compares the proportion of new themes emerging from each interview to the total number of themes already identified. 8 We did not pair participant identifiers with individual quotations to minimize the risk of participant identification.
Procedure, Interview Guide Development, and Interview Schedule
We conducted one 60- to 90-min interview with each participant using a web-conferencing platform from July to August, 2023. Informed consent, including review of the interview guide, was obtained prior to each interview. Interviews were recorded verbatim and transcribed for analysis. Participants were remunerated at $50/h.
We took a semi-structured approach to our interviews with question domains informed by a scoping review of the extant literature on SGM identities in OTDT 1 and input from advisory team partners and co-authors. Collaborators further defined specific questions and potential prompts. Interview domains included (1) benefits of SGM identities, (2) harms, (3) inequities, and (4) beliefs and opinions regarding specific policies, recommendations or identified gaps in care, and (5) descriptions of individual experiences within the OTDT system (Online Supplemental Appendix 1).
A single researcher (M.L.) with a pre-existing relationship with participants (through the advisory team) conducted each interview. This interviewer had detailed knowledge of the subject matter focus of the interviews which facilitated maximum extraction of useful information from participants.
Data Analysis
Demographic data are summarized as counts. 8 Transcripts were analyzed using Atlas.ti (version 22.1.0). We first charted findings using a best-fit framework synthesis structured according to interview domains (Online Supplemental Appendix 1). Interview domains were the initial structure onto which we applied charted findings. The selected domains were based on a scoping review on sexual orientation and gender identity in OTDT. 1 This method has been described as transparent and pragmatic, 9 facilitating the coding of initial data against an a priori defined framework. We paired an additional inductive thematic analysis to identify additional themes and concepts. We conducted our thematic analysis in a phased approach: becoming familiar with the data, generating initial codes, searching for themes, reviewing themes, defining, and naming themes and producing the report. 10 We created a codebook to ensure reliability of coding. Two researchers (M.L. and C.H.) independently coded transcripts in duplicate. The generation of codes was iterative moving from open coding where codes are generated from the text, then through review and discussion codes were grouped and refined to identify themes that captured the essence of the primary data. Agreement on final codes was achieved by consensus.
Positionality and Reflexivity
We are a diverse team of SGM and ally investigators, caregivers, and patient partners. In collaborating on this work, we shared an a priori intention to support health equity for SGM populations. We approached this project with the shared knowledge that harms and inequities exist for SGMs in OTDT 1 and we defined our intention to further explore the experiences of SGM patients and caregivers from their own perspectives. We anticipated that novel themes and experiences not previously published may exist. We felt the unique familiarity with OTDT system issues developed among our patient and caregiver advisory team was a strength of our approach and necessary to explore their perspectives regarding health system policies and practices that are not transparently communicated or commonly known to patients. 1 We anticipated deriving more meaning from interviews with these patients and caregivers who had reflected on how current policies and practices had impacted them, compared to those who may have experienced differential treatment but been unaware.
Results
Participants
Twelve people including caregivers of deceased organ donors (n = 3), registered and living organ donors (n = 2) and transplant recipients (n = 6) each completed a semi-structured interview lasting 60 to 90 minutes. Most participants self-identified as cisgender (n = 11) and gay (n = 7). Participant characteristics are summarized in Table 1.
Thematic Analysis
Seven themes and related sub-themes emerged from the interview transcripts (Table 2), for the analysis focused on SGMs in transplant systems.
Emergent Themes and Sub-Themes.
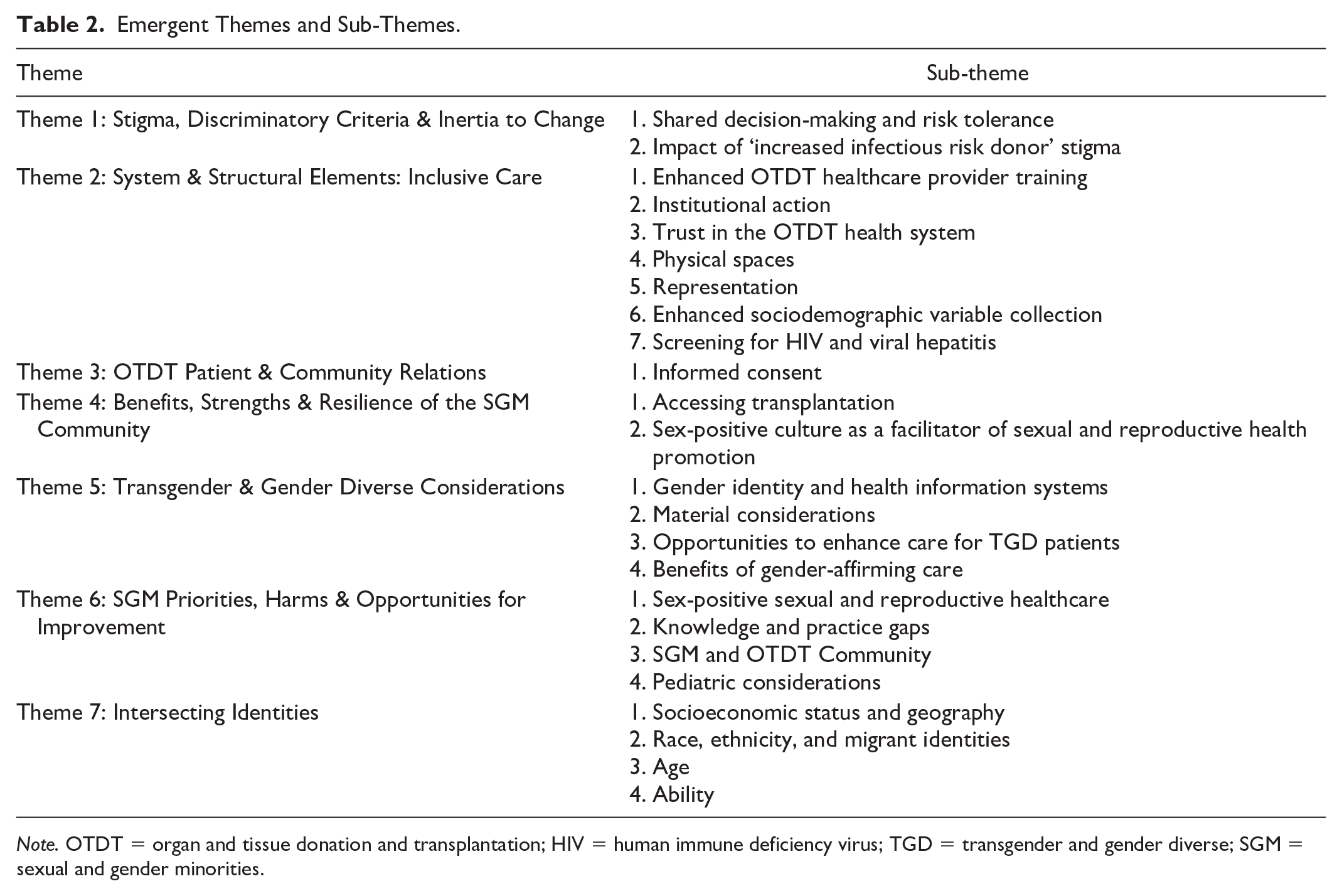
Note. OTDT = organ and tissue donation and transplantation; HIV = human immune deficiency virus; TGD = transgender and gender diverse; SGM = sexual and gender minorities.
Theme 1—Stigma, Discriminatory Criteria, and Inertia to Change
Shared decision-making and risk tolerance
Current shared decision-making processes between transplant programs and transplant candidates were a target for improvement, specifically, enhanced understanding about the benefits and risks of accepting an increased infectious risk donor (IIRD) organ vs. a baseline risk organ. SGM transplant recipients expressed a favorable benefit-to-risk ratio in accepting organs from SGM donors, “because right now my trajectory is death. So I’d rather live. And, those just don’t seem like substantial risks . . .” (Table 3, Quotes 3.3.1.1-3.3.1.2).
Theme 1—Stigma, Discriminatory Criteria, and Inertia to Change.
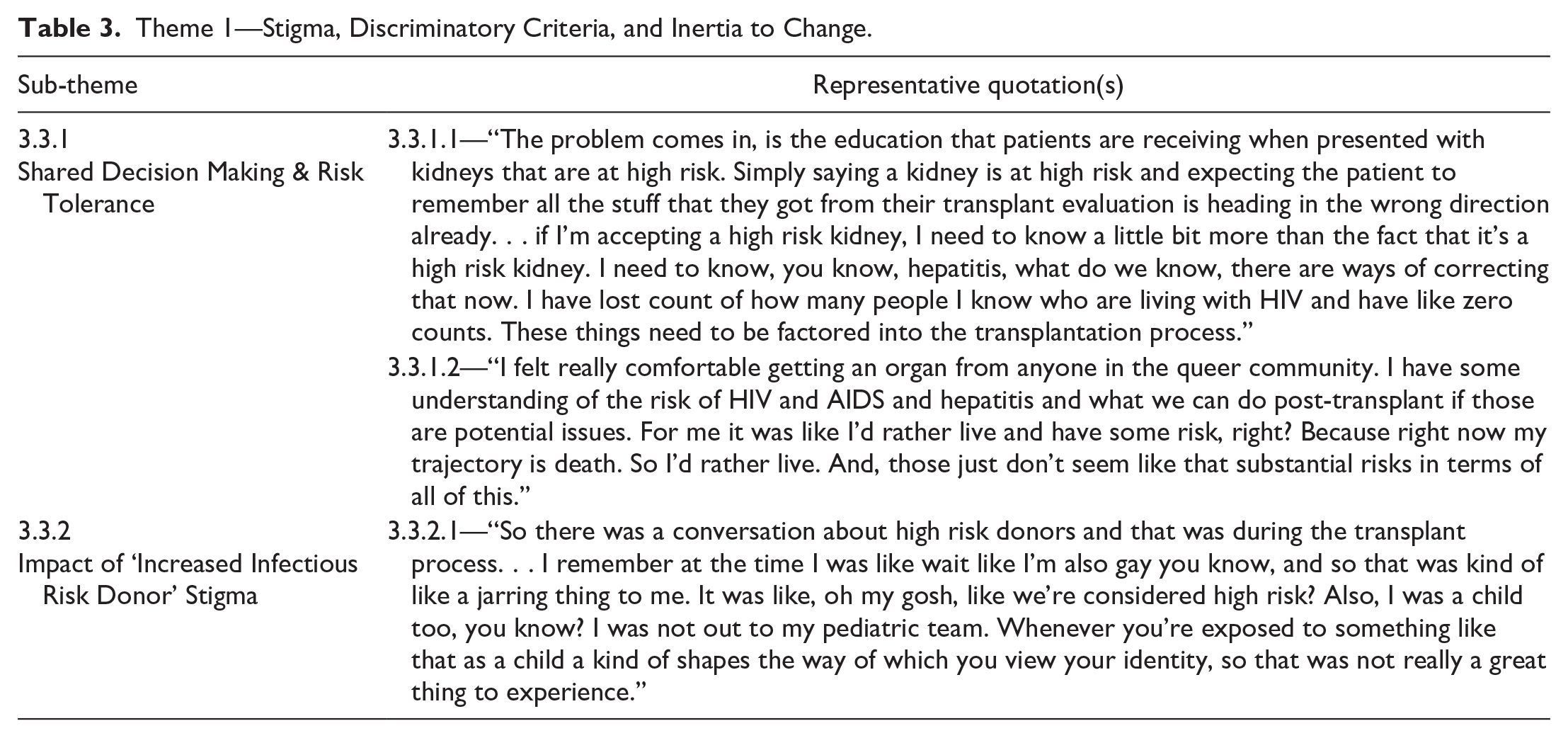
Impact of “increased infectious risk donor” stigma
Impacts of IIRD paradigms on SGM transplant recipients included shame for having their identities equated with disease transmission, uncertainty of the accuracy of donor risk assessments in TGD patients, and opportunities to enhance communication around the relevant risks and benefits of accepting an IIRD-labeled organ. Deficit-focused framing of SGM donors as being at increased risk of infections was particularly impactful to pediatric recipients with evolving sexual orientations (Table 3, Quote 3.3.2.1).
Theme 2—System and Structural Elements: Inclusive Care
Enhanced OTDT healthcare provider training
Participants desired enhanced SGM expertise and cultural humility skills in their healthcare providers (Online Supplemental Appendix 2, Table 2, Quotes 3.4.1-3.4.1.4). “I think anybody who has contact with the patient . . . transport people getting you to a test, the x-ray technician, the phlebotomist . . . not just the nurses and the doctors. Everybody who’s in contact with the patient should be trained.” They wanted healthcare providers to mirror the language they used to describe themselves and their relationships, but not to make assumptions about their identities (Online Supplemental Appendix 2, Table 2, Quotes 3.4.1.5-3.4.1.6). Participants recommended framing the expansion of these skills as an opportunity to celebrate diverse patients’ identities. Participants cautioned against anchoring biases like the “trans broken arm” syndrome (Table 4, Quote 3.4.1.8).
Theme 2—System and Structural Elements: Testing and Inclusive Care.
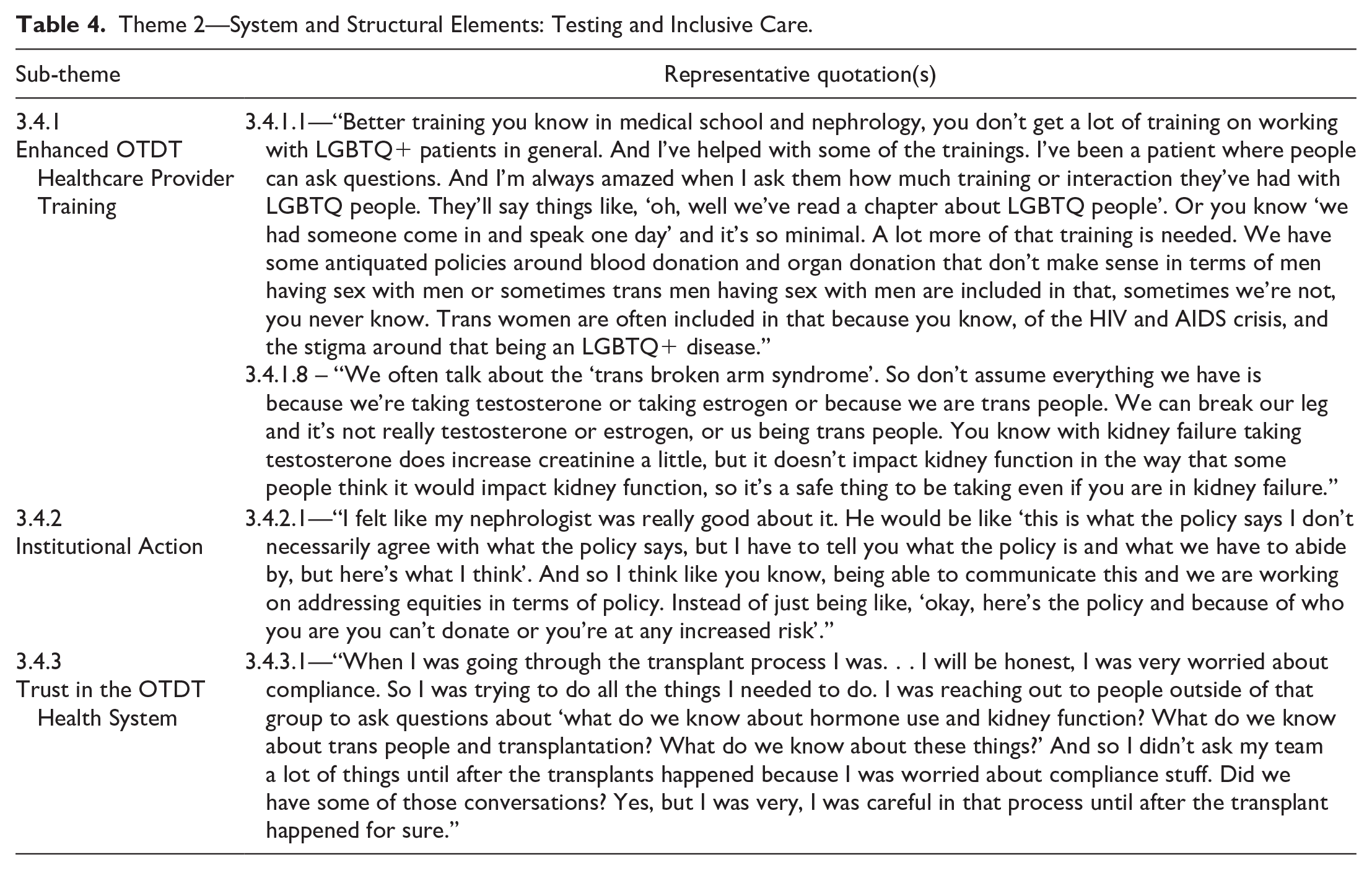
Institutional action
Participants felt institutions should support equitable care through transparent communication, acknowledgment of existing gaps, and recognition of successful equity initiatives (Table 4, Quote 3.4.2.1). Institutions could further support equitable care through creation and enforcement of non-discrimination policies, standardization of SGM-relevant OTDT policies and practices, and offering SGM-specific advocacy services. Novel descriptions of the need for intersectional support networks that included SGM identities along with lived experience of the OTDT system emerged (Online Supplemental Appendix 2, Table 2, Quotes 3.4.2.2-3.4.2.9).
Trust in the OTDT health system
SGM transplant recipients reported a particular need to appear “compliant” to access transplantation, at times hiding their own concerns or even identities (Table 4, Quote 3.4.3.1). Age and ethnicity further interacted in patient perceptions of needing to compromise their priorities to maintain a compliant reputation (Online Supplemental Appendix 2, Table 2, Quote 3.4.3.2). Some patients felt their very bodily autonomy was at stake, “as a transplant patient, you can feel that pressure even more because you are being evaluated based on being compliant. So if you are not compliant in something because you don’t want it to be done to your body. . . you constantly feel afraid.”
Physical spaces, representation, sociodemographic variable collection and screening for HIV and viral hepatitis
Additional sub-themes and representative quotations are presented in Online Supplemental Appendix 3.
Theme 3—OTDT Patient and Community Relations
Informed consent
Opportunities to strengthen informed consent processes in OTDT were identified for transplant recipients, living donors and deceased donors. Transplant recipients related incomplete understanding of issues such as the risks and benefits of accepting IIRD organs, and pressure to consent to whatever was asked to ensure access to transplantation from health system gatekeepers. Living donors identified a lack of preparation for the realization that the recipient of their donation would be notified if any IIRD factors were identified. Voluntary disclosure of sensitive information by donors was conditional on what was specifically asked of them (Online Supplemental Appendix 2, Table 3, Quotes 3.5.1.1-3.5.1.4).
Theme 4—Benefits, Strengths, and Resilience of the SGM Community
Accessing transplantation
SGM communities were framed as specific networks that transplant candidates could turn to in search of a living organ donor (Table 5, Quotes 3.6.1.1-3.6.1.4). Activism and self-advocacy were described as foundational components of SGM communities’ identities, developed through surviving shared cultural events like the HIV/AIDS epidemic. These strengths translated into advocacy in supporting transplant candidates through their OTDT journey (Online Supplemental Appendix 2, Table 4, Quotes 3.6.1.5-3.6.1.6).
Theme 4—Benefits, Strengths, and Resilience of the SGM Community.

Sex-positive culture as a facilitator of sexual and reproductive health promotion
A sex-positive culture in the SGM community was noted to be a strength, particularly in supporting prevention, detection, and treatment of sexually transmitted infections (Online Supplemental Appendix 2, Table 4, Quote 3.6.2.1).
Theme 5—TGD Considerations
Gender identity and health information systems
Universal asking about pronouns and gender identity was an example of an affirming practice (Table 6). Most transplant recipients said they had never been asked to confirm their gender identities. “No! Out of the 2 transplants that I’ve had, it’s never been a discussion.” Describing the options for sex assigned at birth vs. gender identity when registering to be a deceased organ donor, one interviewee noted the binary options available “Absolutely, M or F. Just one or the other.” Another participant noted positive changes at their current transplant center where confirmation of pronouns and gender identity have become a routine part of the clinical encounter (Online Supplemental Appendix 2, Table 5, Quotes 3.7.1.1-3.7.1.4).
Theme 5—Transgender and Gender-Diverse Considerations.
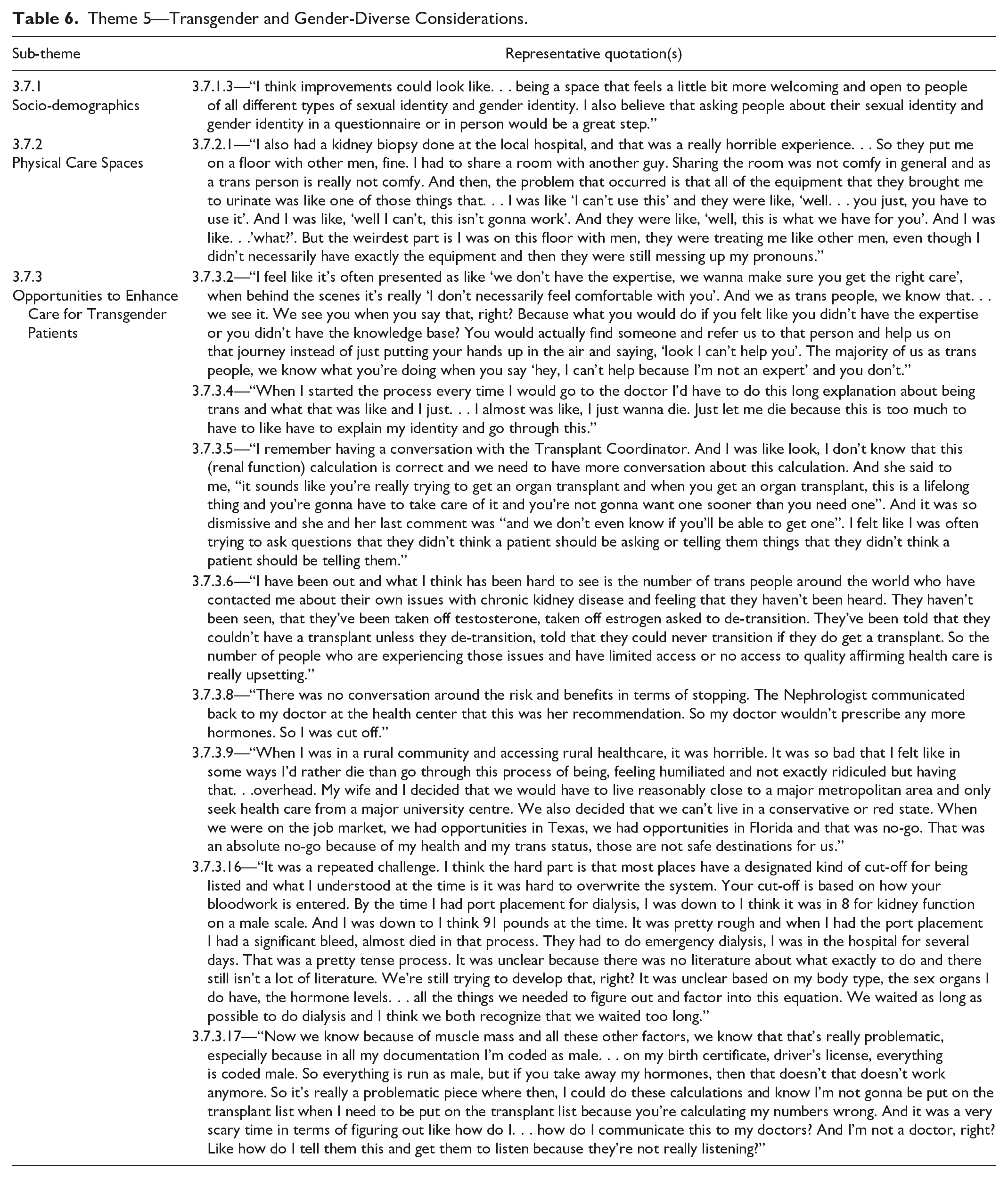
Material considerations
Interviewees identified practical considerations like available urine-collection systems and gender cohorting on hospital wards as factors that may uniquely impact a transgender patient’s experience (Table 6, Quote 3.7.2.1). Reflecting on their hospital stay in the peri-transplant period, one recipient recounted “I don’t think there are gender-neutral bathrooms. I remember the way the floor was divided, of girls’ rooms and boys’ rooms. And I also think that in terms of the activities in the hospital, it was also a boy versus girl type of thing. So I would understand that for someone that’s gender queer or someone that is non-binary that might be an issue for them.”
Opportunities to enhance care for TGD patients
Participants identified an ongoing need for enhanced gender-affirming care in OTDT systems. They identified under-recognized barriers for transgender people accessing care, for example, structural inequities such as a lack of expertise and education among healthcare providers leading to a void in the healthcare network. TGD patients expressed feelings of abandonment when lack of expertise was used as rationale to decline engaging in their care. When TGD patients were able to access care, they described harms related to the additional burden of needing to educate the healthcare team about their identity and specific needs (Table 6, Quotes 3.7.3.2 and 3.7.3.4) (Online Supplemental Appendix 2, Table 5, Quotes 3.7.3.1-3.7.3.4).
Participants highlighted existing knowledge gaps like the application of sex-based biometrics in TGD patients and described a disproportionate burden of having to research their own health issues and advocate for personalized care plans (Table 6, Quote 3.7.3.5). Transgender patients having their gender-affirming hormone therapy (GAHT) discontinued or withheld without their input to access transplantation was a recurrent described harm (Table 6, Quote 3.7.3.6) (Online Supplemental Appendix 2, Table 5, Quotes 3.7.3.6-3.7.3.7). Participants framed this lack of shared decision-making in stopping GAHT as a violation of patient autonomy (Table 6, Quote 3.7.3.8).
Less access to gender-affirming care was reported in smaller and rural centers with TGD transplant recipients describing how their career choices and housing selection were restricted by the need to access inclusive medical care (Table 6, Quote 3.7.3.9). Patients reported needing healthcare directives to avoid certain facilities in the event they could not advocate for themselves due to distrust that they would receive acceptable care. Travel for personal or professional reasons was also limited by the need to have access to inclusive emergency care (Online Supplemental Appendix 2, Table 5, Quotes 3.7.3.10-3.7.3.11). Patients described incidents where their identities were directly invalidated by healthcare staff, exposing a need for enhanced healthcare worker training (Online Supplemental Appendix 2, Table 5, Quotes 3.7.3.12-3.7.3.13).
Reported transgender-specific knowledge gaps in OTDT included invisibility and under-representation of transgender identities in research, uncertainty in how sex-based biometrics should be applied to transgender patients on and off GAHT, and incomplete understanding of the risks and benefits of GAHT in the peri- and post-transplant period. Transgender-specific knowledge gaps directly impacted access to pre-emptive kidney transplantation due to kidney function calculations modified by sex assigned at birth rather than gender identity (Online Supplemental Appendix 2, Table 5, Quotes 3.7.3.14-3.7.3.15). Interviewees described other complications of organ failure due to barriers in accessing pre-emptive transplantation including complications from a dialysis catheter placement which could have been prevented had their listing for transplant not been delayed due to sex-based kidney function criteria. Additional stress in needing to self-advocate and feeling unheard by OTDT providers was described as a harm experienced by transgender patients (Table 6, Quotes 3.7.3.16-3.7.3.17) (Online Supplemental Appendix 2, Table 5, Quotes 3.7.3.16-3.7.3.19).
Benefits of gender-affirming care
Participants shared their hopes for equitable care in the future and more personalization of care for transgender people. Examples of affirming experiences included the structural integration of a patient navigator/advocacy service (Online Supplemental Appendix 2, Table 5, Quote 3.7.4.1). Patients described relief and validation when they were able to access inclusive gender-affirming care. “At my current transplant institute they immediately put me back on hormones. I remember the first time talking to a transplant doctor. I was like, ‘hey, so look here’s the deal, I’m a transgender guy I’ve had hormones for almost 20 years. Here’s what’s happening.’ And she was like ‘okay.’ And I was like, ‘wait, do like, did you hear me? Like I am a trans guy. And so I may need different care.’ She was like ‘okay,’ like it was like nothing. And that was repeatedly my experience at my current hospital. Which was wonderful. It’s absolutely wonderful.”
Theme 6—SGM Priorities, Harms and Opportunities for Improvement
Sex-positive sexual and reproductive healthcare
Participants reported insufficient sexual and reproductive healthcare in their transplant programs. Some attributed this to vulnerabilities in the unique intersection of care they inhabit between primary healthcare and subspecialty transplant care (Table 7, Quotes 3.8.1.2-3.8.1.9). SGM-identifying transplant recipients revealed several barriers to accessing sex-positive care. Healthcare providers framing sexual health interventions as optional, unnecessary, or separate from more important medical issues was a barrier to holistic care. Access to pre-exposure prophylaxis (PrEP) and M-Pox vaccination were specific examples of interventions framed as unnecessary (Online Supplemental Appendix 2, Table 6, Quotes 3.8.1.10-3.8.1.11).
Theme 6—SGM Priorities and Opportunities for Improvement.

Insufficient healthcare provider training in sexual and reproductive health for SGM populations was a noted barrier. “What I discovered is that it wasn’t so much my sexuality that they didn’t want to talk about. They didn’t know how to talk about sex, period. I’ve never seen my nephrologist blush as much as when I asked him about sexual function and kidney disease, and how I would like to be sexually active. And I swear he turned multiple shades of red right in front of me. It was like, ‘okay, I’m asking you this question but it’s obvious it’s not my sexuality that you’re nervous about. . . it’s that you don’t know how to talk about sex.” Ingrained heteronormative assumptions can lead to misunderstandings when taking a sexual history and SGM patients may be uncomfortable disclosing sexual health concerns, further supporting the need for training healthcare providers in inclusive sex-positive care (Online Supplemental Appendix 2, Table 6, Quotes 3.8.1.13-3.8.1.15). Many transplant recipients described a disproportionate need to research their own health issues and self-advocate for access to sexual and reproductive healthcare (Table 7, Quotes 3.8.1.16-3.8.1.20).
Described sexual and reproductive health-related harms included stigmatization of SGM sex as being inherently “risky,” being prescribed abstinence over other risk-reductive strategies, transgender patients being forced to de-transition or denied GAHT to access transplantation, perceptions of SGM patients being used for medical teaching, and having one’s identity disrespected or disregarded (Online Supplemental Appendix 2, Table 6, Quotes 3.8.1.21-3.8.1.24).
Knowledge and practice gaps
Interviewees identified a unique need for enhanced sex-positive sexual and reproductive healthcare as a gap that transplant recipients were specifically impacted by. Transplant visits were identified as opportunities to interface with the medical system and participate in sexual and reproductive health promotion. One transplant recipient shared the disproportionate amount of time and advocacy it took to be able to access human papillomavirus (HPV) vaccination recognizing internal and external barriers (Table 7, Quote 3.8.2.2-3.8.2.3). Interviewees identified additional opportunities to integrate preventative health measures into the transplant system through enhanced education and screening for virally mediated malignancies for all patients. Coordination of care between primary care and subspecialty transplant care as a barrier to be overcome was a repeated theme (Online Supplemental Appendix 2, Table 6, Quotes 3.8.2.1-3.8.2.5).
SGM and OTDT community
Participants described the development of spaces where SGM transplant recipients could meet to share information and provide peer support in reaction to queerphobic discrimination they had faced in general transplant support networks. Representation of the diversity of SGM people including transplant recipients, people with disabilities, different races and ethnicities was described as a benefit of SGM-inclusive transplant support networks (Table 7, Quote 3.8.3.1). Virtual spaces like online discussion groups were used by SGM transplant patients in search of inclusive peer support. Interviewees also noted the potential of an SGM OTDT network to help SGM transplant candidates find a living donor (Online Supplemental Appendix 2, Table 6, Quotes 3.8.3.1-3.8.3.9).
Pediatric considerations
Pediatric transplant recipients were felt to be uniquely vulnerable to harms in the context of evolving identities. The interplay of developing sexual identities and sexual orientations along with a medicalized identity, a disability identity, ethnicity, and migrant status uniquely impacted patients. Participants called for more awareness of the complexities of supporting SGM pediatric patients with organ failure and transplantation. Described harms of non-inclusive care included low self-worth, isolation, and exposure to sexual violence (Table 7, Quotes 3.8.4.1-3.8.4.2).
Theme 7—Intersecting Identities
Interviewees highlighted how additional intersecting identities may uniquely impact an SGM patient or caregiver’s journey through the OTDT system. (Online Supplemental Appendix 4).
Improving SGM Care in OTDT
Targets for system improvement extracted from patient and caregiver interviews are summarized in Figure 1.

Emerging targets for action.
Discussion
TGD Considerations
Representation of TGD identities and experiences in OTDT systems is lacking in published literature. 1 Participant descriptions of delaying or avoiding needed healthcare due to fears of discrimination were poignant and are consistent with barriers to accessing healthcare for TGD populations in the larger health system.11-15 Transgender transplant recipients described a lack of trust in the OTDT system due to experiences of discrimination and threatened access to GAHT. Described forced de-transitioning or barriers to accessing GAHT in exchange for access to transplantation is a critical finding that warrants a coordinated position statement from decision-making bodies in OTDT. Just as transplantation is life-saving in end-organ failure, GAHT is life-saving in TGD patients with gender dysphoria. 16 Physicians are the gatekeepers of medical and surgical transition therapies which are essential to living as one’s true self for many TGD people. Decisions to withhold GAHT should be evidence-based and include shared decision-making with patients. There are significant knowledge gaps in OTDT for TGD patients which need to be addressed to support inclusive data-driven care.1,16-18 Interpreting sex-based biometrics in TGD patients and the potential effects and interactions of GAHT in post-transplant patients are priority areas of research.16-18 Interviewees clearly identified the need for enhanced healthcare worker training in TGD health and cultural humility. ODOs in Canada have also self-identified gaps in training in the provision of SGM-specific care. 5
Trans-joy was evident through participant descriptions of examples of inclusive and affirming care. Medical literature on TGD experiences is often from a deficit-based perspective to describe inequities 15 but strengths-based approaches can identify and reinforce human capacities rather than deficiencies. 19 The framing of a marginalized population in medical literature permeates both education and clinical practice. A strengths-based approach offers an opportunity to focus on wellness and thriving and to de-stigmatize deficit narratives that can subconsciously influence social perspectives and perpetuate deficit-based healthcare approaches.19-22 Recognizing TGD identities through inclusive collection of gender, pronouns and other sociodemographic data, acknowledging the importance of GAHT and facilitating access where appropriate, exhibiting an understanding of TGD specific issues and willingness to provide ongoing care without threatening this identity were all examples of clinicians supporting trans-joy in our interviews.
Sexual and Reproductive Healthcare
Transplant recipients face a unique barrier in accessing sexual and reproductive healthcare, which is typically provided in primary healthcare settings, as they receive much of their care in specialty transplant spaces. They described a deficit in this expertise in transplant providers, yet primary care teams were at times uncomfortable providing this care due to a lack of expertise in transplant recipient-specific issues. SGM transplant recipient interviewees described their transplant teams as being ill-equipped to provide sexual and reproductive health care, a finding that is echoed in the general transplant recipient population.23-26 Transplant providers themselves also identify a need for enhanced training.25,23,27,28 Team-based models that integrate primary care providers into the specialty care of transplant recipients might address this gap in care. Recommendations to promote sexual and reproductive health for general populations of transplant recipients have been published29,30 but specific guidance for SGM populations is lacking. Evidence to inform post-transplant fertility along with GAHT is needed.
Transplant recipients have a significantly increased risk of HPV-associated malignancies, treatment refractory HPV disease, and decreased immune response to HPV vaccination compared to the general population. 30 Guidance on screening, vaccination, and confirmation of immunity for HPV in transplant recipients exist but uptake and implementation of these recommendations may be heterogenous, as was the experience of some interviewees. 30
Our participants reported barriers in accessing HIV preventative PrEP which is highly effective at preventing sexual transmission of HIV.31,32 Awareness of potential drug interactions in transplant recipients (primarily with calcineurin inhibitors) and education on PrEP prescribing and monitoring could increase access to these therapies that have revolutionized HIV prevention efforts.29,33 Additional questions about the efficacy and safety of HIV post-exposure prophylaxis for transplant recipients being offered increased infectious risk donor organs or tissues are unanswered. Concerningly, some participants reported healthcare providers recommending abstinence to prevent HIV, which has been shown to be ineffective. 34 While the use of HIV PrEP is highly effective at preventing HIV transmission through sexual contact,31,32 there is limited experience in the peri-transplant setting with concerns about the risk of renal impairment.
Interviewees described a disproportionate burden of self-advocacy with multiple providers for access to SGM-specific sexual and reproductive healthcare. Decreasing access barriers and supporting shared decision-making with patients is needed. Descriptions of pediatric transplant candidate and recipient perspectives identified a unique intersection where the co-evolution of sexual identity, orientation, and gender identity in combination with a chronic illness made these patients uniquely vulnerable to stressors and at risk of harms including sexual violence when communication was not open and transparent. Patient and caregiver perspectives combined with healthcare provider self-assessments all support that comprehensive education for staff in all parts of the OTDT system on SGM health and cultural humility is needed.
Recognizing the need for enhanced programming, interviewees described SGM populations as having enhanced capacities in social and medical activism born out of a history of discrimination in these spaces. They identified these skills as supporting a sex-positive culture that was uniquely able to engage in HIV detection, prevention, and treatment efforts. In Canada, the proportion of new HIV infections in SGM populations is decreasing and SGM populations are more likely to be aware of their status, engage in regular testing, use effective HIV prevention methods, and for those living with HIV more likely to have undetectable viral levels. 35 These skills make SGM populations ideal partners in enhancing sexual and reproductive healthcare.
Strengths and Limitations
This study characterizes novel lived experiences of SGM patients and caregivers in transplantation systems. These have not been previously published in the medical literature. Patients and caregivers identified actionable targets to enhance inclusive care. We recognize that not all SGM identities or perspectives have been represented, in particular TGD, bisexual and lesbian perspectives were minimally represented and this is a limitation of our sample. For transformational health system change to occur, patient and caregiver experiences will need to be combined with the perspectives of healthcare providers and OTDT system stakeholders.
Conclusions
Our study characterized the priorities and perspectives of SGM patients and caregivers with lived experience of the organ transplantation system. Actionable targets include addressing knowledge and policy gaps for TGD patients and processes to ensure support and safety for SGM pediatric patients. Patients and caregivers called for enhanced healthcare provider training in SGM-specific topics. Expanded sexual and reproductive health service offerings were desired by transplant recipients who described barriers in accessing this care. OTDT systems should use these patient and caregiver priorities as catalysts to further improve inclusive healthcare delivery.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251331703 – Supplemental material for Lived Experiences of Sexual and Gender Minorities in Solid Organ Transplantation: A Best-Fit Framework Synthesis and Inductive Thematic Analysis
Supplemental material, sj-docx-1-cjk-10.1177_20543581251331703 for Lived Experiences of Sexual and Gender Minorities in Solid Organ Transplantation: A Best-Fit Framework Synthesis and Inductive Thematic Analysis by Murdoch Leeies, Carmen Hrymak, David Collister, Emily Christie, Karen Doucette, Ogai Sherzoi, Tricia Carta, Ken Sutha, Cameron T. Whitley, Tzu-Hao Lee, Matthew J. Weiss, Sonny Dhanani and Julie Ho in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-docx-2-cjk-10.1177_20543581251331703 – Supplemental material for Lived Experiences of Sexual and Gender Minorities in Solid Organ Transplantation: A Best-Fit Framework Synthesis and Inductive Thematic Analysis
Supplemental material, sj-docx-2-cjk-10.1177_20543581251331703 for Lived Experiences of Sexual and Gender Minorities in Solid Organ Transplantation: A Best-Fit Framework Synthesis and Inductive Thematic Analysis by Murdoch Leeies, Carmen Hrymak, David Collister, Emily Christie, Karen Doucette, Ogai Sherzoi, Tricia Carta, Ken Sutha, Cameron T. Whitley, Tzu-Hao Lee, Matthew J. Weiss, Sonny Dhanani and Julie Ho in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-docx-3-cjk-10.1177_20543581251331703 – Supplemental material for Lived Experiences of Sexual and Gender Minorities in Solid Organ Transplantation: A Best-Fit Framework Synthesis and Inductive Thematic Analysis
Supplemental material, sj-docx-3-cjk-10.1177_20543581251331703 for Lived Experiences of Sexual and Gender Minorities in Solid Organ Transplantation: A Best-Fit Framework Synthesis and Inductive Thematic Analysis by Murdoch Leeies, Carmen Hrymak, David Collister, Emily Christie, Karen Doucette, Ogai Sherzoi, Tricia Carta, Ken Sutha, Cameron T. Whitley, Tzu-Hao Lee, Matthew J. Weiss, Sonny Dhanani and Julie Ho in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-docx-4-cjk-10.1177_20543581251331703 – Supplemental material for Lived Experiences of Sexual and Gender Minorities in Solid Organ Transplantation: A Best-Fit Framework Synthesis and Inductive Thematic Analysis
Supplemental material, sj-docx-4-cjk-10.1177_20543581251331703 for Lived Experiences of Sexual and Gender Minorities in Solid Organ Transplantation: A Best-Fit Framework Synthesis and Inductive Thematic Analysis by Murdoch Leeies, Carmen Hrymak, David Collister, Emily Christie, Karen Doucette, Ogai Sherzoi, Tricia Carta, Ken Sutha, Cameron T. Whitley, Tzu-Hao Lee, Matthew J. Weiss, Sonny Dhanani and Julie Ho in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
We would like to acknowledge the value of the contributions of the Sexual Orientation and Gender Identity in Organ and Tissue Donation and Transplantation Patient and Caregiver Advisory Team, without which this work would not have been possible. We hope the perspectives and priorities of patients and caregivers with lived experiences will enable patient-centered improvements in donation and transplantation systems to support inclusive and affirming care for sexual and gender minorities and all patients and caregivers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the University of Manitoba Center for Healthcare Innovation via the Preparing for Research by Engaging Public and Patient Partners (PREPPP) Award.
Ethics Approval
The University of Manitoba Research Ethics Board provided approval for this study (HS26020(H2023:172)).
Consent to Participate
Not applicable.
Consent for Publication
Consent for publication was obtained from all authors.
Availability of Data and Materials
No data or material available as this is a study protocol.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.