
Abstract
Background:
Incremental hemodialysis, a strategy to individualize dialysis prescription based on residual kidney function, may be associated with enhanced quality of life and decreased health care costs compared with conventional hemodialysis.
Objective:
We surveyed practicing Canadian nephrologists to assess knowledge, perceptions, and practice pattern on the use of incremental hemodialysis.
Design/Setting:
We distributed a cross-sectional, web-based survey. We asked about incremental hemodialysis prescribing practices, including frequency of prescription, clinical factors used to determine suitability for treatment, and barriers to implementation. The survey was conducted from September 21 to October 30, 2020.
Participants:
We distributed the survey to practicing Canadian nephrologists identified from a private membership list of the Canadian Society of Nephrology (CSN), as well as to nephrologists named on a publicly available national list of practicing Canadian nephrologists created from provincial College of Physician registries. These were samples of convenience.
Methods:
We conducted descriptive analysis of categorical data including frequencies for nominal variables and measures of central tendency (mean) and dispersion (standard deviation) for ordinal variables. We used chi-square analysis to identify association between participant and practice characteristics and their opinions and attitudes toward incremental dialysis. We used simple thematic analysis on free-text responses on questions regarding the prescription of incremental hemodialysis, focusing on age and baseline management of cardiac and noncardiac comorbidities.
Results:
The response rate was 35% (243/691). Most (138/211, 65%) of the participants prescribed incremental hemodialysis using an individualized approach at the nephrologist’s discretion. Most participants (200/203, 98%) did not report any policy for implementation. Residual urine output was identified as the most important factor for eligibility (112/172, 65%), followed by electrolyte stability (76/172, 44%) and patient goals of care (69/117, 40%). Most participants agreed that dialysis prescriptions should take residual kidney function into consideration; however, 74% of the participants disagreed with a statement that there was strong evidence supporting incremental hemodialysis. Barriers identified included patient safety, patient acceptance of dose escalation, and logistics of scheduling. Despite these barriers, 82% of participants felt that that incremental hemodialysis is feasible with their current resources and 78% agreed that with specific criteria, it is a safe option.
Limitations:
The generalizability of our study is limited by its response rate of 35%; however, this is comparable with typical response rates seen in electronic surveys. Most participants practice in an academic setting, which may have introduced bias to the results.
Conclusions:
Despite the perception of limited evidence and a lack of guidance on implementation, incremental hemodialysis is frequently practiced by Canadian nephrologists. Barriers to implementation were identified, highlighting the need for research to guide practice.
Introduction
The number of patients requiring kidney replacement therapy in Canada is increasing annually due to shifts in population demographics and better survival of patients with end-stage kidney disease.1-3 Despite the increase in uptake of home-based dialysis therapies, more than 80% of patients with end-stage kidney disease in Canada are treated with facility-based hemodialysis. 2
The transition to dialysis is a challenging experience for most patients and is associated with a marked increase in hospitalization, morbidity, and mortality in the first 3 months. 4 The current dialysis prescription of establishing a Kt/Vurea of 1.2 with thrice-weekly dialysis was established by the Kidney Disease Outcomes Quality Initiative (KDOQI) based on the landmark National Cooperative Dialysis Study (NCDS) and Hemodialysis Study (HEMO) trials.5,6 Unfortunately, conventional hemodialysis prescriptions do not account for residual kidney function (RKF), which has previously been described as an important determinant of dialysis requirements and has been associated with improved cardiovascular outcomes, nutrition, phosphorous control, and middle molecule clearance.7,8 Furthermore, conventional hemodialysis is associated with repeated ischemic insults, which can contribute to rapid decline in RKF. 9
At present, most patients initiating hemodialysis, regardless of age, sex, comorbidity, weight, and RKF are given the same treatment prescription. Incremental hemodialysis has been proposed as a “gentler” approach to hemodialysis initiation, where the frequency and duration of dialysis sessions are individualized to account for RKF, increasing treatment delivery frequency and/or duration as kidney function decreases. 10 Regular monitoring of patients for uremic symptoms, volume status, and RKF through 24-h urine collection is performed. The 2015 update of the KDOQI clinical practice guidelines and the European Best Practices guidelines endorse this approach by suggesting RKF should be considered in the prescription of hemodialysis with modification of minimal adequacy targets; however, this has not been widely translated into clinical practice.11,12
An incremental approach to hemodialysis initiation may facilitate delivery of patient centered care while reducing the per patient cost of care delivery and increasing treatment capacity. 13 Anecdotally, it is known that there is use of incremental hemodialysis in Canada; however, the extent of use and current practice is unclear. We surveyed practicing Canadian nephrologists to assess knowledge, perceptions, and practice pattern on the use of incremental hemodialysis.
Methods
Design and Participants
A cross-sectional survey of nephrologists practicing in Canada was implemented using an online survey tool. The convenience sampling frame was practicing Canadian nephrologists, who were identified from a private membership list of the Canadian Society of Nephrology (CSN) as well as a publicly available national list of practicing Canadian nephrologists created from provincial College of Physician registries. Duplicates were removed from the combined list at the time of survey distribution so that nephrologists would be contacted once, yielding a final list of 691 practicing nephrologists in Canada with a publicly available email address.
Development and Validation of Survey Instrument
The first and last authors (A.D. and N.P.) developed a survey to assess attitudes toward and current practices of incremental hemodialysis. For the purposes of the survey, incremental hemodialysis was defined as prescription of facility-based hemodialysis in new patients (within 12 months) where hemodialysis is titrated based on RKF. This definition refers to hemodialysis started at less than 3 times per week and/or less than 4 h per session with the intention to titrate the treatment as needed. Items were generated through a review of the current literature and a focus group with 3 nephrologists. The pilot survey was peer reviewed for content validity and comprehensiveness. Pilot participants included 5 academic nephrologists with expertise in survey design, as well as an implementation scientist. The survey was revised based on their recommendations and subsequently formatted for online administration. The final questionnaire included 22 questions eliciting knowledge of incremental hemodialysis, opinions regarding various dialysis prescription factors, and perception of feasibility of incremental hemodialysis along with items eliciting demographic and practice characteristics of each participant (Supplementary Appendix 1). The demographic data included location of training, years in practice, dialysis provision model, practice style (academic vs private practice), and reimbursement structure (alternative relationship plan vs fee for service). Dialysis provision models included longitudinal care, in which nephrologists follow select patients throughout their dialysis care, shift-based, in which nephrologists follow patients during a designated dialysis shift, or a combination of the above models.
The final survey, including a combination of multiple-choice and free-text questions, was uploaded to the Select Survey platform (https://survey.albertahealthservices.ca), an online platform that provides anonymity for its users and is copyrighted by Alberta Health Services, the provincial health authority for the province of Alberta, Canada. The survey was only distributed in English.
Survey Administration
The CSN emailed the survey web link to all identified nephrologists as described above. The survey was delivered over a period of 6 weeks (September 21, 2020, and October 30, 2020). To optimize participation, reminders were sent weekly until the end of the survey period. Participants were informed that the confidentiality of the data would be protected and only aggregate results would be disseminated.
Data Analysis
The survey results were stored anonymously on the Select Survey platform prior to analysis. The data were subsequently exported to the Excel software (Microsoft Corp, Redmond, WA) for descriptive analysis of the categorical data. This analysis included frequencies for nominal variables and measures of central tendency (mean) and dispersion (standard deviation) for ordinal variables. Chi-square analysis was performed to identify association between participant and practice characteristics and their opinions and attitudes toward incremental dialysis. The level of statistical significance was set at .05.
Simple thematic analysis was used on free-text responses on questions regarding the prescription of incremental hemodialysis, focusing on age and baseline management of cardiac and noncardiac comorbidities. 14 Participants were also given the opportunity to provide free-text responses on perceived barriers to incremental hemodialysis. On the first level, the responses were read and transcribed independently by the first and last authors of the article (A.D. and N.P.). This was followed by a collaborative effort to determine overarching codes on incremental hemodialysis prescribing practices and perceived barriers to incremental hemodialysis. Finally, the identified themes were reviewed before being defined and written up. This study was approved by the Research Ethics Board at the University of Alberta (Pro00098076). The survey design and reporting was validated using the Checklist for Reporting Results of Internet E-Surveys. 15
Of the 691 nephrologists that were contacted, 243 responses were received (response rate of 35%). One hundred and sixty-one (66%) responses were 100% complete and 82 (34%) were at least 50% complete. Of these, 6 participants indicated that they did not provide dialysis treatment and were excluded from subsequent analysis; therefore, the total number of participants used in the final analysis was 237. Partially complete surveys were analyzed for the questions answered completely; if a question was not answered fully, it was excluded from analysis of that question.
Results
Demographic Information, Including Dialysis Practice, of Surveyed Participants
Characteristics of the participants are provided in Table 1. Most of the participants completed their nephrology training in Canada (92%), with 69% in practice for at least 10 years. Participants commonly had an academic practice (62%) and were reimbursed for dialysis using a fee for service model (69%). Seventy-seven percent of all participants spend more than 50% of their time on clinical work. Forty-four percent of participants used a longitudinal/continuous care model and 44% used a shift-based model of dialysis coverage. Participants providing longitudinal/continuous dialysis care more frequently provided dialysis for greater than 6 months of the year (21%) compared with those that provide shift-based care (8%). In both provision models, patients were most often seen weekly.
Demographic Information of Survey Participants, Including Dialysis Practice.

Note. ARP = alternate relationship plan; FFS = fee for service; HD = hemodialysis.
Sixty percent of participants worked in centers where there are more than 50 patients receiving facility-based hemodialysis (see Table 2). Sixty-five percent of participants reported prescribing incremental hemodialysis, with most of the prescriptions individualized. Finally, 98% of participants did not have center-specific criteria available for incremental hemodialysis. There was no significant association between prescription of incremental hemodialysis and participant or practice characteristics (results not shown).
Surveyed Participants Current Incremental Dialysis Practice.

Note. HD = hemodialysis.
Determination of Important Patient and Clinical Factors in Prescribing Incremental Hemodialysis
Participants were asked to rank a predefined list of patient factors (eg, goals of care), and clinical factors (eg, urine output), that they considered in the decision to provide incremental hemodialysis (see Figure 1). Urine output was the most important factor in the decision to prescribe incremental hemodialysis (65%), followed by electrolyte homeostasis and goals of care (44% and 40%, respectively). Forty-five percent of participants ranked “age” from important to critical. Participants were asked to provide additional details in a free-text response if they ranked “age” as important (see Table 3). Participants were more likely to consider incremental hemodialysis in the elderly population largely due to concerns regarding quality of life. In contrast, participants identified concern of patient acceptance of dose escalation and desire to optimize patients for possible transplantation when considering younger patients for incremental hemodialysis. Poor management of cardiac and volume-related comorbidities was identified as a possible deterrent to initiation of incremental hemodialysis. There was no significant association between ranking of patient and clinical factors in incremental hemodialysis prescriptions and participant or practice characteristics (results not shown).

Importance of certain patient and clinical factors in prescribing incremental hemodialysis.
Simple Thematic Analysis of Free-Text Responses.

Note. HD = hemodialysis; QOL = quality of life; CHF = congestive heart failure; ESLD = end-stage liver disease; eGFR = estimated glomerular filtration rate; RCT = randomized control trial; IDEAL = initiating dialysis early and late study; PD = peritoneal dialysis; ESKD = end-stage kidney disease.
Content displayed is unedited from original statements.
Opinions on Dialysis Prescribing Patterns, Including Incremental Hemodialysis
Participants were asked to rank the degree of agreement with various statements on dialysis prescribing patterns, including incremental dialysis (Figure 2). Most of the participants agree that dialysis prescriptions are dynamic (88%) and RKF is an important component in prescribing hemodialysis (81%). Although 74% of participants disagreed that there is strong evidence supporting incremental dialysis, 78% agreed that with specific inclusion and exclusion criteria, incremental dialysis is a safe option. Participants who provided shift-based dialysis care were more likely to agree that with specific criteria, incremental hemodialysis can be a safe dialysis modality (P = .05) (results not shown).
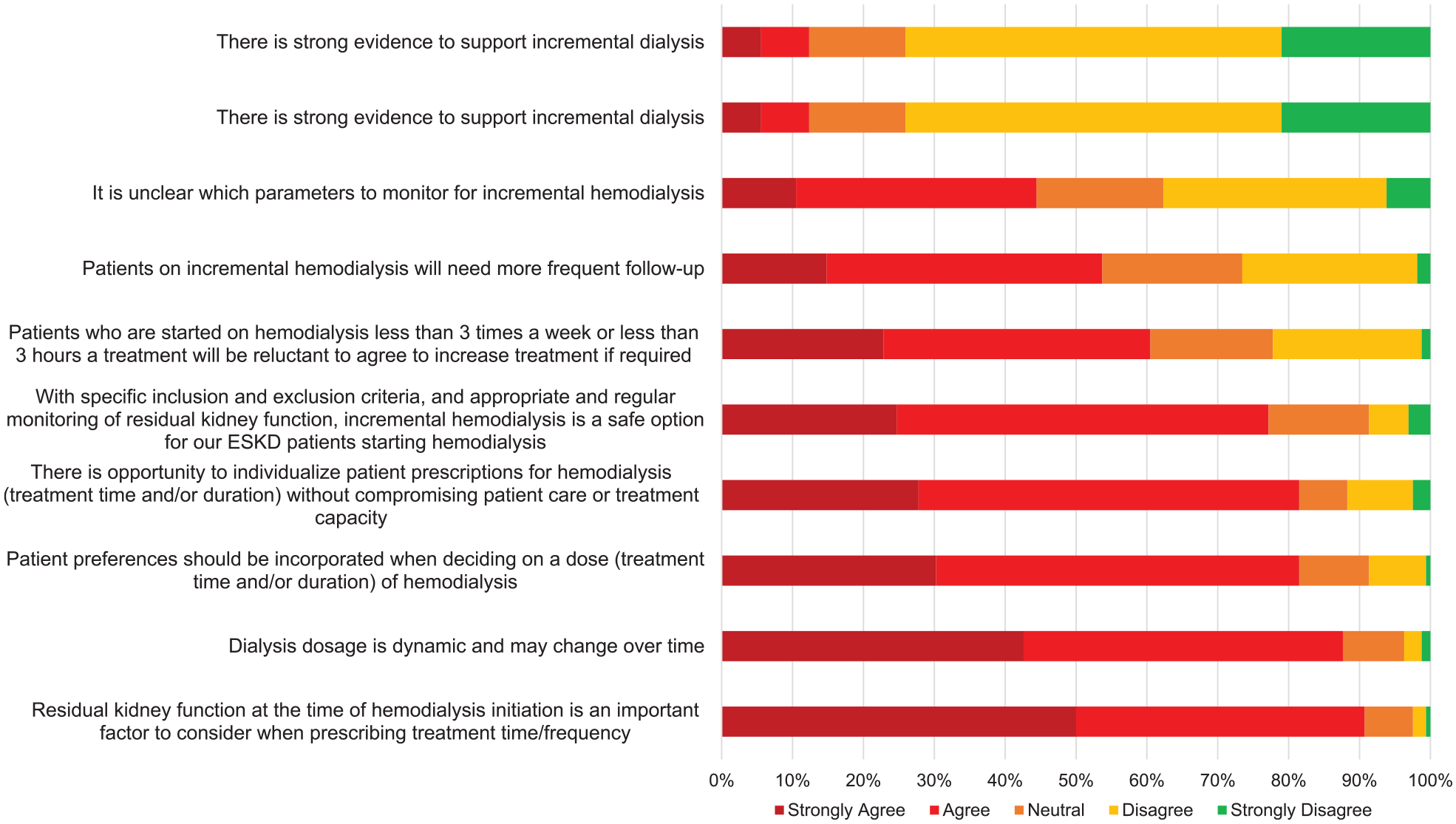
Degree of agreement with statements on dialysis prescriptions and incremental hemodialysis.
Barriers to Incremental Hemodialysis
Participants were asked to rank a prespecified list of potential barriers to designing an incremental dialysis program (see Figure 3). Lack of scientific evidence was identified as a barrier to incremental hemodialysis. Sixty-five percent of participants agreed that patient acceptance of dose escalation is somewhat/definite barrier. Participants who provided shift-based dialysis care were more likely to identify patient acceptance of dose escalation as a barrier to incremental hemodialysis (P = .003) (results not shown). Furthermore, participants who work in an academic practice were more likely to identify continuity of care as a barrier to incremental hemodialysis (P = .047). Participants who completed their nephrology training in Canada were more likely to identify patient safety as a barrier to incremental hemodialysis (P = .0006).

Potential barriers to incremental hemodialysis.
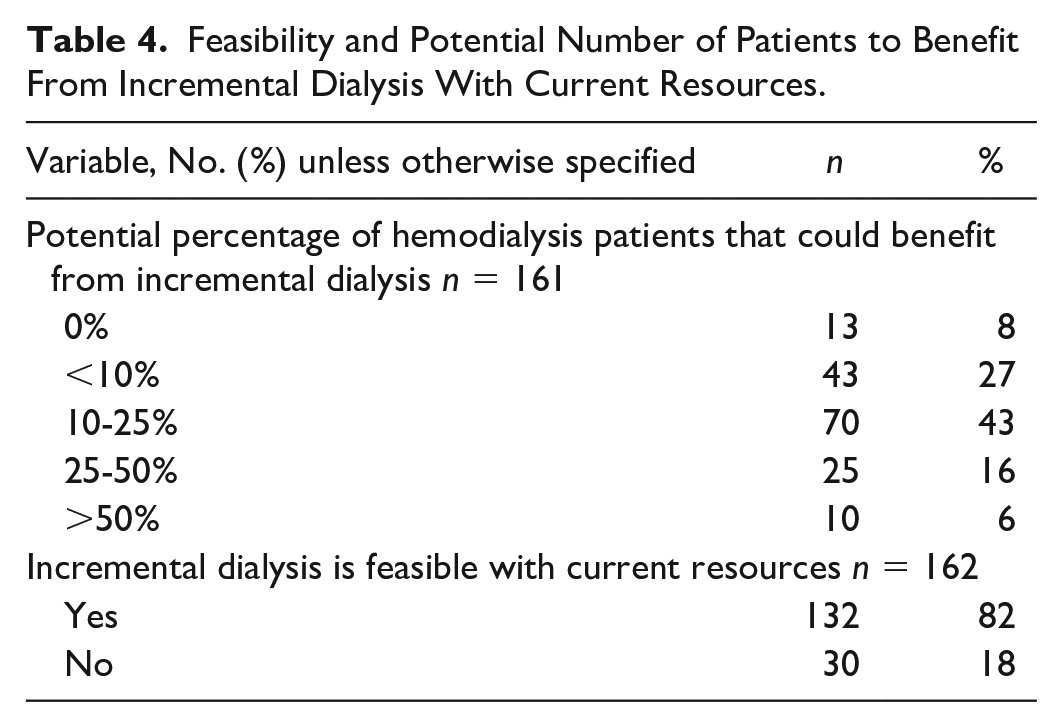
Participants were asked to provide free-text responses on potential barriers to incremental hemodialysis (see Table 3). Simple thematic analysis revealed concerns regarding limited scientific evidence in the form of randomized trials. Furthermore, participants had stated that centers are often over-capacity and it will be challenging to accommodate the individual schedules required for incremental hemodialysis. Finally, participants expressed concern regarding cooperation of patients and staff members to the implementation of an incremental hemodialysis program. Despite the identified barriers, 82% of participants agreed that incremental hemodialysis is feasible with their current resources (see Table 4). Chi-square analysis did not reveal differences in the perception of incremental hemodialysis feasibility based on the participant demographic characteristics (results not shown).
Feasibility and Potential Number of Patients to Benefit From Incremental Dialysis With Current Resources.
Discussion
This national survey of Canadian nephrologists indicates that the practice of incremental hemodialysis is widespread, but discretionary, with no systematic approach to assessment and monitoring. We identified that the 3 most common criteria used in the prescription of incremental hemodialysis are residual urine output, electrolyte homeostasis, and goals of care. No significant association was found between reimbursement model and prescription of incremental hemodialysis. For prescribers with a model available for incremental hemodialysis, an individualized approach was most used. In contrast, it was uncommon to start hemodialysis with reduced hours 3 times weekly or with once-weekly treatment. Significant concerns included patient safety, logistics of scheduling, lack of scientific evidence, and patient acceptance of dose escalation. However, most of the surveyed nephrologists felt that incremental hemodialysis can be safely prescribed.
Incremental dialysis, where the frequency and duration of dialysis sessions are individualized to account for RKF, has been discussed as a possible strategy to address the various patient- and system-related issues associated with conventional hemodialysis. 16 An opinion paper published in 2014 proposed 10 criteria for patient eligibility for incremental hemodialysis: RKF, manageable intradialytic weight gain, stable cardiovascular status, infrequent hospitalization, quality of life, small to normal body habitus, good nutritional status, and absence of hyperkalemia, hyperphosphatemia, and profound anemia. 17 A systematic review identified 15 observational studies comparing outcomes in patients receiving incremental hemodialysis with those receiving standard thrice-weekly treatment and found similar survival between groups, with greater preservation of RKF in those receiving incremental hemodialysis, deferring a requirement for a full dialysis dose by a mean of 12.1 months (95% confidence interval = 9.8-14.3). 18 In addition to preservation of RKF, incremental hemodialysis has been associated with shorter recovery time after dialysis treatment, similar or improved health-related quality of life, and fewer dialysis access-related complications.18,19 Although incremental hemodialysis has been endorsed by national and regional dialysis guidelines, little is published on its actual practice. In North America and Europe, approximately 4% of hemodialysis patients are on twice-weekly or less frequent hemodialysis.20,21 In non-Western countries, this number is considerable higher, up to 75% in areas like Sudan, which may largely be driven by resource limitations. 22 However, it should be noted that less frequent dialysis is not the same as incremental dialysis and it is not well known how many of these centers account for RKF when prescribing less frequent hemodialysis. Individual dialysis center experiences who have prescribed less frequent dialysis with monitoring of RKF have shown younger, less comorbid patients with Kt/Vurea of at least 1.6 tend to have similar survival outcomes as those prescribed thrice-weekly dialysis.23-25 Anecdotally, it is known that these centers have continued their practice of incremental dialysis, but there is limited information on how their programs have evolved over time. At this time, there is no clear consensus as to which patient and clinical factors should be taken into account when prescribing incremental dialysis. Randomized control trials currently in progress hope to address the efficacy of incremental dialysis.26,27
The results of this survey demonstrate broad agreement with previously identified clinical and patient factors, especially RKF, in prescribing incremental hemodialysis. Furthermore, we have shown there is a wide practice of incremental hemodialysis in Canada. For the first time, this survey has concretely identified barriers and concerns regarding the implementation of an incremental hemodialysis program. Development of clear eligibility and monitoring criteria, appropriate patient and provider education regarding treatment options, and a shared decision-making model in making dialysis treatment decisions should be considered in future development of incremental hemodialysis programs.
Limitations
The generalizability of our study is limited by the response rate of 35%. We acknowledge there is a likely bias and potential overestimation of frequency of the provision of incremental hemodialysis: participants who provide incremental dialysis may be more likely to complete a survey on the subject. However, this is a known issue with any elecAtronic survey and our response rate was comparable with the usual rates seen in electronic surveys. Many survey participants were from an academic setting, making the results less generalizable to the community setting.
Conclusions
Anecdotally, the use of incremental hemodialysis is known; however, there is a paucity of information on nephrologist opinions regarding and current practice of incremental hemodialysis. The results of this survey indicate that although the practice of incremental dialysis is widespread, there is a lack of standardization, resulting in a large variation in care. Going forward, efforts to implement an incremental hemodialysis program will need to address concerns regarding patient expectations regarding treatment, patient safety, and dialysis scheduling logistics.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581211065255 – Supplemental material for Knowledge and Practice of Incremental Hemodialysis: A Survey of Canadian Nephrologists
Supplemental material, sj-docx-1-cjk-10.1177_20543581211065255 for Knowledge and Practice of Incremental Hemodialysis: A Survey of Canadian Nephrologists by Anita Dahiya, Aminu Bello, Stephanie Thompson, Kara Schick-Makaroff and Neesh Pannu in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-docx-2-cjk-10.1177_20543581211065255 – Supplemental material for Knowledge and Practice of Incremental Hemodialysis: A Survey of Canadian Nephrologists
Supplemental material, sj-docx-2-cjk-10.1177_20543581211065255 for Knowledge and Practice of Incremental Hemodialysis: A Survey of Canadian Nephrologists by Anita Dahiya, Aminu Bello, Stephanie Thompson, Kara Schick-Makaroff and Neesh Pannu in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of Terry Smith for survey development and thank the CSN for deploying the survey to their members. The authors would like to thank the nephrologists who participated in the survey.
Ethics Approval and Consent to Participate
This study was approved by the Research Ethics Board at the University of Alberta (Pro00098076). Participation consent was obtained on initiation and completion of the electronic survey.
Author Contributions
Anita Dahiya, BSc, MD (1): conceptualization, data curation, formal analysis, writing—original draft, review, and editing; Aminu Bello, MD, PhD (2): conceptualization, methodology, writing—review and editing; Stephanie Thompson, MD, PhD (2): conceptualization, resources, writing—review and editing; Kara Schick-Makaroff, RN, BSc, MN, PhD (3): conceptualization, resources, writing—review and editing; Neesh Pannu, BSc, MD, SM (2): conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, supervision, writing—original draft, reviewing, and editing
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Kidney Health Section of the Medicine Strategic Clinical Network and the Canadian Society of Nephrology (CSN).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.