
Abstract
Background:
Acute kidney injury (AKI) is a frequent complication associated with severe COVID-19 and has been linked to increased mortality. While vaccination against SARS-CoV-2 has shown effectiveness in reducing severe COVID-19 outcomes, its impact on the development of AKI among hospitalized patients remains unclear.
Objective:
To evaluate the effect of SARS-CoV-2 vaccination on the incidence and severity of AKI and 28-day mortality among hospitalized patients with severe COVID-19.
Design:
Retrospective case-control study.
Setting:
Conducted at the Internal Medicine Department of Hospital General Dr. Manuel Gea González, Mexico, from April 2020 to December 2021.
Patients:
413 patients over 18 with confirmed severe COVID-19 were included. Patients were categorized based on their vaccination status before COVID-19 infection.
Measurements:
Key outcomes included the incidence of AKI, progression to AKI stage 3, and 28-day mortality. AKI was defined according to the KDIGO criteria.
Methods:
Data were analyzed using univariate and logistic regression models to assess the association between vaccination status and the studied outcomes. Covariates included age, sex, BMI, type 2 diabetes, hypertension, and inflammatory markers.
Results:
Among the 413 patients, 70% developed AKI, with a median hospital stay of 10 days (range 6-17). Vaccinated patients had a significantly lower incidence of AKI compared with nonvaccinated patients (48.7% vs 74.9%; P < .001). After adjusting for confounding factors, vaccination was associated with lower odds of AKI (OR: 0.252, 95% CI: 0.140-0.452), AKI stage 3 (OR: 0.448, 95% CI: 0.205-0.981), and 28-day mortality (OR: 0.187, 95% CI: 0.064-0.544).
Limitations:
As a single-center retrospective study, generalizability is limited. In addition, vaccination data were obtained from medical records, and the completeness of vaccination could not be independently verified.
Conclusions:
SARS-CoV-2 vaccination was independently associated with a reduced risk of AKI, AKI stage 3, and 28-day mortality in hospitalized patients with severe COVID-19. These findings highlight the potential protective effects of vaccination against severe kidney complications in this population.
Introduction
The COVID-19 pandemic has presented unprecedented global health challenges, resulting in over 800 million infections and 7 million deaths worldwide despite widespread vaccination efforts.1,2 Vaccines have shown significant real-world effectiveness in reducing the rates of SARS-CoV-2 infection, hospitalization, and mortality. 1 As the pandemic continues to evolve and transition to an endemic state, 3 it is important to understand the vaccine’s impact on specific complications, such as acute kidney injury (AKI). AKI is a severe complication of COVID-19 that is linked to increased in-hospital mortality, prolonged hospitalization, and the need for kidney replacement therapy (KRT).4-6 Given the significant health risks associated with AKI in severe COVID-19 cases, it is crucial to investigate whether vaccination provides protective benefits against this complication.
Prior studies have extensively documented the overall efficacy of COVID-19 vaccines in reducing severe outcomes like hospitalization and death. 1 However, the mechanisms of COVID-19-induced AKI are complex, involving acute tubular necrosis, collapsing glomerulopathy, and mitochondrial impairment due to direct viral damage and the cytokine storm. 4 ,7-9 While some research has explored the general complications of COVID-19 on kidney function, there is a lack of comprehensive studies analyzing the specific effects of vaccination on the incidence and severity of AKI in patients with severe COVID-19. This gap in knowledge leaves clinicians and policymakers uncertain about the potential kidney protective benefits of vaccination.
The primary objective of this study is to describe the frequency and characteristics of AKI in hospitalized patients with severe COVID-19 who have received at least 1 dose of the SARS-CoV-2 vaccine. It is hypothesized that immunization against SARS-CoV-2 is associated with a lower incidence of AKI, reduced progression to AKI stage 3, and decreased 28-day mortality. The secondary aim is to evaluate whether vaccination independently reduces these adverse outcomes when adjusted for clinical and biochemical confounders, such as age, comorbidities, and inflammatory markers. Using a case-control design, the study aims to provide evidence that could support the role of vaccination in protecting against severe renal complications in patients with COVID-19.
Material and Methods
Participants
A retrospective observational study was performed using medical files from patients hospitalized at the Internal Medicine department of the Hospital General Dr. Manuel Gea Gonzalez (HGDMGG) from April 2020 to December 2021. We report our findings following the STROBE guidelines for case-control studies. The patient inclusion criteria were age >18 years, confirmed SARS-CoV-2 infection through a positive polymerase chain reaction testing, hospitalization at the emergency department less than 24 hours, and patients with 30-day follow-up. Severe COVID-19 infection was defined as clinical signs of dyspnea, respiratory frequency over 30/min, oxygen saturation less than 93%, arterial oxygen partial pressure/fractional inspired oxygen (PaO2/FiO2) ratio less than 300, and lung infiltrates more than 50% of the lung field within 24 to 48 hours. 10 Likewise, AKI was defined according to KDIGO criteria as follows: stage 1, as an increase in serum creatinine level by 0.3 mg/dL within 48 hours or 1.5 to 1.9 times increase in serum creatinine level from baseline within 7 days; stage 2, as 2 to 2.9 times increase in serum creatinine level within 7 days; and stage 3, as 3 or more times increase in serum creatinine level within 7 days or initiation of dialysis. 5 The exclusion criteria included incomplete 30-day follow-up and loss of variables of interest (i.e., creatinine serum levels and AKI stage). Baseline kidney function was determined using the most recent outpatient serum creatinine measurement within the past 3 months for patients with prior follow-up or the first serum creatinine measurement at emergency department admission for those without recent outpatient data.
Overall, records from 1057 hospitalized patients with COVID-19 diagnosis were analyzed. Of them, 644 patients were excluded due to missing data. A flow diagram of the patient selection process is presented in Figure 1. This study was approved by the HGDMGG Research Committee and Research Ethics Committee (REF 14-17-2022), and patient anonymity was guaranteed according to the 1975 Declaration of Helsinki. Upon medical admission, the patient or a family member signed an informed consent form permitting the use of his/her medical file information for didactic, research, and publication purposes.
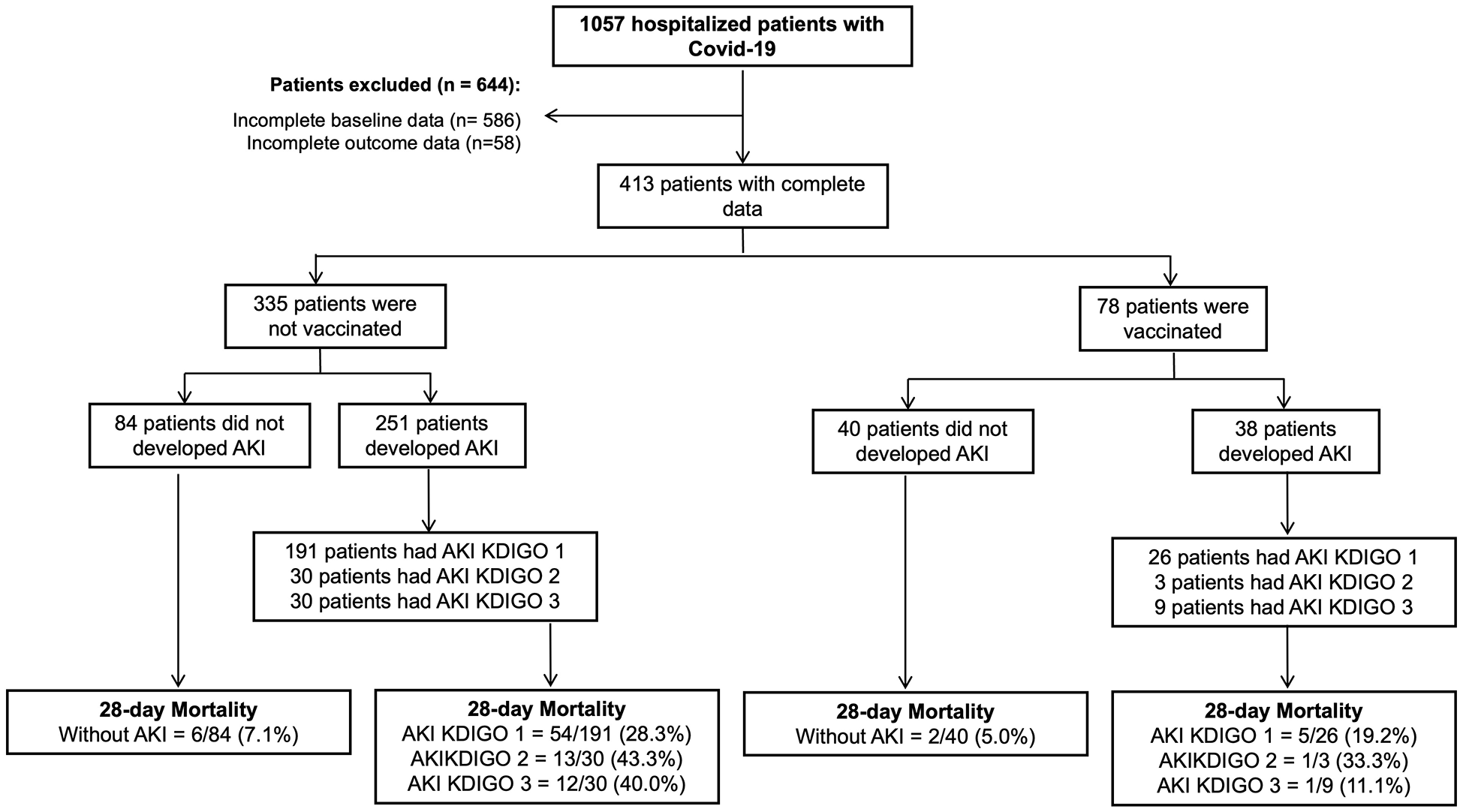
Patient selection flow diagram.
Clinical and biochemical data were obtained at admission. The body mass index (BMI) was calculated as the basal weight in kilograms (kg) divided by the square of body height in meters (m2); average weight was defined as <25 kg/m2, overweight as BMI between 25 and 29.9 kg/m2, and obesity as BMI ≥ 30 kg/m2. Hypertension was defined as BP values >140/90 mm Hg or prior documented diagnosis. Type 2 diabetes was defined when fasting plasma glucose values were ≥126 mg/dL or when the patient self-reported a previous diagnosis or current hypoglycemic drug use. The KIDGO guidelines defined chronic kidney disease (CKD) as a glomerular filtration rate <60 mL/min/1.73m2 for more than 3 months, structural renal changes, or when the patient self-reported a previous diagnosis. The glomerular filtration rate was estimated with the 2021 Chronic Kidney Disease Epidemiology Collaboration equation. 5
SARS-CoV-2 Vaccine Data
The COVID-19 vaccination in Mexico is the national strategy initiated on December 24, 2020, to vaccinate the population over 15 years old to reduce the risk of hospitalization and death in a global effort to combat the COVID-19 pandemic. 11 The vaccination began on December 24, 2020, in the federal entities of Mexico City, Querétaro, and the State of Mexico. Mexico became the first country in Latin America to receive COVID-19 vaccines authorized for use and application. The first authorized vaccine was Pfizer-BioNTech in December 2020; the second COVID-19 vaccine approved was AZD1222 by Oxford-AstraZeneca in January 2021, followed by Gam-COVID-Vac/Sputnik V, Sinovac, and CanSino in February 2021. 11
Biochemical Analysis
Blood samples from the patients were collected after admission to the emergency department. The measurements were carried out with commercially available standardized methods. Serum creatinine, serum blood urea nitrogen (BUN), C-reactive protein (C-RP), and lactic dehydrogenase (LDH) were measured using DxC 700 AU Chemistry Analyzer (Beckman Coulter, Fullerton CA). Plasma ferritin concentrations were estimated using an enzyme-linked immunosorbent assay (Beckman Coulter DxC 600i, Fullerton, CA). D Dimer levels were assessed using an ACL Top 550 CTS (Werfen Company, Spain).
Statistical Analysis
Statistical analysis was conducted using SPSS 26 (SPSS Inc., Chicago, IL). The data were checked for outliers and normality assumptions. The normality of continuous variables was evaluated using the Shapiro-Wilk normality test and visually using histograms and Q-Q plots. Values are presented as mean ± standard deviation, median (interquartile range), or frequencies (%). Means and medians were compared using the t-student test or Mann-Whitney’s U test, and frequencies were compared using the chi-squared test.
The Kaplan-Meier method was used to calculate survival distributions for groups classified by AKI and vaccine status, with statistical significance assessed using the log-rank test. Binary logistic regression models were employed to determine the association between vaccine status and AKI, 28-day mortality, and the development of AKI stage 3. These regression models, utilizing backward stepwise elimination, included the following covariates: sex, age, BMI, type 2 diabetes, hypertension, serum levels of D-dimer, lactic dehydrogenase, C-reactive protein, and ferritin. Odds ratios (ORs) with 95% confidence intervals (95% CI) were reported, and statistical significance was set at P ≤ .005.
Results
The study included 413 hospitalized patients with confirmed SARS-CoV-2 infection. Overall, 70% (n = 289) of the patients developed AKI at any stage and had a median hospital stay of 10 days (6-17). The mean age of the participants was 55.2 ± 14.8 years; 36.1% (n = 149) were women, had a mean BMI of 28.2 ± 5.5 kg/m2 (29.6% had average weight, 38.1% had overweight, and 32.3% had obesity), 44.1% had type 2 diabetes, 29.3% had hypertension, and only 5.1% had chronic kidney disease. Of the 413 patients included in the study, only 18.9% (n = 78) received at least 1 dose of the SARS-CoV-2 vaccine. Among these, 29 patients (7.0%) had 1 dose, 41 (9.9%) had 2 doses, and only 8 patients (1.9%) received 3 or more doses. AZD1222 (Oxford-AstraZeneca) was the most common vaccine, followed by Pfizer-BioNTech and Sputnik. The frequency of AKI was significantly lower in vaccinated patients compared with those who did not receive any vaccines (48.7% vs 74.9%; P < .001). Detailed demographic characteristics of the vaccinated patients are provided in the supplementary tables.
The overall mortality rate in our cohort was 28.8% (n = 119). Within this group, the 28-day mortality was 22.8% (n = 94). In addition, 29.3% of patients (n = 121) required mechanical ventilation, and 8.0% (n = 33) needed KRT. Of them, 7.3% (n = 30) received hemodialysis, and 1.2% (n = 5) underwent peritoneal dialysis.
The clinical and biochemical characteristics of the patients were classified by vaccine status and subclassified by AKI status afterward (see Table 1). Among the nonvaccinated population, those who developed AKI were significantly older, more likely to be men, had a longer length of stay in the hospital, a higher frequency of mechanical ventilation, higher median serum levels of BUN, basal, admission, and discharge creatinine, lower eGFR at admission and discharge, higher D-dimer, C-reactive protein, KRT, and mortality. Among the vaccinated population, those who developed AKI were older, had a lower BMI, had a longer length of stay in the hospital, and had higher levels of D-dimer. As expected, according to the operational definition of AKI, they had higher median serum levels of BUN, basal, admission, and discharge creatinine and lower eGFR at admission and discharge. Furthermore, we aimed to compare vaccinated patients with AKI with those who were not, serving as the control group (Supplementary Table 1). Unvaccinated patients with AKI exhibited a lower frequency of diagnosed hypertension, as well as lower median serum levels of BUN, basal creatinine, and lactate dehydrogenase. We found no bivariate association with the frequency of mechanical ventilation, serum creatinine at admission and discharge, duration of AKI, D-dimer, C-reactive protein, ferritin, and 28-day mortality. However, they tended to have lower levels in the vaccinated AKI group.
Clinical and Biochemical Characteristics of Patients With Severe COVID-19 Stratified by Vaccine Status and Acute Kidney Injury (AKI).

Variables are mean ± standard deviation, median (interquartile range), or percentages. P-value: T-student test, U Mann-Whitney, or chi 2 . BMI = body mass index; CKD = chronic kidney disease; BUN = blood urea nitrogen; LDH = lactic dehydrogenase; KRT = kidney replacement therapy; N/A = not applicable.
KDIGO stage at the onset of AKI.
The 28-day mortality distribution (Figure 2) differed among the vaccine and AKI status (χ2 = 8.469, P = .036). Multiple logistic regression models assessed the association between immunization against SARS-CoV-2 and AKI, the development of AKI stage 3, and 28-day mortality (Table 2). The unadjusted model indicated that COVID-19 vaccination was associated with lower odds of developing AKI and reduced 28-day mortality by 68.2% and 61.6%, respectively. However, AKI stage 3 did not reach statistical significance in this model. Following adjustment for clinical and demographic confounding variables, COVID-19 vaccination decreased the probability of AKI by 72.7%, AKI stage 3 by 55.8%, and 28-day mortality by 80.8%. Finally, when proinflammatory biomarkers were added to the variables of model 1, COVID-19 vaccination remained associated with lower odds of AKI by 74.8%, AKI stage 3 by 55.2%, and 28-day mortality by 81.3%.

Time-to-event analysis for COVID-19 vaccination and acute kidney injury (AKI).
Binary Logistic Regression Models of SARS-CoV-2 Vaccination and the Odds for Acute Kidney Injury (AKI), 28-Day Mortality, and the Development of AKI Stage 3 in Patients With Severe COVID-19.

Model 1 was adjusted by SARS-CoV-2 Vaccination status, age, sex, Body Mass Index, type 2 diabetes, and hypertension; model 2 included model 1 plus serum levels of D-dimer, lactic dehydrogenase, C-reactive protein, and ferritin.
Discussion
Ever since the initial documentation of the SARS-CoV-2 infection in December 2019, it has been widely acknowledged that the upper respiratory tract is the primary site of infection. 10 Nevertheless, substantial evidence indicates that beyond the respiratory system, various organs, such as the heart, liver, and kidneys, can also suffer severe repercussions. 4 ,6-8 Among these, COVID-19-induced AKI is closely associated with the critical clinical condition of patients, resulting in a worse prognosis.5,12 Although more than 8.2 billion COVID-19 vaccine doses have been administered globally to mitigate the burden of COVID-19, 13 to our knowledge, no studies have thoroughly analyzed the rate and outcomes of AKI in post-vaccine patients with severe COVID-19. Our results show that compared with their control peers, hospitalized patients with severe COVID-19 were significantly less likely to develop AKI, AKI stage 3, and had reduced 28-day mortality. It is important to note that while our study included patients with CKD who developed AKI during hospitalization, we did not have any patients on maintenance dialysis or kidney transplant recipients before their COVID-19 infection. All instances of KRT initiation occurred during hospitalization as a result of COVID-19-related complications. This distinction is important as it underscores that the need for KRT in our cohort was directly associated with the acute impact of severe COVID-19 rather than preexisting ESKD. While these results may not be directly applicable to the entire COVID-19 population due to potential differences in ethnicity or host response in other settings, vaccination against SARS-CoV-2 is unequivocally necessary not only to reduce the risk of infection but also to prevent AKI and mitigate worse outcomes in severe COVID-19 cases with AKI.
The development of COVID-19 vaccines during the worst periods of the pandemic marked one of the most challenging moments in human history. 1 The race to find a successful vaccine led to the development of numerous vaccines that have been widely authorized worldwide. Overall, 3 major types of COVID-19 were approved for emergency use during the pandemic: messenger RNA (mRNA), viral vector, and inactivated and protein subunit vaccines.1,3 The efficacy, immunogenicity, and safety of COVID-19 vaccines have been widely documented across different phase I, phase II, and phase III trials. A recent meta-analysis by Sharif et al 1 showed that the collective vaccine efficacy for the adenovirus vector vaccines was 73% (95% CI = 69-77), and for the mRNA vaccines was 85% (95% CI = 82-88). In this study, the primary type of vaccine was adenovirus vector vaccines (Oxford/AstraZeneca), followed by mRNA vaccines. In addition, different vaccine regimens have been proposed for each vaccine. However, patients of this study may not have had complete immunization as suggested by the Mexican national strategy. 11
It has been reported that AKI following the COVID-19 vaccination was more frequent than the application of other vaccines, such as influenza vaccine and yellow fever vaccine, among others.8,9 Although this study aimed to demonstrate the lower burden of AKI in hospitalized patients with severe COVID-19, some other reports have shown that SARS-CoV-2 vaccination could be partially associated with some adverse renal events.14-17 As part of this, Chen et al 15 found that coexisting active illnesses were independently associated with AKI after receiving the SARS-CoV-2 vaccine. Interestingly, they reported that having an active disease increased the odds of AKI-associated mortality by 2.19 times after receiving a COVID-19 mRNA vaccination. It has been proposed that the AKI after vaccination could be caused by high immunogenicity, especially in the mRNA vaccines that can induce increased cell-mediated and antibody-mediated immune responses. 14 It is important to highlight that this study did not account for different SARS-CoV-2 variants during the study period, which could impact vaccine effectiveness and patient outcomes. The varying transmissibility and pathogenicity of these variants may have influenced the rates of acute kidney injury and other clinical outcomes, representing a significant limitation of our analysis.
The direct impact of SARS-CoV-2 on the kidneys triggers local inflammation, attracting immune cells such as macrophages, effector T cells, and polymorphonuclear neutrophils.4,7,8 Within the lungs, damage-associated molecular patterns and pathogen-associated molecular patterns prompt the release of cytokines, which exacerbate inflammation and tissue damage by recruiting additional inflammatory cells. 4 Interferon secretion from immune cells aids in viral clearance. 9 In addition, activated neutrophils release neutrophil extracellular traps, which may further enhance the local inflammatory response, aid in pathogen clearance, and contribute to thrombosis.7,8 The enhanced release of inflammatory mediators by immune and resident kidney cells is likely to be a key mechanism of tissue damage in patients with COVID-19, the so-called cytokine storm. 8 The cytokine storm is perceived as a critical condition marked by organ failure and the swift overactivity and proliferation of all components of the immune system, such as T cells, macrophages, and natural killer cells. 18 This results in an elevated production and release of various chemical mediators and inflammatory cytokines, posing a significant threat to life.8,18 In this study, we hypothesized that severe COVID-19 infection accompanied by AKI would exhibit a diminished proinflammatory response in vaccinated individuals. Only lactic dehydrogenase levels were significantly lower in vaccinated patients with severe COVID-19 and AKI. While ferritin, C-reactive protein, and D-dimer levels did not reach statistical significance, they tended to be lower, possibly due to the sample size.
This study has several strengths. To the best of our knowledge, this was the first case-control study to investigate the association between SARS-CoV-2 vaccination and the development of AKI, AKI stage 3, and 28-day mortality. Other reports have only focused on the rare adverse renal events of the COVID-19 vaccine. While we did not identify a significant reduction in proinflammatory makers after vaccination, reporting these negative results is valuable for future research. Another strength is that the population included exclusively comprised patients with severe COVID-19, allowing us to analyze the course of the disease in the setting of severe inflammation.
On the other hand, our study has some significant limitations. Being a single-center retrospective study in Mexico, the results may be challenging to generalize, and further studies are needed to confirm our findings. Secondly, the COVID-19 vaccination data was extracted from medical records within our institution. Thus, we could not verify the adequacy of its administration and the duration between administration and the onset of AKI. Third, our cohort’s relatively small proportion of vaccinated patients may limit our findings’ statistical power and generalizability, necessitating more extensive studies to validate these results. An additional limitation to consider is the potential for selection bias. Patients who received the COVID-19 vaccine may have had more regular contact with healthcare services due to preexisting chronic conditions, making them more likely to engage with vaccination programs and other preventive measures. Our institution, being a major referral center, serves a population with significant health disparities, including high levels of illiteracy and limited access to information. While vaccines were accessible at local primary care centers, differences in health-seeking behaviors and access to timely treatment could have contributed to the observed lower risk of AKI among vaccinated patients. This potential selection bias should be considered when interpreting the protective effect of vaccination observed in our study. Moreover, we could only confirm if patients had prior COVID-19 hospitalizations within our institution, as this was based solely on the available clinical records. Another limitation was the inclusion of patients from April 2020, before the availability of COVID-19 vaccines, which may have influenced the comparison of outcomes between vaccinated and unvaccinated groups.
Furthermore, significant advancements in the understanding and management of COVID-19 occurred during the study period from April 2020 to December 2021. These advancements, including improved clinical protocols, corticosteroids, and antiviral treatments, could have contributed to better patient outcomes independent of vaccination status.19,20 Therefore, these temporal changes in treatment strategies might confound the observed protective effect of vaccination on AKI and mortality. Future studies should consider a narrower timeframe or stratified analysis to account for these rapid developments in COVID-19 management. Finally, there was an imbalance in baseline comorbidities between the vaccinated and nonvaccinated groups, with the vaccinated patients exhibiting higher rates of hypertension, diabetes, and CKD. These preexisting conditions are known risk factors for more severe AKI. They may have contributed to the observed increase in stage 3 AKI and the need for KRT among the vaccinated patients. In addition, the lack of statistical significance in the logistic regression models for stage 3 AKI suggests that the protective effect of vaccination on severe AKI outcomes should be interpreted with caution. Future studies should consider adjusting for these comorbidities more robustly to isolate the impact of immunization on AKI severity.
Conclusions
In conclusion, in this case-control study of hospitalized patients with AKI and severe COVID-19, the application of at least 1 dose of the SARS-CoV-2 vaccine was associated with lower odds for AKI, AKI stage 3 and 28-day mortality, independently of demographic, clinical, and proinflammatory data.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581241297369 – Supplemental material for COVID-19 and Acute Kidney Injury Outcomes in Hospitalized Patients Following SARS-CoV-2 Vaccination: A Case-Control Study
Supplemental material, sj-docx-1-cjk-10.1177_20543581241297369 for COVID-19 and Acute Kidney Injury Outcomes in Hospitalized Patients Following SARS-CoV-2 Vaccination: A Case-Control Study by Froylan D. Martínez-Sánchez, Luis A. Bastida-Castro, José L. Torres-Cuevas, Julio A. Vasquez-Vasquez, Alejandra Diaz-Jarquin, Rafael Moreno-Novales, Joana Balderas-Juarez, Mauricio A. Salinas-Ramírez, Jose L. Hernández-Castillo and Erika K. Tenorio-Aguirre in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
This paper is dedicated to my father, Froylan Martínez Marín, who sadly passed away on December 29, 2023. Thank you for your support and love. I will always love you, dad. The present work results were partially presented at Kidney Week 2022 in Philadelphia as a poster titled “Outcomes Among Hospitalized Patients with COVID-19 and Acute Kidney Injury: Role of SARS-CoV-2 Vaccine.”
Author Contributions
F.D.M.S. L.A.B.C., J.L.T.C., M.A.S.R., and J.B.J. conceived the project, researched and analyzed data, contributed to the discussion, and wrote the manuscript. F.D.M.S. edited the final draft. J.A.V.V., A.D.J., R.M.N., and E.K.T.A. researched data and contributed to the discussion. F.D.M.S. and J.B.J. are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the HGDMGG Research Committee and Research Ethics Committee (REF 14-17-2022) and conducted according to the 1975 Declaration of Helsinki. Upon medical admission, the patient or a family member signed an informed consent form permitting the use of his/her medical file information for didactic, research, and publication purposes.
Availability of Data and Materials
All data and materials are available from the corresponding author and will be made available at a reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.