
Abstract
Background:
Obesity can be an issue for renal transplant eligibility. Semaglutide constitutes an interesting choice for obesity treatment, but little data exist regarding its efficacy and security among dialysis patients.
Objectives:
The co-primary endpoints of this study were to describe the change in body weight (%) and in body mass index (BMI) from the beginning and after 3, 6, and 12 months of treatment for participants who used semaglutide compared with a control group of non-users. Secondary endpoints included description of dosages used and reported adverse events.
Design:
Multicenter cross-sectional descriptive study.
Setting:
Seven hemodialysis centers in Quebec and New Brunswick, Canada.
Patients:
Adults receiving hemodialysis treatment with BMI of at least 30 kg/m2 were included.
Measurements:
Weight as defined by the target body weight (kg) at the end of dialysis. Body mass index is defined by weight, kg/m2.
Methods:
As a primary objective, we collected in records the body weights and calculated BMI at months 0, 3, 6, and 12 for participants with BMI of 30 kg/m2 or greater. The dosages of semaglutide and the mention of any adverse events were also collected from questionnaire to participants, to community drug stores, and from records.
Results:
A total of 1286 patients received hemodialysis treatments in June 2023. Of these, 396 (31%) had a BMI of 30 kg/m2 or greater. Two hundred fifty-one participants were included in the study and 41 (16%) received semaglutide. The estimated treatment differences for the percentage change in body weight from baseline to 3, 6, and 12 months for semaglutide compared with the control group were −2.26%, 95% confidence interval (CI), −3.68 to −0.84, P = .002; −0.94%, 95% CI, −2.17 to 0.29, P = 0.135; and −0.64%; 95% CI, −2.04 to 0.76, P = .370, respectively. The estimated treatment differences at 3, 6, and 12 months for BMI were −0.87 kg/m2, 95% CI, −1.38 to −0.36, P < .001; −0.35 kg/m2, 95% CI, −0.79 to 0.09, P = .119; and −0.23 kg/m2, 95% CI, −0.72 to 0.27, P = .371, respectively. The estimated treatment difference in body weight and BMI change between the 2 groups was statistically significant at 3 months. A sensitivity analysis was carried out with all the participants of the semaglutide group who continued the treatment for 12 months (N = 15). The estimated treatment differences for the percentage change in body weight between this group and the control group were −3.04%, 95% CI, −5.18 to −0.89, P = .006; −1.97%, 95% CI, −3.79 to −0.14, P = .035; and −2.83%, 95% CI, −4.66 to −1.00, P = .003 at 3, 6, and 12 months, respectively. The average body weight change between months 0 and 12 was −3.88 ± 7.90 kg in the semaglutide group compared with −0.52 ± 5.53 kg in the control group (P = .015). With the sensitivity analysis, the body weight change between Months 0 and 12 was −6.83 ± 6.90 kg for the participants who continued their treatment for 12 months. The dosage of 1 mg of semaglutide was the most prescribed (49%). The occurrence of adverse events led to dose reduction in 5 participants (12%) and to treatment discontinuation in 13 participants (32%).
Limitations:
This study has several limitations, including its non-randomized design, short follow-up period, small sample size, and incomplete data on treatment compliance and adverse effects. Differences in patient characteristics, limited semaglutide doses for weight loss, and declining sample sizes over time further reduce the strength of conclusions, necessitating cautious interpretation of group comparisons.
Conclusions:
This study suggests that semaglutide promotes weight loss in hemodialyzed adults with obesity, but discontinuation of treatment was frequent and common adverse events were reported.
Introduction
Obesity is defined by a body mass index (BMI) higher than 30 kg/m2. It is associated with many chronic conditions, such as hypertension, cardiovascular diseases, and diabetes. 1 During kidney transplantation, it is associated with an increased risk of mortality, operative wound complications, delayed engraftment, acute rejections, and prolonged hospital stays. 2 The Canadian Society of Transplantation recommends supervised weight-loss therapy for obese candidates with target BMI < 30 kg/m2 (grade B), 3 and the latest KDIGO (Kidney Disease: Improving Global Outcomes) guidelines suggest offering weight-loss intervention to candidates with obesity prior to transplantation (2D). Patients with a BMI ≥ 35 kg/m2 should be considered for interventions, such as dietary counseling or bariatric surgery prior to transplantation. Those with a BMI ≥ 40 kg/m2 should be approached with caution, as there is an increased risk of post-operative complications. 2
When obesity is restricting a patient’s eligibility for renal transplantation, it is critical to do everything possible to support the patient’s attainment of the target body weight or BMI. Obesity management typically includes pharmacotherapy, nutritional counseling, psychological support, and physical activity, 4 but the efficacy and safety of obesity treatments have not been studied for patients with terminal kidney disease who are receiving hemodialysis treatments. Semaglutide has demonstrated a favorable efficacy and safety profile for participants with normal kidney function or renal insufficiency down to 15 ml/min/1.73m2.5,6 There is, however, little data for patients who are receiving hemodialysis treatments, which limit its use for these people, even though they could potentially benefit from it.7-12
This study aims to describe the use of semaglutide and the body weight change generated by this therapy for obese adults who are receiving hemodialysis treatments.
Materials and Methods
Study Design and Population
This multi-center cross-sectional descriptive study was carried out in Canada at 6 Francophone hospital centers that offer hemodialysis treatments in Québec and 1 in New Brunswick.
Potentially eligible participants were selected through a 2-phase process. First, the body weight and height of all the participants receiving hemodialysis treatment between May 28 and June 10, 2023, were collected from medical records, to calculate their BMI. Second, obese adults with a BMI of 30 kg/m2 or more were approached to be included in the study. The exclusion criteria were as follows: pregnant or nursing women, presence of active cancer, previous bariatric surgery, personal history of thyroid cancer, multiple endocrine neoplasia syndrome type 2, or taking one of the suggested weight-loss medications (liraglutide, orlistat, or bupropion + naltrexone).
Data Collection and Study Variables
Data collection was carried out between June 2023 and March 2024. The participants included began by answering a questionnaire about their prior or current use or non-use of weight-loss medication (semaglutide, liraglutide, orlistat, or bupropion + naltrexone), the occurrence of adverse events related to semaglutide (nausea, vomiting, diarrhea, or other), physical activity practices or diets, as well as whether they have a professional (nutritionist, kinesiologist, or other) to support them in their weight loss. A questionnaire was also sent to the participants’ pharmacies to collect the following information: whether they had a prescription for semaglutide between January 2021 and March 2024, the doses used, dispense dates, dosage change, or discontinuation of treatment, any notes in their file concerning adverse events, and whether they had a liraglutide, orlistat, or bupropion + naltrexone prescription. Based on questionnaire responses, participants who had received semaglutide since 2021 were assigned to the semaglutide group, while others formed the control group. Participants who had received weight-loss medication other than semaglutide since 2021 were excluded. Those who had started and then stopped semaglutide or other weight-loss medication before beginning their hemodialysis treatment were assigned to the control group.
The medical records were consulted to collect the following data: sex, age, weight, height, amputation history, kidney failure etiology, history of hypertension, cardiovascular disease, or diabetes and presence of exclusion criteria. Glycated hemoglobin (HbA1c) was collected at baseline then at an interval between 0 and 6 months, and between 6 and 12 months.
For the participants in the semaglutide group, their target body weight at the end of dialysis was taken just before they started semaglutide and then 3, 6, and 12 months after the start of the treatment. The body weights of the participants who stopped the treatment within 12 months of commencement were taken on the same schedule. The occurrence of adverse events was sought in the records, based on the dose reduction or treatment cessation dates, and on the participants’ and pharmacies’ questionnaires. For the control group, their target body weight at the end of dialysis was collected systematically on June 1, September 1 and December 1, 2022, and on June 1, 2023 (± 7 days), which corresponds to the body weight at 0, 3, 6, and 12 months for the participants selected during the recruitment period in June 2023. For participants who began dialysis between March 1, 2022, and the recruitment period, the body weights were taken 3 months after they started dialysis (time 0) and then 3, 6, and 12 months later. The study data were then anonymized by being assigned a random number before being compiled using REDcap. Each center kept a password-protected Excel file associating the participant file with its randomized number, so that, the collaborators could refer to it if any data appeared to be missing.
End Points and Assessments
The study’s main objective was to describe the change in body weight (%) and BMI (kg/m2) from the beginning of the treatment and after 3, 6, and 12 months of treatment for the participants in each group. The study also had 7 secondary objectives: (1) Describe the proportion of all hemodialyzed participants who have a BMI of 30 kg/m2 or more. (2) Describe the proportion of hemodialyzed participants who have a BMI of 30 kg/m2 or more and who have received a prescription for semaglutide since 2021. Of the participants who received semaglutide: (3) Describe the proportion of participants who change BMI category (≥ 30 to < 35, ≥ 35 to < 40, and ≥ 40 kg/m2). (4) Describe the average body weight lost (kg) in the year following commencement of the treatment. (5) Describe the proportion of participants who suffered adverse effects that led to a dose reduction. (6) Describe the proportion of participants who suffered severe adverse effects that led to the cessation of the medication, an unplanned medical visit, hospitalization, or death. (7) Describe the proportion of participants who stopped the treatment for any reason.
Ethics Approval
This study is supported by a research grant from l’Association des pharmaciens des établissements de santé du Québec (A.P.E.S.). The study protocol was approved by the CIUSSS de l’Estrie-CHUS independent research ethics committee (MP-31-2023-5065) and by the institutional review board at each participating center. All the participants included in the study signed the study information and consent form. The investigators were responsible for data collection. All the authors had full access to the study data, participated in drafting the manuscript, approved its submission for publication, and vouch for the accuracy and completeness of the data and the trial’s fidelity to the protocol.
Statistical Analysis
Descriptive statistics were provided for the complete sample, as well as separately for each arm. Categorical data are presented using frequencies and percentages. Continuous data with a normal distribution are described using means and standard deviations, while non-normally distributed data are presented using medians and interquartile ranges (IQRs). Socio-demographic comparisons between the groups were evaluated using Student’s t test for continuous data (Mann-Whitney U test) and chi-square tests (Fisher’s exact test) for categorical variables. Normality was visually assessed using quantile-quantile plots and histograms. Given the longitudinal design, missing values at different time points were handled using maximum-likelihood estimation for mixed models. All tests were 2-tailed, with a significance level of 5%. Statistical analyses were performed using R v.4.3.0 (R Core Team, Vienna, Austria).
For the primary outcomes, linear mixed models were used to assess the evolution of body weights and BMIs in both groups over time, as the dependent variables consist of continuous data (absolute and relative differences in BMI and body weight) at various time points. A random intercept was incorporated at the participant level to account for the variability of repeated measures, and fixed effects were considered for arm, time, and their interaction. In addition, adjustments for age, sex, and diabetes were included in a multivariable model. It should be noted that sensitivity analysis was performed only with participants still receiving semaglutide at 12 months. The results are reported as model coefficients (mean differences) with 95% confidence intervals (CIs). Assumptions of residual normality and homoscedasticity were assessed visually using appropriate diagnostic plots, and transformations were applied when necessary.
Results
Study Participants
Between May 28 and June 10, 2023, a total of 1286 patients were hemodialyzed in the participating centers. Of these, 396 had a BMI of ≥ 30 kg/m2. After the exclusion criteria were applied, 251 agreed to take part in the study, 41 (16%) in the semaglutide group and 210 in the control group (Figure 1). At the time of data collection, 14/41 participants (34%) had stopped taking semaglutide after 1 to 5 months of treatment (13 participants due to side effects and 1 participant due to no reimbursement of the treatment) and 1 participant in the semaglutide group had stopped being hemodialyzed to begin peritoneal dialysis. The remaining 26 participants were still on semaglutide but not all had completed 12 months of treatment. Since some participants had not reached 3, 6, or 12 months of treatment, the body weights of 38, 35, and 24 participants were taken at 3, 6, and 12 months, and of these, 32, 22, and 15 participants were receiving active treatment with semaglutide at each of the steps. The duration of semaglutide use was 364 days (IQR) (184-366 days). It should be noted that during the study, 5 participants underwent kidney transplantation (3 in the semaglutide group and 2 in the control group) and 4 died (all in the control group).

Patient selection.
The demographic data are presented in Table 1. Participants in the semaglutide group were younger (62.8 vs 66.6 years) and had higher body weights (108.0 vs 96.7 kg) and higher BMI (37 vs 35 kg/m²) than those in the control group. There were more men (75.6% vs 57.2%) and more participants for whom the kidney disease etiology was glomerulonephritis (26.8% vs 10.5%). While the differences were non-significant, there were also more Caucasians (85.4% vs 78.6%) and diabetics (85.4% vs 72.4%) in the semaglutide group and they had higher HbA1c (7.17% vs 6.58%).
Baseline Characteristics of Trial Population.

Note. *Statistically significant difference. Data are N (%) or mean (GMD) and include all participants receiving hemodialysis between May 28 and June 10, 2023. Participants in the semaglutide group were younger, had higher body weights and higher BMIs than those in the control group. There were more men and more participants for whom the kidney disease etiology was glomerulonephritis. ¥ BW and height (for the calculation of BMI) was collected in the medical records at screening. HbA1c collected was the most recent value around Time 0. Etiology of kidney disease and comorbidities was collected in medical record. GMD = Gini mean difference, BW= body weight, BMI = body mass index, HbA1c = glycated hemoglobin, ACD = atherosclerotic coronary disease, AVD = atherosclerotic vascular disease, HTA = hypertension.
Primary Outcome
The results related to the main objectives are presented in Table 2 and are presented in an “Intention to Treat Analysis” (ITT analysis) including all those who took semaglutide for any duration. In the semaglutide group, weight loss was observed from the third month following the start of treatment. The mean percentage body weight change at 3 months was −2.33% with semaglutide vs −0.07% with the control group and it was −3.21% vs −0.08% at 6 months and −3.36% vs −0.47% at 12 months. The estimated treatment difference at 3, 6, and 12 months were −2.26%, 95% CI, −3.68 to −0.84, P = .002; −0.94%, 95% CI, −2.17 to 0.29, P = .135; and −0.64%, 95% CI, −2.04 to 0.76, P = .370 (Figure 2a), respectively. The mean changes in BMI in the semaglutide group were −0.90, −1.25, and −1.34 kg/m2 at 3, 6, and 12 months compared with −0.04, −0.06, and −0.24 kg/m2 for the control group, respectively. The estimated treatment differences at 3, 6, and 12 months were −0.87 kg/m2, 95% CI, −1.38 to −0.36, P < .001; −0.35 kg/m2, 95% CI, −0.79 to 0.09, P = .119; and −0.23 kg/m2, 95% CI, −0.72 to 0.27; P = .371, respectively. The estimated treatment difference in body weight and BMI change between the 2 groups is statistically significant at 3 months. The same effect was observed when the groups were balanced based on age, sex, and diabetes (Supplemental material).
Mean Change of Body Weight and Body Mass Index From Baseline To Month 12.

Data are N or mean (GMD). N = Available body weight at data collection. All participants were included in the treatment comparison (intention-to-treat analysis). The difference in body weight and BMI change between the 2 groups is statistically significant at 3 months.

Comparison of body weight parameters for semaglutide group and control group.
A sensitivity analysis was carried out with all the participants of the semaglutide group who continued the treatment for 12 months (N = 15). The estimated treatment differences between this group and the control group for percentage body weight change were −3.04%, 95% CI, −5.18 to −0.89, P = .006; −1.97%, 95% CI, −3.79 to −0.14, P = .035; and −2.83%, 95% CI, −4.66 to −1.00, P = .003 at 3, 6, and 12 months (Figure 2b), respectively. The participants’ weight loss can be observed within the first 3 months and continues for 12 months when the participants continue their treatment with semaglutide.
Secondary Outcome
Among all the dialyzed patients, 31% had a BMI of 30 kg/m2 or more and 10% had received a semaglutide prescription since 2021. In the “Intention to treat analysis”, the average body weight change between months 0 and 12 was −3.88 ± 7.90 kg in the semaglutide group compared with −0.52 ± 5.53 kg in the control group (P = .015). With the sensitivity analysis, the body weight change between months 0 and 12 was −6.83 ± 6.90 kg for the participants who continued their treatment for 12 months.
In the semaglutide group, the proportions of participants who reduced their body weight by 5%, 10%, and 15% were 38% (N = 9), 12% (N = 3), and 4% (N = 1) (ITT), compared with 19% (N = 34), 3% (N = 6), and 0.6% in the control group (N = 1). With the sensitivity analysis (N = 15), the proportions were 53% (N = 8), 20% (N = 3), and 7% (N = 1) (Figure 2c). The difference was statistically significant in both cases.
Among the participants in the semaglutide group (N = 41), 10 (24%) changed to a lower BMI category and 1 (2%) changed to a higher category (Table 3). With sensitivity analysis (N = 15), 5 (33%) participants changed to a lower BMI category and no participants changed to a higher category (Supplemental material).
Change of BMI Category From Baseline to 12 Months.
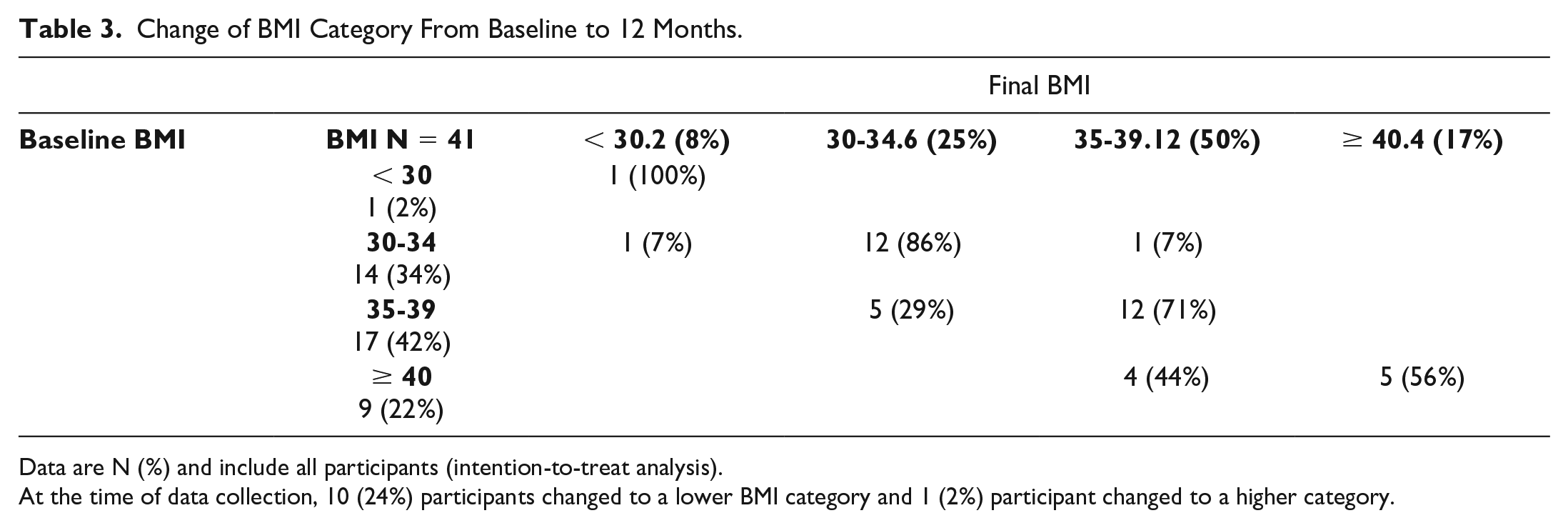
Data are N (%) and include all participants (intention-to-treat analysis).
At the time of data collection, 10 (24%) participants changed to a lower BMI category and 1 (2%) participant changed to a higher category.
Table 4 presents the prescribed doses of semaglutide, and the side effects reported during the study. The 1-mg dose was the most common final dose for 49% of the participants, according to the ITT analysis, and for 73% of the participants who were still on semaglutide at 12 months. Gastrointestinal disorders, namely, nausea and vomiting, were the most frequent adverse events reported in 24 (60%) participants. There were no adverse events that led to hospitalization or death. Semaglutide was stopped for 13 participants (32%) due to side effects and 1 participant due to no reimbursement of the treatment.
Dosages Used and Reported Adverse Events in the Semaglutide Group.

Note. Data are N (%) and include all participants in the full analysis. One participant did not answer the questionnaire. GI disorders were the most reported side effects. Any serious adverse events were reported but AE frequently leads to discontinuation of treatment.
According to the questionnaire responses, 34% of the participants were engaging in varying degrees of physical activity, 4% were on a diet, and 17% had a weight-loss program supervised by a professional.
Following the beginning of the treatment, the HbA1c tended to drop in the semaglutide group but this was not significant. The mean HbA1c between months 0 and 6 was 6.81% in semaglutide group compared with 6.66% in the control group and 6.67% vs 6.65% at 6 to 12 months. The estimated treatment difference was −0.26, 95% CI, −0.61 to 0.09, P = .145 and −0.22, 95% CI −0.62 to 0.17, P = .268.
Finally, between the recruitment period and the data collections, 4 participants, all in the control group, died, and 5 received transplants, 3 (7%) in the semaglutide group, and 2 (0.9%) in the control group.
Discussion
In our study, participants in the semaglutide group experienced a significant weight loss by 3 months of treatment. Participants who continued the treatment lost weight even at 6 and 12 months. Participants receiving semaglutide tolerated dosages up to 1 mg weekly over the long term but often experienced adverse gastrointestinal effects, which sometimes led to dose reduction or treatment discontinuation.
There are little data on the effect of semaglutide for weight loss among people with end-stage kidney disease who are receiving hemodialysis treatment (stage 5D). According to Granhall et al, 13 kidney disease has no impact on the pharmacokinetic properties of semaglutide, and this molecule is not eliminated by hemodialysis. Its use for dialyzed patients therefore seems safe. A few case reports have been published in the literature mentioning the efficacy of semaglutide for weight loss for these patients. Long et al 11 report decreases in weight, from 108 ± 24.5 to 104 ± 29.4 kg, among 78 participants with chronic kidney disease (CKD), including 8 patients in end-stage renal disease, and Thomas et al 14 reported an average loss of 5 ± 8 kg among 20 participants (CKD 5 + 5D) who received semaglutide. Two case reports were also published on the weekly use of semaglutide at a 1-mg dose: Touzot et al 9 reported weight losses of 6.5 and 9 kg for 2 participants (5D), and De la Flor reported a weight loss of 10.2% for 1 participant. 15 The results obtained in our study demonstrate a less considerable weight loss, that is, a loss of 3.88 ± 7.90 kg at 12 months, in an analysis including all the participants in the semaglutide group, whether or not they discontinued the treatment before the 12 months was up. This can be explained by the use of variable doses and the high dropout rate in our cohort. Only 15 of the 24 body weights (62.5%) available at 12 months were for participants still receiving semaglutide. The other 9 participants had stopped taking semaglutide after 1 to 5 months of treatment, and several of them had received maximum weekly doses of 0.25 and 0.5 mg. The sensitivity analysis showed, however, that when semaglutide is titrated to 1 mg and maintained, significant weight loss continued at 3, 6, and 12 months, with an average loss of 6.83 ± 6.90 kg. Among these participants, over 50% lost 5% or more of their body weight, which represents the minimum weight loss considered to be significant.5,6 These results are similar to the STEP 2 study, in which participants who received a weekly dose of semaglutide 1 mg for 68 weeks lost an average of 6.9 kg (vs 3.5 kg for placebo) and 57% of participants lost 5% or more of their body weight. The presence of gastrointestinal adverse events was comparable, as reported in 57.5% of the participants. 16
One study (RAISE-KT) measured the effect of taking 1 mg of semaglutide weekly on admittance to the kidney transplantation list: 15 participants (CKD 4-5D) were randomized (7 semaglutide and 8 placebo). After 9 months of treatment, 3/5 vs 0/7 participants were added to the kidney transplantation list. 17 During our study, 3 participants (7%) in the semaglutide group and 2 participants (0.9%) in the control group received transplants. The RAISE-KT and this study are underpowered to sufficiently evaluate this outcome, but the OK-TRANSPLANT 2 study could answer this hypothesis. This upcoming randomized control trial is planned to evaluate medication that can promote weight loss, including semaglutide, and a virtual weight management program in individuals hoping to lose weight for the purpose of kidney transplant (NCT06396416).
The BMI threshold to be eligible for kidney transplantation is not clearly defined and may differ from one transplantation center to another. While it is widely acknowledged that the eligibility of a patient with a BMI higher than 40 kg/m2 is risky, patients with a BMI between 35 and 40 kg/m2 may be considered based on certain criteria, including abdominal adiposity. When obese candidates are assessed for kidney transplantation, a weight-loss objective is often set. It is therefore beneficial to describe the proportion of participants who changed BMI category, because these categories are often used by the teams that assess eligibility for kidney transplantation. In our study, 10 participants changed to a lower BMI category. Of these, 4 participants in the BMI category of over 40 reduced their BMI to the 35 to 39 category, and 5 in the 35 to 39 category reduced their BMI to the 30 to 34 category, which can facilitate the goal of becoming a kidney transplantation candidate.
Although the Canadian Society of Transplantation recommends supervised weight-loss therapy for obese candidates, 3 very few participants reported on their questionnaire that they were receiving professional services or had access to a supervised program to support their weight loss, even though, in association with pharmacotherapy, this could potentially provide an additional benefit. Treatment provided as part of comprehensive obesity therapy, including a diet and an exercise program, may be even more effective, as demonstrated in the STEP program studies.5,6
Not surprisingly, the significant presence of adverse gastrointestinal effects influenced the doses prescribed and the continuation of treatment. Weekly doses of 1 mg were well tolerated, however, for 12 months and more, by 11 of the 15 participants who were still receiving active treatment at 12 months. One participant had even been tolerating a weekly supertherapeutic dose of 3 mg for 3 years.
This real-world study has limitations, including a non-randomized cross-sectional design, the short follow-up period and the limited sample size. A randomized prospective study could have more effectively validated the effect on weight loss, BMI change and treatment tolerance. Some information about treatment compliance or the presence of adverse effects was not systematically collected. The missing in weight measurements at the 12-month follow-up was primarily because 16 participants had not completed 12 months of treatment yet and not to loss of follow-up. However, the sample of body weights taken and the number of active treatments declined in each step at months 3, 6, and 12, reducing the quality of the outcomes. A higher number of participants may have been required to reveal a difference between the groups. Also, a longer observation period could have revealed additional weight loss. Indeed, in the STEP 5 trial, semaglutide 2.4 mg as an adjunct to behavioral intervention led to a substantial initial reduction in weight, which plateaued after approximately week 60. 18 Furthermore, the population under study was determined based on a list of patients being dialyzed between May 28 and June 10, 2023, with a BMI of 30 kg/m2 or more. The study would have been more complete if it included all participants who had been dialyzed since the publication of the key studies on semaglutide and weight loss in 2021. Some participants who had received semaglutide may have received transplants or lowered their BMI to below 30 kg/m2 and therefore not been included in the study. Finally, since public drug insurance only covers semaglutide for the treatment of diabetes, most of the participants treated were diabetic. Among the semaglutide group, only 6 participants were not diabetic. One participant stopped treatment after 1 month because it was not reimbursed, 2 participants had private insurance that reimbursed their treatment, and 3 participants received free samples. The majority of the participants were receiving the doses recommended for the treatment of diabetes. These doses are lower than those recommended for weight loss, offering limited insight into the effect and tolerance of semaglutide at the 2.4-mg dose recommended for weight loss. Comparing the body weight and BMI of the semaglutide group with a control group provides supplementary indicators on the effects of semaglutide, but the group comparison must be interpreted with care. The semaglutide group was slightly younger and involved more men and, oddly enough, more participants with glomerulonephritis. They were also more obese, which is not surprising, as semaglutide is the preferred diabetes treatment for patients with obesity. There were more deaths and fewer transplantations in the control group. This group may have included participants who were more ill and less likely to lose weight.
The main strength of this study is that the participants came from several regions of Québec and New Brunswick where there is a varied population and that it reflects the use of semaglutide in real time. Furthermore, the verification of semaglutide prescriptions and service using the computer systems of the pharmacies dispensing the treatment offers more reliable data than medical records about the commencement of treatment and dosage changes.
Conclusion
This study suggests that semaglutide promotes weight loss in hemodialyzed adults with obesity, but discontinuation of treatment was frequent and common side effects were reported. Further prospective studies could assess the effectiveness of semaglutide in a larger population, along with the impact of treatment on access to kidney transplantation in patients with stage 5 and 5D chronic kidney failure.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251324588 – Supplemental material for The Real-World Use of Semaglutide to Promote Weight Loss in Obese Adults With Hemodialysis: A Multicenter Cross-Sectional Descriptive Study
Supplemental material, sj-docx-1-cjk-10.1177_20543581251324588 for The Real-World Use of Semaglutide to Promote Weight Loss in Obese Adults With Hemodialysis: A Multicenter Cross-Sectional Descriptive Study by Jodianne Couture, Pascale Robert, Marie-France Beauchesne, Gabriel Dallaire, Annie Lizotte, Jo-Annie Lafrenière, Julie Beauregard and Janique Doucet in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors thank Samuel Lemaire-Paquette, MSc, for his assistance with the statistical analyses. The authors also thank Gabriela Maria Zuniga, research assistant; Roxanne Couture, Tamara Kazwini, Justin Lafrenière, and Leyne Merrouche, pharmacy students; Josée Krupa, nurse and data collection compiler; and Guylaine Marcotte, research coordinator.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors’ first thanks go to the Association des pharmaciens des établissements de santé du Québec (A.P.E.S.) for allowing them to carry out this study independently through a research grant.
Ethics Approval
Ethical approval was granted by the CIUSSS de l’Estrie-CHUS independent research ethics committee and by the institutional review board at each participating center.
Consent to Participate
All participants provided written informed consent.
Consent for Publication
All the authors provide consent for publication.
Availability of Data and Materials
All data are available for sharing by the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.