
Abstract
Background:
There are several steps patients and their health care providers must navigate to access kidney transplantation in British Columbia (BC).
Objective:
We explored perceptions and experiences with the pretransplant process across BC to determine where process improvements can be made to enhance access to transplantation.
Design:
Anonymous surveys were sent online and via post to health care providers (including nephrologists, registered nurses, and coordinators) and patients across BC.
Setting:
Kidney care clinics, transplant regional clinics, and provincial transplant centers in BC.
Measurements:
Surveys included Likert scale questions on the current pretransplant process and transplant education available in BC. The health provider survey focused on understanding the pretransplant process, knowledge, roles, and communication while the patient survey focused on patient education and experience of the pretransplant processes.
Results:
A total of 100 health care providers and 146 patients responded. Seventy-six percent of health care providers understood their role and responsibility in the pretransplant process, while only 47% understood others’ roles in the process. Fifty-nine percent of health care respondents felt adequately supported by the provincial donor and transplant teams. Seventy-one percent of registered nurses and 92% of nephrologists understood transplant eligibility. About 68% and 77% of nurses and nephrologists, respectively, reported having enough knowledge to discuss living donation with patients. Fifty percent of patients had received transplant education, of which 60% had a good grasp of the pretransplant clinical processes. Sixty-three percent felt their respective kidney teams had provided enough advice and tools to support them in finding a living donor. Fifty percent of patients reported feeling up to date with their status in the evaluation process.
Limitations:
This analysis was conducted between December 2021 and June 2022 and may need to account for practice changes that occurred during the COVID-19 pandemic. Responses are from a selection of health care providers, thus acknowledging a risk of selection bias. Furthermore, we are not able to verify patients who reported receiving formal transplant education from their health care providers.
Conclusions:
Exploring these themes suggests communication with regional clinics and transplant centers can be improved. In addition, patient and staff education can benefit from education on kidney transplantation and the pretransplant clinical processes. Our findings provide opportunities to develop strategies to actively address modifiable barriers in a patient’s kidney transplantation journey.
What was known before
Patients with chronic kidney disease in British Columbia take several steps to complete their transplant evaluation before kidney transplantation, including transplant education and support in finding living donors.
What this adds
This study identifies opportunities within our current pretransplant processes to improve patients’ journey to kidney transplantation in British Columbia.
Background
For patients with end-stage kidney disease (ESKD), kidney transplantation improves quality and length of life.1,2 In 2019, more than 3000 Canadians were on the kidney transplant waitlist; however, 45% were unable to receive kidney offers owing to inactive waitlist status. 3 The process toward receiving a kidney transplant is complex, with several steps for patients and health care providers to navigate and complete. In British Columbia (BC), kidney transplant evaluation occurs at 2 tertiary transplant centers in Vancouver. Patients often require several visits for assessment and investigations while some travel long distances for these tests and medical reviews. Medical factors such as patient co-morbidities and immunological compatibility can affect medical suitability and, thus, access to transplantation. 4 Nonmedical (potentially modifiable factors) are considered multilevel health system factors. 5 Suggested factors such as provider biases, lack of patient knowledge, and poor communication between care providers contribute to the barriers to receiving a kidney transplant.6,7 In addition to the breakdown in communication between transplant centers and regional clinics, inconsistent health care provider training and the financial burden on donors and recipients were cited as barriers to living donation in BC. 8
Worldwide, there is no absolute measure of how and when patients should be referred for transplant evaluation. Kidney Disease Improving Global Outcomes (KDIGO) suggests potential kidney recipients should be referred for evaluation 6 to 12 months before anticipated dialysis initiation, emphasizing preemptive transplantation. 9 To help achieve this goal in BC, BC Transplant and BC Renal, which, respectively, oversee the transplant processes and the rest of chronic kidney disease (CKD) care in BC, launched the Transplant First initiative. The Transplant First initiative aims to ensure every kidney care clinic (KCC) patient (estimated glomerular filtration rate [eGFR] < 25) in BC who is a potential kidney transplant candidate is considered, identified, assessed, and supported along the path toward transplantation as the treatment of choice, including assistance in finding a living donor.
To determine where process improvements can be made within the context of this provincial transplant program, we developed a survey to assess health care providers’ and potential transplant recipients’ perceptions and experiences with the current transplant pretransplant process. These key stakeholder perspectives will be integral in the identification of any potentially modifiable nonmedical barriers encountered by nondialysis-dependent CKD patients in the steps toward transplant evaluation within BC.
Methods
Study Setting
These surveys were conducted across the province of BC, Canada. In BC, there are 15 regional KCCs that care for over 13 000 patients living with nondialysis-dependent CKD. The recipient identification and assessment process is shown in Figure 1. The process of screening and identifying potential recipient candidates for education, and determining their willingness and suitability to proceed is initiated in the KCCs with dedicated pretransplant registered nurses. Referral and initial testing process is also performed by KCC staff. The transplant referral is submitted to one of the transplant centers where the remaining of the requisite testing and assessments are completed. About 50% to 60% of all kidney transplantation performed annually in BC are from living donors. 10 Between 2015 and 2019, there was a median of 272 (mean = 254) referrals per year submitted from the KCCs; a median of 100 living donor transplants was conducted per year, of which a median of 38 were preemptive living donor transplants.
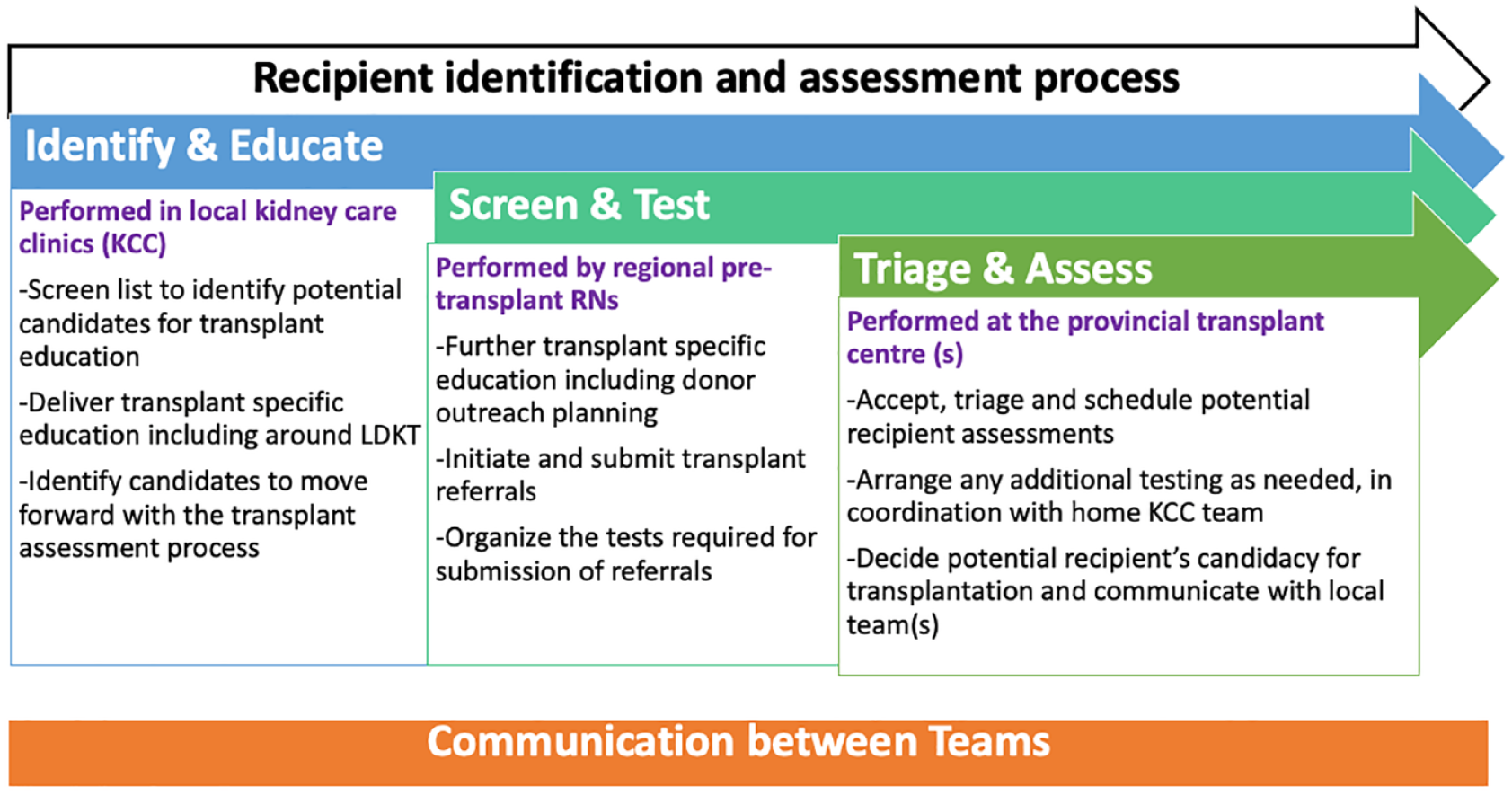
Pretransplant process in British Columbia.
Survey Design
A dedicated Evaluation Working Group was formed as part of a larger initiative in BC to promote living donor transplantation called Transplant First. This Evaluation Working Group included transplant nephrologists, general nephrologists, a methodologist, statisticians, and project managers. The Evaluation Working Group developed a multimodal evaluation framework containing goals and objectives for the Transplant First initiative. From this evaluation framework, metrics that would require direct feedback from recipients and health care providers were highlighted as the target for these surveys. A subgroup of the Evaluation Working Group then convened to design the survey questions; this included a subset of the members listed above, quality improvement specialist and a patient partner. These developments were initiated on September 13, 2021, initially focusing on the development of the health care provider survey, followed by the recipient survey. In addition to communications with other groups in the transplant field, a literature search was conducted to identify any existing or validated tools that addressed these items. Where no tools were found, the Working Group developed questions in accordance with the evaluation framework.
Using this framework, the survey was designed to explore the following themes for health care providers; knowledge and understanding by interdisciplinary teams of the pretransplant process (including roles and responsibilities), interdisciplinary team communication across care settings and between health providers, potential recipients about their transplant journey, and provider perception of the patient experience in their transplant journey. For the patient survey, the themes we explored include knowledge and understanding of the pretransplant process, and experience in their transplant journey, including the capacity to approach donors.
Two surveys were developed: a health provider survey and a patient survey (supplementary file). Where relevant, efforts were made to ensure alignment between the 2 surveys.
Participants, Recruitment, and Survey Methods
For the clinician survey, all health care providers at KCCs, regional transplant clinics, and the 2 BC provincial transplant centers were invited to participate via broadcast emails to all these clinical groups, thus unable to capture a response rate. Health care providers include nephrologists, transplant nephrologists, registered nurses, social workers, unit, recipient, and donor coordinators. For the patient survey, a list of potential candidates was generated via PROMIS (Patient Records and Outcome Management Information System), 11 the bespoke renal database encompassing all renal and transplant care in BC. To identify potential participants who would be at a stage where transplant discussions would be expected, potential participants had to meet all of the following inclusion criteria: active KCC patients between >18 and ≤80 years of age, eGFR < 20, ≥1 KCC visit completed, and no absolute contraindications to transplant listed in the PROMIS modality assessment module. A list was then generated of patients who met all these criteria. These patients were invited to participate via a mailout containing the information to access the survey and a direct QR code linking to the online survey.
The clinician surveys were offered online and, for ease of use, hosted via Survey Monkey (Momentive Inc, San Mateo, California), supported by BC Renal. For the patient survey, a tool more tailored for this purpose was selected, in this case, Checkbox (Checkbox Survey Solutions Inc, Watertown, Massachusetts). The clinician survey was active for 4 weeks from December 2021 to January 2022, and the patient survey was active for 10 weeks from June to July 2022. All surveys were offered in English.
Data Analysis
Respondents were asked to indicate their agreement with statements in the survey using a 5-point Likert scale (see supplement). The Likert scale was combined into 2 dichotomous categories of “yes” and “no” for the analysis. The response “Yes” was an aggregate of “strongly agree” and “agree,” while “No” was an aggregate of “neutral,” “strongly disagree,” and “disagree.” Responses from the online surveys were exported into Microsoft Excel, and descriptive statistics were reported. Respondents with incomplete surveys were still included in the overall survey response rate. When calculating the proportions of responses for each question, only those who responded to the question of interest were included.
Microsoft Excel and R software were used to analyze responses. All P values were 2-sided and statistically significant at the P < .05 level.
Results
A total of 100 surveys were completed by health care providers working within KCCs, Regional Transplant Clinics, and Provincial Transplant centers across the province. Among the staff respondents, the majority were registered nurses, 33 (33%). Nephrologists (13 [13%]), unit coordinators (14 [14%]), and social workers (12 [12%]) had similar response rates. Two (2%) were donors and 3 (3%) were recipient coordinators. Fifty percent had worked in the clinic setting for more than 5 years. A total of 71 respondents worked within the KCC, 28 at a regional transplant clinic and 15 at a provincial transplant center (Table 1). Supplementary figures provide 5-scale Likert health care staff responses.
Participant Characteristics.

Note. Missing data not included in count.
10.
12.
1 “don’t know.”
A total of 1705 mail-outs were sent, and 155 surveys were completed by patients for a response rate of 9%. Nine patient survey results were excluded from the analysis; 5 patients were not aware whether they had received transplant education and 4 patients did not respond to questions relating to transplant education.
Health Care Provider Survey Results
Forty-three percent of health care providers (23% of which are nephrologists) provided transplant education in advance of other renal replacement therapy options at their clinics across the province. This response was consistent at KCCs and regional transplant clinics (Table 2).
Knowledge and Understanding of Pretransplant Process Including Roles and Responsibilities of Interdisciplinary Teams.

Note. Coordinators include donor and recipient coordinators.
Recipient coordinator only responses.
Understanding of the Pretransplant Process Including Roles and Responsibilities of Multidisciplinary Teams
Seventy-seven percent of nephrologists and 55% of nurses were aware of the patient criteria required for evaluation at the provincial transplant center (Table 2). About 64% and 62% of nurses and nephrologists, respectively, understood the tests required for their patients to proceed with a referral for transplant evaluation at the tertiary transplant center.
Seventy-six percent felt they understood their role and responsibility in the pretransplant process while 47% were aware of other members’ roles and responsibilities. Sixty-two percent of staff felt patients’ primary care providers were not adequately informed of the pretransplant process, and 76% thought primary care providers were unaware of their patients’ stages in the transplant evaluation journey.
Communication During the Pretransplant Process
Fifty-nine percent of health care respondents felt able to contact the provincial donor and transplant teams for information and support (Table 3). Ninety-two percent of health care staff working in the provincial transplant centers could access information regarding patients’ stages in the transplant evaluation journey, compared with 11% and 27% in KCCs and regional transplant clinics. Ten percent of staff working in KCCs and transplant clinics were able to obtain potential donor information in the evaluation process. When questions arose in the transplant process, 71% and 78% of health care staff working in these clinics, respectively, could readily access members of the multidisciplinary team involved in the transplant process.
Communication Across Care Settings and Between Health Providers.

Note. Coordinators include donor and recipient coordinators.
Donor coordinator only responses.
Staff Knowledge About Pretransplant Process
Seventy-one percent of registered nurses and 92% of nephrologists reported having enough knowledge to educate patients about transplant eligibility (Table 4). About 68% and 77% of nurses and nephrologists, respectively, had enough knowledge to discuss living donation with patients. Forty-seven percent of health care workers knew the steps involved in the transplant evaluation process.
Staff Knowledge.

Note. Coordinators include donor and recipient coordinators.
Recipient coordinator only responses.
Donor coordinator.
Eighty percent of staff who responded to the survey felt finding a living donor challenging to navigate and complete for patients. Forty-six percent of nephrologists and 48% of nurses reported having sufficient knowledge to support their patients in finding a living donor.
Staff Perception of the Patient Experience
Overall, 28% of health care respondents perceived their patients had a good grasp of all steps in the transplant process, and it was easy for them to navigate (Table 5). Nineteen percent of health care providers felt finding a donor was easy to navigate for their patients. All coordinators, however, felt their patients understood the process well, could navigate the evaluation system, and find a living donor.
Staff Perception of the Patient Experience.

Note. Coordinators include donor and recipient coordinators.
Donor coordinator only responses.
Patient Survey Results
A total of 146 survey results were included in the analysis. Of these, 72 patients had received transplant education, while 74 patients were yet to receive transplant education. Overall, there were more positive responses from patients who had received transplant education than those yet to receive an education.
Patient Education and Understanding of the Transplant Process
Seventy-four percent of patients were satisfied with the transplant education, and 46% had transplant education preceding other forms of renal replacement therapy. Eighty-five percent of potential kidney recipients who received transplant education felt equipped with information to discuss family and social circle about living donation. Among those yet to receive transplant education, 35% were confident approaching family and friends regarding living donation. Sixty-three percent of patients reported their kidney teams had provided enough advice and tools to support them in finding a living donor (Figure 2). Some comments that are representative of patient education and understanding include the following: “Honestly, my kidney team have not discussed about kidney transplant. I was being educated about going into dialysis.” “I am told that I will be automatically put on transplant waiting list once I start dialysis.”

Bar chart showing patient survey responses.
Patient Experience of Transplant Process
Patients who received transplant education were more likely to understand the investigations required for the transplant evaluation process (66% vs 22%). Fifty-two percent of the patients who received education thought the investigations were easy for them to complete, and 61% said they were supported by their health care team throughout the testing process. Fifty-one percent of patients who received education responded they were updated regarding their status in the pretransplant process, while 75% of potential kidney recipients who had received transplant education were comfortable seeking information or questions about the transplant process compared with 44% of potential recipients yet to receive transplant education. Some comments that are representative of patients’ experience in the transplant evaluation process include the following: “Have had blood work done for a possible donor and now haven’t heard anything in months.” “Most people I talk to are reluctant to commit to donation.”
Discussion
We conducted surveys for health care providers and patients to explore the perception of our current pretransplant process across the province; the responses offer insight and provide an opportunity to identify and address barriers during the education and assessment phases of the kidney transplantation process.
In BC, the primary responsibility of determining the suitability of potential kidney recipients is served by the transplant nephrologist; however, general nephrologists play a vital role as their existing relationship with patients provides a platform to recognize patients who may benefit from kidney transplantation and initiate these conversations. Seventy-seven percent of nephrologists were aware of the patient referral criteria, while 62% were aware of tests required for transplant evaluation at the provincial transplant center. Health care staff in regional transplant clinics were more familiar with these referral criteria than those in KCCs (72% vs 47%). Similarly, less than half of the staff respondents were aware of the transplant evaluation process. Lack of awareness of the transplant process is reported as the third significant barrier to kidney transplantation by health care staff in the Southeastern United States. 12 Health care providers in BC previously expressed the need for formalized training sessions as they felt this was a barrier to preemptive live donor kidney transplantation (LDKT). 8 There are ongoing opportunities to enhance access to transplantation by focusing on improving the understanding and familiarity with the pretransplant process and candidate selection criteria among general nephrologists and other KCC staff.
Transplant education emerged as a major theme in staff and patient survey responses. Patients who begin transplant education within their dialysis centers or from their community nephrologists are more likely to complete transplant evaluation successfully, get on the transplant waiting list, and receive living donor kidney transplants.5,13-15 The KDIGO recommends commencing transplant education once eGFR is <30 mL/min/1.73 m2 in all patients expected to reach ESKD and for transplant workup to begin at least 6 to 12 months before anticipated dialysis initiation. 9 From our analysis, only 23% of nephrologists and 55% of nurses provided transplant education in advance of other renal replacement therapies (RRTs). About 38% and 29% provided transplant education prior to other RRTs at kidney care and regional transplant clinics, respectively, indicating that focusing on early transplant discussions may be another potential strategy to consider.
Educating patients on the donor’s experiences, motivations, and benefits of living versus deceased transplantation may increase patients’ comfort with LDKT. Our study shows that more than 60% of patients felt equipped with the knowledge, practical advice, and tools to approach a potential donor after transplant education. While this is a 3-fold increase compared with those who did not yet have education, the remaining 40% did not feel confident with the knowledge received to approach donors; indicating there are further opportunities to close the knowledge gap and improve transplant education.
Following the completion of transplant education, our analysis revealed that at least 60% of patients understood the pretransplant clinical processes and felt supported by their health care provider during the testing process. More than 70% of patients knew who to contact should questions arise during the process. Interestingly, there is a distinction between patient and staff responses. About 20% of health care staff indicated their patients had a good grasp of the transplant process and were easy to navigate. This discordance suggests longitudinal conversations with patients after the initial transplant education is necessary. The patient survey responses reveal less than half (40%) of patients received transplant education multiple times.
Communication emerged as another theme from our survey responses, a common concern from previous studies on nonmedical barriers to kidney transplantation.7,8,12 While 78% of health care providers in provincial transplant centers could obtain information on the progress of kidney donor evaluation, only 10% of KCC and regional transplant clinic health care providers felt updated with donor evaluation progress. This suggests there are opportunities to improve the current means of communication between provincial transplant centers and other clinics.
All health care providers acknowledged inadequate communication about the patient’s journey and transplant processes with their primary care providers. Only one respondent (nephrologist) confirmed that primary care doctors were informed about the patient’s journey in the pretransplant processes. Patients rely on their primary care physicians to help access specialized medical care 16 and are likely to provide support and motivation for their patients with kidney disease, including donor outreach. Primary care is an underutilized resource, and understanding how best to integrate primary care providers into this process requires further exploration.
The strengths of this study are it captures a broad range of perspectives, including physicians, patients, nurses, and coordinators serving a diverse patient population as we have in BC. We explore staff and patient perceptions of the transplant evaluation process. Studies in this area typically focus on dialysis staff perception and are generally not presented with self-described patient perspectives on transplant evaluation. Our survey findings reflect the importance of communication on a patient level and among various health care staff involved in managing CKD.
Limitations must be considered in interpreting results. Given the requirement for participants to agree to participate in this study, we acknowledge the risk of selection bias. Interest for survey participation was sent via post to capture patients who do not have electronic means to assess information. Our findings may also be affected by patient and staff response bias; however, this was addressed by making the survey anonymous. Our results from the patient survey rely on self-reported education on kidney transplantation, thus subject to recall bias. Furthermore, we are not aware of which patients received formal transplant education.
Another limitation to consider is our survey is not exhaustive. Our survey allowed us to understand better the current state of BC’s pretransplant processes, its complexities, and potential challenges. Our survey did not examine patient demographics; however, multiple studies continue to advance the discussions on racial, age, and sex disparities in kidney transplant referral, evaluation, and waitlisting.17-19
Finally, our survey was conducted during the COVID-19 pandemic and may need to account for practice changes that occurred during the pandemic. There was an increase in telehealth tools during the pandemic, likely impacting responses.
Conclusion
We have identified elements within our pretransplant practice that serve as an opportunity to improve access to transplantation in BC. Improvement strategies should prioritize communication between stakeholders, particularly provincial transplant centers and other kidney clinics, health care staff training on transplant processes, and timely (including reinforcement) transplant education for our patients. Future projects should focus on streamlining the current pretransplant process and quality improvement programs on transplant education.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581241256735 – Supplemental material for Opportunities for Improving the Transplant Assessment and Education Process in British Columbia: Patient and Health Care Provider Perspective
Supplemental material, sj-docx-1-cjk-10.1177_20543581241256735 for Opportunities for Improving the Transplant Assessment and Education Process in British Columbia: Patient and Health Care Provider Perspective by Oshorenua Aiyegbusi, Sharon Gradin, Yanchini Rajmohan, Bingyue Zhu, Alexandra Romann, Helen Chiu, Jagbir Gill, Olwyn Johnston and Micheli Bevilacqua in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-docx-2-cjk-10.1177_20543581241256735 – Supplemental material for Opportunities for Improving the Transplant Assessment and Education Process in British Columbia: Patient and Health Care Provider Perspective
Supplemental material, sj-docx-2-cjk-10.1177_20543581241256735 for Opportunities for Improving the Transplant Assessment and Education Process in British Columbia: Patient and Health Care Provider Perspective by Oshorenua Aiyegbusi, Sharon Gradin, Yanchini Rajmohan, Bingyue Zhu, Alexandra Romann, Helen Chiu, Jagbir Gill, Olwyn Johnston and Micheli Bevilacqua in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-docx-3-cjk-10.1177_20543581241256735 – Supplemental material for Opportunities for Improving the Transplant Assessment and Education Process in British Columbia: Patient and Health Care Provider Perspective
Supplemental material, sj-docx-3-cjk-10.1177_20543581241256735 for Opportunities for Improving the Transplant Assessment and Education Process in British Columbia: Patient and Health Care Provider Perspective by Oshorenua Aiyegbusi, Sharon Gradin, Yanchini Rajmohan, Bingyue Zhu, Alexandra Romann, Helen Chiu, Jagbir Gill, Olwyn Johnston and Micheli Bevilacqua in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
All authors thank the transplant first committee and working groups, BC renal CKD research groups for their feedback on our methodology and the PAAC project group, Alberta, on sharing their experience and survey questions in a similar project.
Ethics Approval and Consent to Participate
The study protocol was reviewed by our institutional research ethics board and approved to proceed as a limited risk study exempt from full review. Informed consent was obtained from all patients and care providers who volunteered to participate in the surveys.
Consent for Publication
Consent for publication was obtained from all authors.
Availability of Data and Materials
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.