
Abstract
Background:
Quality indicators are required to identify gaps in care and to improve equitable access to kidney transplants. Referral to a transplant center for an evaluation is the first step toward receiving a kidney transplant, yet widespread reporting on this metric is lacking.
Objective:
The objective was to use administrative health care databases to examine multiple ways to define referral for a kidney transplant evaluation by varying clinical inclusion criteria, definitions for end of follow-up, and statistical methodologies.
Design:
This is a population-based cohort study.
Setting:
This study linked administrative health care databases in Ontario, Canada.
Patients:
Adults from Ontario, Canada, with advanced chronic kidney disease (CKD) between April 1, 2017, and March 31, 2018.
Measurements:
The primary outcome was the 1-year cumulative incidence of kidney transplant referral.
Methods:
We created several patient cohort definitions, varying patient transplant eligibility by health status (eg, whether patients had a recorded contraindication to transplant). We presented results by advanced CKD status (ie, patients approaching the need for dialysis vs receiving maintenance dialysis) and by method of cohort entry (ie, incident only vs prevalent and incident patients combined), resulting in 12 unique cohorts.
Results:
Sample size varied substantially from 414 to 4128 depending on the patient cohort definition, with the largest reduction in cohort size occurring when we restricted to a “healthy” (eg, no evidence of cardiovascular disease) group of patients. The 1-year cumulative incidence of transplant referral varied widely across cohorts. For example, in the incident maintenance dialysis population, the cumulative incidence varied more than 2-fold from 16.3% (95% confidence interval [CI] = 15.0%-17.7%) using our most inclusive cohort definition to 40.0% (95% CI = 36.0%-44.5%) using our most restrictive “healthy” cohort of patients.
Limitations:
Administrative data may have misclassified individuals’ eligibility for kidney transplant.
Conclusions:
These results can be used by jurisdictions to measure transplant referral, a necessary step in kidney transplantation that is not equitable for all patients. Adoption of these indicators should drive quality improvement efforts that increase the number of patients referred for transplantation and ensure equitable access for all patient groups.
Introduction
Compared with dialysis, a kidney transplant offers patients a longer and better quality of life.1,2 Unfortunately, many barriers impede patients’ access to transplant.3-7 One barrier is a lack of transparency and accountability for ensuring timely and equitable access to transplant. 8 Quality indicators in kidney transplantation are needed to identify care gaps and to monitor improvement. 9 However, transplant quality indicators have typically focused on downstream metrics (eg, patient survival) instead of upstream events (eg, transplant referral), with the latter providing insight into access to kidney transplant. 10 Unintended consequences associated with post-transplant outcome metrics have led to calls to reform kidney transplant quality indicators to include measures of transplant access.9,11-16
One of the first steps in receiving a kidney transplant is a referral to a transplant center for an evaluation. However, measurement of this crucial step is rarely reported. Despite data showing substantial geographic variability and inequities in kidney transplant referral,16-17 most jurisdictions, including the United States and Canada, do not mandate reporting of any indicator relating to referral for transplantation.12,18,19
No accepted metric captures the process of transplant referral for patients with kidney failure. Developing a quality indicator requires careful consideration of the methodology selected 20 which includes defining the cohort of interest (eg, restricting to transplant eligible patients), censoring events (eg, stopping follow-up when a patient is no longer transplant eligible), and statistical methodologies (eg, accounting for the competing risk of death). In previous work examining pre-emptive kidney transplantation as a quality indicator, we found that varying the inclusion criteria (eg, including all patients approaching the need for dialysis vs excluding those with a contraindication to transplantation) resulted in a wide variation in the incidence of kidney transplantation from 1.02 to 2.21 per 100 person-years. 21
Using administrative health care databases, we developed different measures of referral for a kidney transplant evaluation by varying clinical inclusion criteria, definitions for end of follow-up, and statistical methodologies.
Methods
Study Overview
We conducted a population-based cohort study to identify adults from Ontario, Canada, with advanced chronic kidney disease (CKD) between April 1, 2017, and March 31, 2018. This time frame was selected to represent a fiscal year based on data availability at the time of analysis. We created 12 patient cohorts by varying the following parameters: (1) level of kidney function (ie, patients approaching the need for dialysis or receiving maintenance dialysis); (2) presence or absence of a recorded contraindication to transplant; (3) whether patients met a prespecified “healthy” definition (described in Table 1 below); and (4) type of cohort entry (incident vs prevalent). All individuals in this study would have been under the care of a nephrologist, with patients approaching the need for dialysis receiving their care at one of Ontario’s multidisciplinary CKD clinics.
Description of the Inclusion and Exclusion Criteria Across Cohort Definitions.
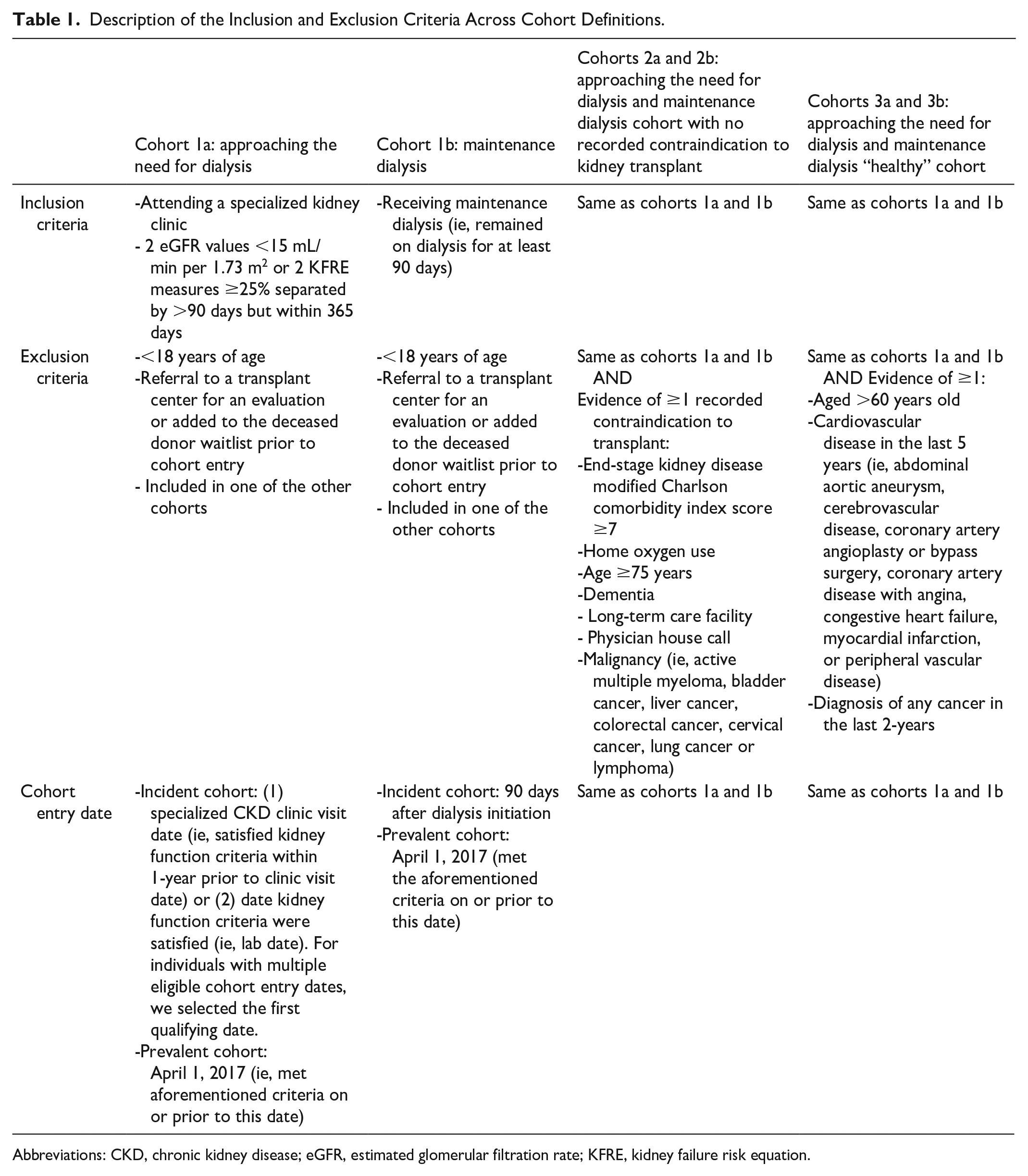
Abbreviations: CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; KFRE, kidney failure risk equation.
Design and Setting
We used administrative health care databases from Ontario, Canada, held at ICES (ices.on.ca/). ICES is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. These data sets were linked using unique encoded identifiers and analyzed at ICES Western. The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board. To report this study, we used the Reporting of studies Conducted using Observational Routinely-collected health Data (RECORD) Statement (Supplementary Table 1).
Database Sources
We used several linked administrative databases, including the Ontario Renal Reporting System to identify specialized kidney clinic visits and to identify patients receiving maintenance dialysis. We applied the 2021 CKD-EPI creatinine equation without race to calculate the estimated glomerular filtration rate (eGFR) with serum creatinine captured from the Ontario Laboratories Information System (OLIS). 22 We combined eGFR and the urine albumin-to-creatinine ratio from OLIS to calculate the 2-year probability of kidney failure using the kidney failure risk equation (KFRE). 23 To capture kidney transplant referrals, we used data from the Trillium Gift of Life Network-Ontario Health, the agency responsible for coordinating organ and tissue donation and transplantation services across the province of Ontario. Supplementary Table 2 provides further details on the databases and coding definitions used.
Cohort Definitions
We included both prevalent (ie, entered the cohort on April 1, 2017) and incident patients (ie, entered the cohort between April 2, 2017, and March 31, 2018). We presented data using incident patients alone as well as a combined cohort of incident and prevalent patients. We allowed individuals to be included in more than 1 cohort (ie, cohorts were not mutually exclusive). Cohort definitions are detailed in the following sections and in Table 1.
Cohort 1a: Approaching the Need for Dialysis
We included adults (ie, aged ≥ 18 years) who attended a specialized kidney clinic in Ontario and satisfied at least one of the following kidney function criteria: (1) 2 outpatient eGFR values <15 mL/min per 1.73 m2 or (2) two, 2-year KFRE measures ≥25%. To ensure stability of kidney function, the 2 measures had to be separated by at least 90 days but no more than 12 months. We excluded individuals who received a kidney transplant referral prior to cohort entry.
Cohort 1b: Maintenance Dialysis
We included adults (ie, aged ≥ 18 years) receiving maintenance dialysis (in-center or at home). We required all individuals to receive dialysis for at least 90 days to ensure we were not capturing patients receiving acute dialysis and excluded individuals who received a kidney transplant referral prior to cohort entry.
Cohorts 2a and 2b: Advanced Chronic Kidney Disease With No Recorded Contraindication to Kidney Transplant
In addition to the inclusion and exclusion criteria for cohorts 1a and 1b, we created a cohort of individuals who had no recorded contraindication to kidney transplant. For this cohort, patients were excluded if one or more of the following was present: age >75 years old, end-stage kidney disease (ESKD) modified Charlson comorbidity index score ≥7, home oxygen use, dementia, residence at a long-term care facility, received at least 1 physician house call in the past year, and select malignancies. This definition was based on our previous work which found 97% of individuals with at least one of these characteristics never received a kidney transplant during follow-up. 24
Cohorts 3a and 3b: Advanced Chronic Kidney Disease and “Healthy”
In addition to the inclusion and exclusion criteria for cohorts 1a and 1b, we further restricted our cohort, creating a “healthy” cohort of individuals. We included only individuals who were 18 to 60 years old without a diagnosis of cardiovascular disease or cancer. We recognize that this is a strict definition, but we included this cohort as virtually all patients meeting these criteria should be referred for transplantation. We have used a similar definition in our previous work. 25
Kidney Transplant Referral
Our primary outcome was referral to a kidney transplant center for an evaluation (ie, kidney transplant referral) within 1-year of cohort entry. We also examined referrals occurring within 2- and 3 years of cohort entry. We included referral for both kidney-only and kidney combination transplants (eg, kidney-pancreas). Although there is no established benchmark for a timely referral, most clinicians agree that referrals should be made within 1-year of meeting the referral eligibility criteria. In Ontario, Canada, patients are eligible for transplant referral with an eGFR <15 mL/min/1.73 m2 or a 2-year KFRE ≥25% or when maintenance dialysis is initiated; they also must have no absolute contraindications to kidney transplant (eg, no active malignancy). 26
In the province of Ontario, physicians in the CKD programs are responsible for sending referrals to 1 of 6 transplant centers. Unlike in the United States, patient self-referral for transplantation is not permitted. 27
End of Follow-up Events
For cohorts 1 and 3, we stopped following individuals at death and end of follow-up. We stopped follow-up in the cohort of patients approaching the need for dialysis when they initiated maintenance dialysis; once these individuals started dialysis, they contributed person-time to the maintenance dialysis cohort. For cohort 2 (ie, no recorded contraindications to transplant), we stopped following individuals at death, end of follow-up, or if a patient developed a recorded contraindication to transplant (individuals who became older than age 75 years during follow-up remained in the study). We also stopped following individuals at the maximum follow-up, which for the incident cohort was March 31, 2019, March 31, 2020, or March 31, 2021, when estimating the 1-, 2-, and 3-year cumulative incidence of referral, respectively. When examining the combined incident and prevalent population cohorts, the end of follow-up was the same as the end of accrual period, with a follow-up from April 1, 2017, to March 31, 2018.
Statistical Analysis
For baseline characteristics, we used medians (25th, 75th percentiles) for continuous variables and frequencies (proportions) for categorical variables. We calculated the cumulative incidence of transplant referral (95% confidence interval) using the nonparametric Aalen-Johansen estimator of cumulative incidence function (CIF) to account for the competing risk of death and in the approaching the need for dialysis cohort, the competing risk of initiating maintenance dialysis. 28 The literature suggests using the CIF when the risk of the competing event is high to avoid potentially overestimating the cumulative incidence which may occur with more traditional methods such as the Kaplan-Meier estimator.28,29 To understand how the estimates were affected by using more traditional methods (ie, Kaplan-Meier estimator), we also calculated the cumulative probability of transplant referral.
Similar to the incident cohort, when we examined the combined incident/prevalent cohort, we reported the cumulative incidence of referral using the CIF. However, at cohort entry, the prevalent patients had delayed/staggered entries as a function of their disease onset. Thus, we adopted a left-truncated and right-censored (LTRC) approach, where the risk set for the Aalen-Johansen estimator naturally accounts for both left-truncation and right-censoring. 30 This type of analysis is also known as period analysis, which is commonly used in the cancer literature.31,32 The estimated cumulative incidence in this analysis reflects a projection of referral activity on a hypothetical population. Supplementary Table 3 provides a summary of the traditional methodology used in our incident population vs the LTRC approach used in our combined incident and prevalent population.
Our data were largely complete except for the following baseline variables: rural residence (<1% missing with urban residence imputed), income quintile (<1% missing with income quintile 3 imputed), and KFRE (≤1.5% missing in the approaching the need for dialysis cohort and kept the missing category). Our capture of referral to a transplant center for an evaluation was largely complete, with our previous work demonstrating 1.35% of patients had a missing referral date (ie, patient had evidence of being placed on the transplant waitlist or received a kidney transplant, but there was no evidence of a referral date). 33 We have previously described our handling of missing transplant referral data. 33
Confidence interval widths were not adjusted for multiple testing. We conducted all analyses using the SAS version 9.4 (SAS Institute, Cary, North Carolina).
Additional Analyses
In our prespecified subgroup analyses, we presented the results by age (<65 vs ≥65 years old) and sex (male vs female) for cohort 1.
Results
Approaching the Need for Dialysis Cohorts
We included 8204 individuals approaching the need for dialysis in our most inclusive cohort (cohort 1a), 4637 individuals after restricting to individuals with no recorded contraindications to kidney transplant (cohort 2a), and 1313 patients after further restricting to a “healthy” cohort (cohort 3a).
Maintenance Dialysis Cohorts
In our most inclusive cohort, we included 9700 individuals receiving maintenance dialysis (cohort 1b), with 1090 of these individuals originally in the cohort of patients approaching the need for dialysis but started maintenance dialysis during the accrual window. After restricting to individuals with no recorded contraindications to kidney transplant our cohort size decreased to 4906 individuals (cohort 2b), with 633 of these individuals originally in the approaching the need for dialysis cohort. Restricting to a “healthy” cohort resulted, in 1069 individuals (cohort 3b), with 174 of these individuals originally in the approaching the need for dialysis cohort. The flow diagram for all cohorts is provided in Supplementary Figures 1a-1l.
Baseline Characteristics
Baseline characteristics are presented for the approaching the need for dialysis cohorts in Table 2 and for the maintenance dialysis cohorts in Table 3. In the maintenance dialysis cohorts, the median age was the highest in Cohort 1b (71 years [only cohort to include individuals >75 years]) and the lowest in Cohort 3b (48 years; excluded individuals >60 years). Our most inclusive cohort (ie, Cohort 1b) had the highest proportion of individuals with comorbid conditions whereas cohort 3b (ie, healthy cohort) had the lowest proportion of individuals with comorbid conditions. For example, in the maintenance dialysis population, cohort 1b had 7.2% of individuals residing in a long-term care home and 72.3% with cardiovascular disease compared to 1.6 and 0%, in cohort 3b, respectively.
Baseline Characteristics for Patients in the Combined Incident/Prevalent Approaching the Need for Dialysis Cohort, Presented by 3 Cohort Definitions.

Data are presented as n (%) or median (25th, 75th percentile).
Cohort 1a: Incident and prevalent patients approaching the need for dialysis.
Cohort 2a: Incident and prevalent patients approaching the need for dialysis with no recorded contraindication to kidney transplant.
Cohort 3a: Incident and prevalent patients approaching the need for dialysis and considered “healthy.”
Income quintile is constructed using neighborhood-level income. Missing data were imputed into category 3 (<0.5% of individuals had missing data).
Missing data were imputed into urban (<0.5% of individuals had missing data).
Outpatient estimated glomerular filtration rate within 1 year of the cohort entry date (if multiple values the most recent one was selected).
Outpatient estimated 2-year risk of kidney failure within 1-year of the cohort entry date (if multiple values the most recent one was selected). This information was missing in <1.5% of individuals across cohort definitions.
A higher ESKD-modified Charlson Comorbidity Index score indicates greater comorbidity.
Malignancy defined as active multiple myeloma, bladder cancer, liver cancer, colorectal cancer, cervical cancer, lung cancer, or lymphoma in the last 5 years except liver cancer which was defined as a diagnosis any time prior to cohort entry.
Cardiovascular disease was defined as abdominal aortic aneurysm, cerebrovascular disease, coronary artery angioplasty or bypass surgery, coronary artery disease with angina, congestive heart failure, myocardial infarction, or peripheral vascular disease. We looked back 5 years for all of the aforementioned conditions except for congestive heart failure which we looked back to the beginning of data availability.
Malignancy in the last 2 years includes any cancer type recorded in the Ontario Cancer Registry.
In accordance with ICES privacy policies, cell sizes less than or equal to 5 cannot be reported.
We did not report this information as both myocardial infarction and stroke/transient ischemic attack were exclusion criteria in the cohort creation. The baseline characteristic definition of myocardial infarction and stroke/transient ischemic attack are slightly different than the exclusion criteria so there could be some individuals who had these characteristics.
Although cohort 3 excluded individuals with a malignancy in the last 2 years, the definitions of malignancy between cohorts 2 and 3 were slightly different resulting in some individuals (n = 9) having malignancy according to the definition used in cohort 2.
Although cohort 2 excluded individuals with a malignancy, the definitions of malignancy between cohorts 2 and 3 were slightly different resulting in some individuals (n = 92) having malignancy in the last 2 years, according to the definition used in cohort 3.
Baseline Characteristics for Patients in the Combined Incident/Prevalent Maintenance Dialysis Cohort, Presented by 3 Cohort Definitions.
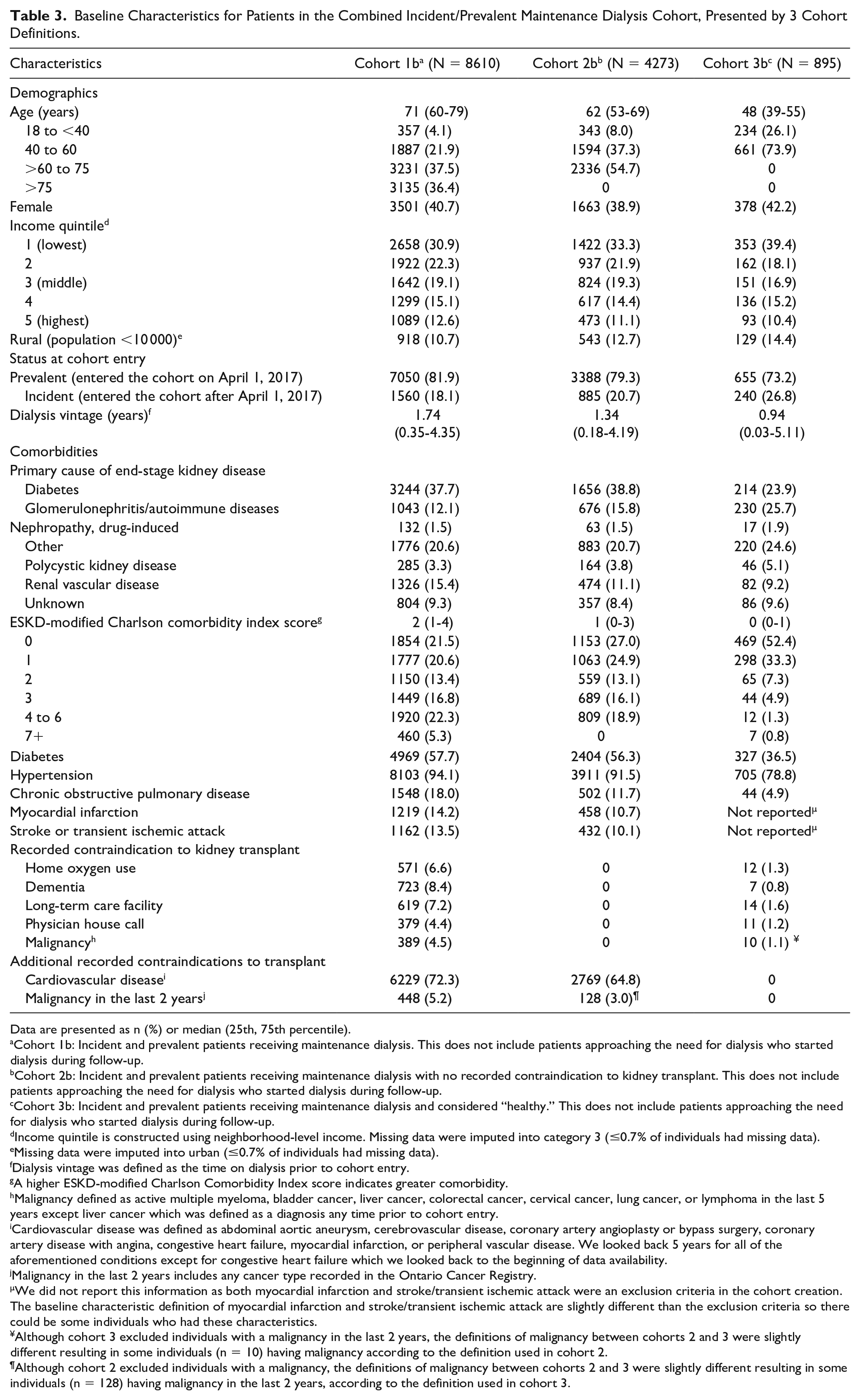
Data are presented as n (%) or median (25th, 75th percentile).
Cohort 1b: Incident and prevalent patients receiving maintenance dialysis. This does not include patients approaching the need for dialysis who started dialysis during follow-up.
Cohort 2b: Incident and prevalent patients receiving maintenance dialysis with no recorded contraindication to kidney transplant. This does not include patients approaching the need for dialysis who started dialysis during follow-up.
Cohort 3b: Incident and prevalent patients receiving maintenance dialysis and considered “healthy.” This does not include patients approaching the need for dialysis who started dialysis during follow-up.
Income quintile is constructed using neighborhood-level income. Missing data were imputed into category 3 (≤0.7% of individuals had missing data).
Missing data were imputed into urban (≤0.7% of individuals had missing data).
Dialysis vintage was defined as the time on dialysis prior to cohort entry.
A higher ESKD-modified Charlson Comorbidity Index score indicates greater comorbidity.
Malignancy defined as active multiple myeloma, bladder cancer, liver cancer, colorectal cancer, cervical cancer, lung cancer, or lymphoma in the last 5 years except liver cancer which was defined as a diagnosis any time prior to cohort entry.
Cardiovascular disease was defined as abdominal aortic aneurysm, cerebrovascular disease, coronary artery angioplasty or bypass surgery, coronary artery disease with angina, congestive heart failure, myocardial infarction, or peripheral vascular disease. We looked back 5 years for all of the aforementioned conditions except for congestive heart failure which we looked back to the beginning of data availability.
Malignancy in the last 2 years includes any cancer type recorded in the Ontario Cancer Registry.
We did not report this information as both myocardial infarction and stroke/transient ischemic attack were an exclusion criteria in the cohort creation. The baseline characteristic definition of myocardial infarction and stroke/transient ischemic attack are slightly different than the exclusion criteria so there could be some individuals who had these characteristics.
Although cohort 3 excluded individuals with a malignancy in the last 2 years, the definitions of malignancy between cohorts 2 and 3 were slightly different resulting in some individuals (n = 10) having malignancy according to the definition used in cohort 2.
Although cohort 2 excluded individuals with a malignancy, the definitions of malignancy between cohorts 2 and 3 were slightly different resulting in some individuals (n = 128) having malignancy in the last 2 years, according to the definition used in cohort 3.
Cumulative Incidence of Kidney Transplant Referral
Approaching the need for dialysis
The 1-year cumulative incidence of kidney transplant referral in the incident cohort of patients approaching the need for dialysis varied more than 3-fold across definitions, with estimates of 6.1% (95% CI = 5.5%-6.8%), 10.4% (95% CI = 9.4%-11.6%), and 20.7% (95% CI = 17.8%-20.4%), for the most inclusive (cohort 1a), the no recorded contraindications to transplant cohort (cohort 2a), and the most restrictive “healthy” cohort (cohort 3a), respectively (Figure 1). Similar variability was observed when examining the combined incident and prevalent cohort and when examining the 2- and 3-year cumulative incidence (Table 4).
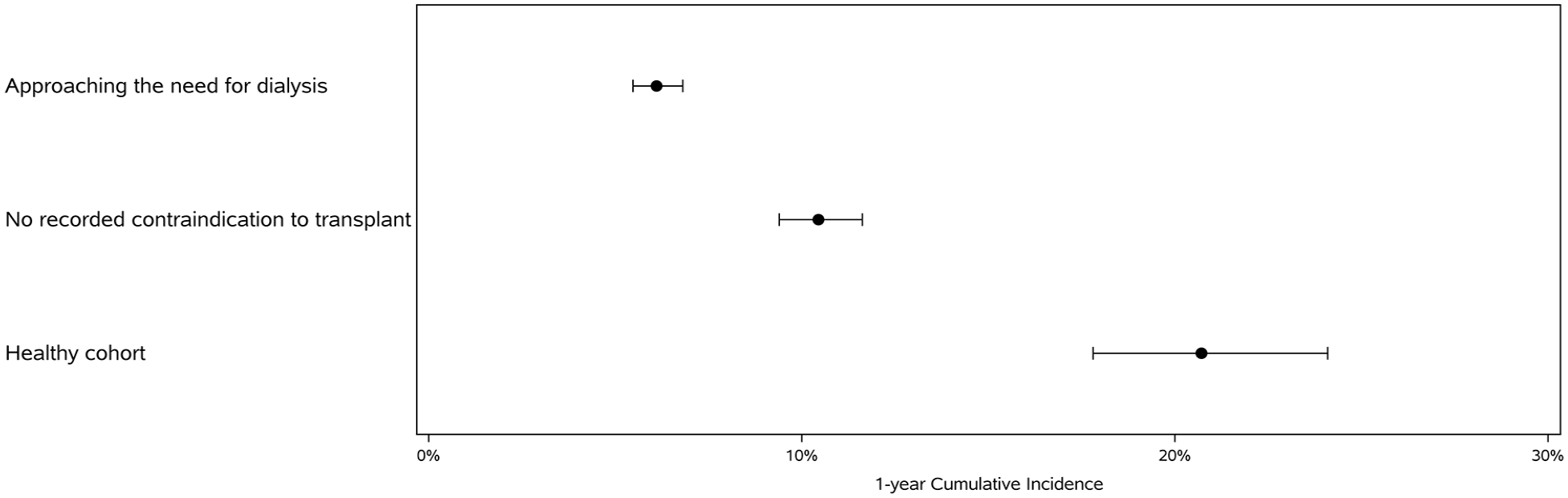
The 1-year cumulative incidence of kidney transplant referral in the incident cohort of patients approaching the need for dialysis, including the most inclusive (cohort 1a), the no recorded contraindications to transplant cohort (cohort 2a) and the most restrictive “healthy” cohort (cohort 3a).
1-, 2-, and 3-Year Cumulative Incidence of Referral to a Transplant Center for an Evaluation, Presented Across Cohorts.

Abbreviations: CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; KFRE, kidney failure risk equation.
Represents the number of transplant referral events for 1 year of follow-up (incident cohorts) and for the combined incident and prevalent cohorts it represents the number of events during the 1-year accrual window.
Maintenance dialysis
The 1-year cumulative incidence of referral in the incident maintenance dialysis cohort varied more than 2-fold across definitions, with estimates of 16.3% (95% CI = 15.0%-17.7%), 27.1% (24.9%-29.5%), and 40.0% (95% CI = 36.0%-44.5%) (Figure 2), for the most inclusive (cohort 1b), the no recorded contraindications to transplant cohort (cohort 2b) and the most restrictive “healthy” cohort (cohort 3b), respectively (Table 4). Similar variability was observed when examining the combined incident and prevalent cohort and when examining the 2- and 3-year cumulative incidence (Table 4). The cumulative incidence of referral was consistently higher in the maintenance dialysis cohort compared to the approaching the need for dialysis cohort.

The 1-year cumulative incidence of referral in the incident maintenance dialysis cohort including the most inclusive (cohort 1b), the no recorded contraindications to transplant cohort (cohort 2b), and the most restrictive “healthy” cohort (cohort 3b).
In both the approaching the need for dialysis and the maintenance dialysis cohorts, the absolute number of referrals generally decreased as we used more restrictive denominators. For example, the number of transplant referrals in the incident maintenance dialysis cohort decreased from 431 in our most inclusive cohort to 166 referrals in our most restrictive “healthy” cohort.
For both the approaching the need for dialysis cohort and maintenance dialysis cohort, the Kaplan-Meier estimator always resulted in a higher cumulative probability of referral compared to when using the CIF (Supplementary Tables 4a-c).
End of Follow-up Events
We found that the end of follow-up events varied considerably depending on the cohort definition used. For example, in the “healthy” cohort, 1.8% of patients receiving dialysis died during follow-up vs 12.8% in our most inclusive cohort (Supplementary Table 5).
Additional Analyses
In both the approaching the need for dialysis and maintenance dialysis incident cohorts, individuals aged ≥65 years had a substantially lower incidence of transplant referral at 1 year compared to individuals aged <65 years (Table 5). When examining sex, females had a slightly lower cumulative incidence of kidney transplant referral compared to males.
1-Year Cumulative Incidence of Referral to a Transplant Center for an Evaluation, Presented by Age and Sex.

Cohort 1a (incident): Approaching the need for dialysis (eGFR <15 mL/min per 1.73 m2 or 2-year KFRE measures ≥25%).
Cohort 1b (incident): Maintenance dialysis.
Discussion
Using administrative health care databases, we explored different cohort definitions, methods, and end of follow-up definitions to measure the cumulative incidence of kidney transplant referral. We found that the cumulative incidence of transplant referral varied widely across cohort definitions, with the 1-year cumulative incidence varying more than 2-fold from 16.3% to 40.0% in the maintenance dialysis population. Our definitions for kidney transplant referral can be used to monitor and improve access to kidney transplant in CKD clinics and dialysis centers. This research highlights the importance of exploring different definitions to select a quality indicator that is most appropriate from the patient’s perspective as well as the health care system.
We found that the cohort size and resulting cumulative incidence of referral changed considerably across cohort definitions, with the most substantial change occurring when we restricted to a “healthy” cohort. For example, our cohort size was reduced by 84%, from 2650 to 414 incident patients receiving maintenance dialysis, after restricting to a “healthy” (eg, no evidence of cardiovascular disease) cohort of patients, and the 1-year cumulative of transplant referral changed from 16.3% to 40.0%. Changes in the cumulative incidence of referral occurred to a lesser degree when using different methodology (Kaplan-Meier vs CIF) and when including incident vs incident and prevalent patients.
There are several criteria to consider when selecting a quality indicator, including importance, measurability, actionability, evidence-based, feasibility, interpretability, and data quality. 34 The optimal definition of kidney transplant referral will likely vary by jurisdiction depending on data availability (ie, feasibility and data quality) and the intended use of the indicator. For example, cohort 1 is the easiest to adopt as it has the fewest number of exclusions; however, many of the patients in this cohort will never be eligible for transplant which can complicate the interpretation of the metric. In our jurisdiction, in addition to including patients receiving maintenance dialysis, it was important to include patients approaching the need for dialysis, given a provincial priority to increase pre-emptive kidney transplants. However, some jurisdictions may not have access to lab data to define kidney function. Future studies may want to explore an alternative definition of kidney transplant referral for patients approaching the need for dialysis which requires these patients to also have a potential living donor. Unless it is expected that the patient will require dialysis within the next year, Ontario guidance is that the patient should only be referred if they have a potential living donor. 35 It is important to recognize that the creation of quality indicators is a dynamic process for which modifications will need to be made based on factors such as user feedback, updated clinical guidelines and newly available data. 36
Another important consideration when selecting a quality indicator is an understanding of potential unintended consequences. For example, while increasing kidney transplant referrals is a laudable goal, we would not want to increase the number of inappropriate referrals (eg, increasing referrals in patients who would not be healthy enough to be placed on the waitlist). Therefore, it is important to have balancing measures, such as measuring the proportion of patients referred for kidney transplant who are placed on the transplant waitlist. With transplant referrals, there is the added nuance of no national benchmark for their optimal timing; referring a patient too early may result in increased testing on the waitlist, whereas a referral too late may result in a missed opportunity for a pre-emptive kidney transplant.
Although the goal of this work was not to endorse a specific definition, the results of this work have provided us with insights on how we might want to report kidney transplant referral in Ontario. First, we would present the transplant referral metric using 2 different cohorts. One metric including all individuals and a second restricted to a transplant eligible cohort; we found that the absolute number of referrals decreased as we used more restrictive cohort definitions. Therefore, employing 2 cohort definitions will help ensure we are capturing all referrals in Ontario. Second, it is important to present the results separately for patients approaching the need for dialysis vs patients receiving maintenance dialysis, given that the staff and clinic/unit caring for these populations are usually not the same. Last, we would likely present results using the combined incident/prevalent cohort given that it had more events, captured the complete population, and the results were similar to the incident cohort.
Regardless of the definition used in our study, the cumulative incidence of kidney transplant referral was low. Even using our most restrictive “healthy” cohort definition, we found that only 55% of patients receiving maintenance dialysis were referred for a transplant over 3 years. We thought that given the relative health in this cohort, the number of individuals referred would be closer to 100%. Potential reasons for the healthy cohort referrals being substantially lower than 100%, include we could not examine patient preference for transplant, our administrative databases cannot capture all the complexities of transplant eligibility (ie, healthy cohort likely included some individuals with medical contraindications to transplant), lack of patient education on the potential benefits of a transplant compared to dialysis, and provider knowledge about transplant. This work highlights the need to understand barriers to referral, to regularly report on transplant referral to monitor improvements, to establish national referral benchmarks, and the need for interventions and policy changes to improve referrals.13,37 Other jurisdictions have found similar results with a study conducted in Georgia, United States, finding the 1-year cumulative incidence of referral in patients aged 18 to 70 years receiving dialysis was 24%. 16 Similarly, Kim et al 38 found that only 17% of Canadian patients receiving maintenance dialysis were referred for transplant within 1 year.
In addition to there being multiple ways of defining the cohort, considerations for subgroup reporting are also crucial to understand equity in access to kidney transplant. 39 Some important equity measures to consider include age, sex, race, geographic location, and socioeconomic status. Similar to previous work,40,41 we found that females had a lower cumulative incidence of referral compared to males. Potential reasons include physicians may view women as frailer, providers may be less likely to discuss transplant as a treatment option, female’s attitudes toward transplant, concerns about being a care burden, and lower self-advocacy.40,41 We also found older individuals were substantially less likely to be referred for kidney transplant.
Our study has several limitations. First, we conducted this study using data that was several years old. However, we do not anticipate that having more recent data would change our conclusions. Second, we tried to emulate transplant eligibility using cohort definitions based on administrative data, which may have misclassified individuals’ eligibility for kidney transplant. Third, we did not adjust for patient characteristics, using a metric such as the standardized referral ratio. 42 We opted to use restriction to account for patient characteristics. Last, regions outside of Ontario may find it difficult to implement some of our cohort definitions due to a lack of available data.
In conclusion, our study demonstrates the importance of considering multiple ways to define patient cohorts when developing an indicator for quality measurement. The results from this study can be used by jurisdictions to implement a metric that appropriately measures the process of referral for transplantation, a necessary step that is not equitable for all patients. Ultimately, the adoption of a referral indicator worldwide should drive quality improvement processes that increase the absolute numbers of patients referred for transplantation as well as ensure equitable access for all patient groups.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251317009 – Supplemental material for Defining Referral for a Kidney Transplant Evaluation as a Quality Indicator: A Population-Based Cohort Study
Supplemental material, sj-docx-1-cjk-10.1177_20543581251317009 for Defining Referral for a Kidney Transplant Evaluation as a Quality Indicator: A Population-Based Cohort Study by Kyla L. Naylor, S. Joseph Kim, Bin Luo, Carol Wang, Amit X. Garg, Seychelle Yohanna, Darin Treleaven, Susan McKenzie, Jane Ip, Rebecca Cooper, Nadiyah Rehman and Gregory Knoll in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
Dr K.L.N. is supported by a Health System Impact Embedded Early Career Researcher Award Canadian Institutes of Health Research. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). The study was completed at the ICES Western site. This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from Canada Post Corporation and Statistics Canada. Parts of this material are based on data and/or information compiled and provided by: MOH, Canadian Institute for Health Information (CIHI), and Ontario Health. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. The authors acknowledge that the data used in this study were provided by the Trillium Gift of Life Network (Ontario Health), [2018], Toronto Ontario. The researcher’s interpretations and statements in this publication are those of the researcher only and not those of Trillium Gift of Life Network (Ontario Health).
Ethics Approval and Consent to Participate
ICES is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board.
Consent for Publication
Consent for publication was obtained from all authors.
Availability of Data and Materials
The data set from this study is held securely in coded form at ICES. Although legal data sharing agreements between ICES and data providers (eg, health care organizations and government) prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at ![]() (email:
(email:
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.