
Abstract
Purpose of review:
Cardiovascular (CV) disease is a major cause of morbidity and mortality for patients with glomerular disease. Despite the fact that mechanisms underpinning CV disease risk in this population are likely distinct from other forms of kidney disease, treatment and preventive strategies tend to be extrapolated from studies of patients with undifferentiated chronic kidney disease (CKD). There is an unmet need to delineate the pathophysiology of CV disease in patients with glomerular disease, establish unique risk factors, and identify novel therapeutic targets for disease prevention. The aims of this narrative review are to summarize the existing knowledge regarding the epidemiology, molecular mechanisms, and management of CV disease in patients with common glomerular disease, highlight the patient perspective, and propose specific areas for future study.
Sources of information:
The literature for this narrative review was accessed using common research search engines, including PubMed, PubMed Central, Medline, and Google Scholar. Information for the patient perspective section was collected through iterative discussions with a patient partner.
Methods:
We reviewed the epidemiology, molecular mechanisms of disease, management approaches, and the patient perspective in relation to CV disease in patients with glomerulopathies. Throughout, we have highlighted the current knowledge and have discussed future research approaches, both clinical and translational, while integrating the patient perspective.
Key findings:
Patients with glomerular disease have significant CV disease risk driven by multifactorial, molecular mechanisms originating from their glomerular disease but complicated by existing comorbidities, kidney disease, and medication side effects. The current approach to risk stratification and treatment relies heavily on existing data from CKD patients, but this may not always be appropriate given the unique pathophysiology and mechanisms associated with CV disease risk in patients with glomerular disease. We highlight the need for ongoing glomerular disease-focused studies aimed to better delineate CV disease risk, while integrating the patient perspective.
Limitations:
This is a narrative review and does not represent a comprehensive and systematic review of the literature.
Introduction
It is well-established that patients with chronic kidney disease (CKD) have a disproportionately high burden of cardiovascular (CV) disease. 1 Large-scale population studies in individuals with CKD have convincingly shown that the risk of major adverse CV events increases with both a reduction in estimated glomerular filtration rate (eGFR) and an increase in albuminuria.2 -4 Kidney Disease Improving Global Outcomes (KDIGO) guidelines suggest that lipid-lowering therapy be used for primary prevention in patients with a 10-year risk of a CV event of more than 10%, and in all patients with CKD over the age of 50 years. 5 To date, studies of CV risk in patients with kidney disease have been dominated by older patients with undifferentiated CKD and a high burden of traditional risk factors, such as diabetes, longstanding hypertension, and atherosclerosis. In contrast, there has been a paucity of studies examining the risk of CV events in patients with specific forms of kidney disease, such as glomerulonephritis (GN). It is unclear if the CKD guidelines should similarly apply to individuals with GN, who might be younger and have a different risk factor profile compared with those with undifferentiated CKD.
The pathophysiology of CV disease in individuals with GN is complex and multifactorial, involving a range of molecular and cellular processes. It includes both traditional and non-traditional risk factors, some of which might be unique to the underlying GN. Glomerular disease activity tends to wax and wane over time, as patients experience periods of relapse and remission. When the disease is active, patients are at risk of complications, such as systemic inflammation or vascular thrombosis in the setting of nephrotic syndrome. The treatment of GN could itself contribute to the risk of CV events, for example, related to toxicity of immunosuppression, such as corticosteroids 6 or calcineurin inhibitors. Because patients with GN are often diagnosed at a young age, one must also consider the cumulative burden of both their kidney disease and the scope for complications, such as CV disease from a life-course perspective (Figure 1).
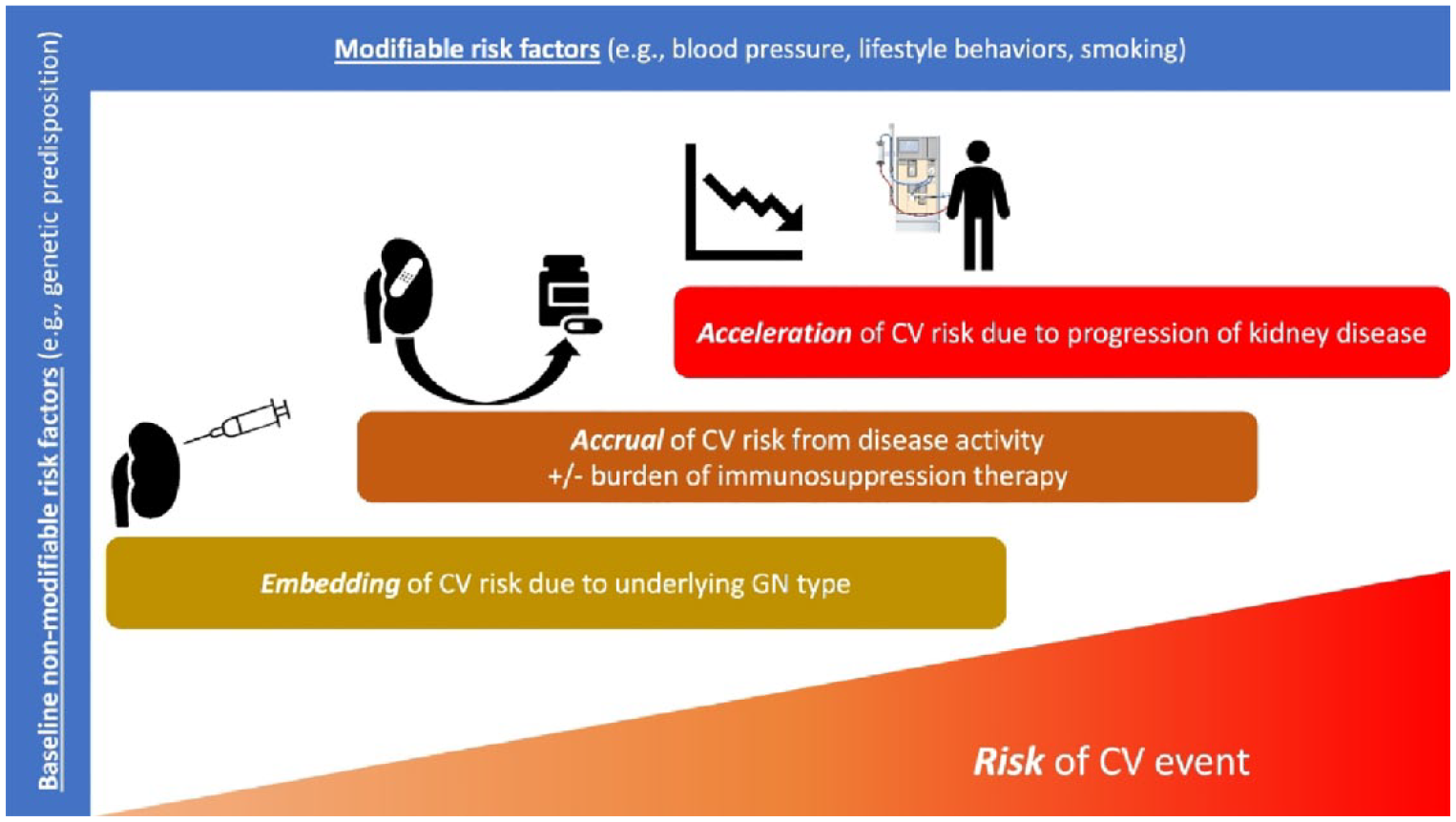
Conceptual framework for the development of cardiovascular risk in patients with glomerulonephritis across the life course.
The objectives of this narrative review are to describe the epidemiology and the pathophysiology of CV disease in patients with GN, identify potential treatment strategies to reduce CV risk, and discuss priorities and challenges of such strategies from the perspective of a patient with GN. The case is hypothetical but reflects real-life experiences that have been shared by patients with kidney disease. We specifically focus on arterial CV events, although we acknowledge that hypercoagulability and venous thrombotic events are an important source of morbidity in people with GN. Throughout, we highlight knowledge gaps and opportunities for future research (Table 1; Box 1–3).
Knowledge Gaps and Opportunities to Reduce the Burden of Cardiovascular Disease in Patients With GN.

Note. GN = glomerulonephritis; CV = cardiovascular; SGLT2i = sodium glucose co-transporter 2 inhibitors.
Clinical Vignette.
Clinical Vignette.

Clinical Vignette.

Epidemiology of CV Disease in Patients With GN
What Is the Incidence of CV Events?
Because GN is a rare condition, obtaining accurate population-level estimates of CV disease in people with GN is challenging. O’Shaughnessy and colleagues 9 used the United States Renal Data System to evaluate the risk of major CV events (myocardial infarction, ischemic stroke, or CV death) among 658 168 patients with different causes of kidney failure who initiated dialysis between 1997 and 2014. As expected, the event rate was highest in patients with diabetic nephropathy (14.34 events per 100 person-years). Compared with immunoglobulin A (IgA) nephropathy, after adjusting for potential confounding variables, the risk of a CV event was higher in patients with focal segmental glomerulosclerosis (FSGS, hazard ratio [HR] = 1.65, 95% confidence interval (CI) = 1.53-1.78), membranous nephropathy (HR = 1.67, 95% CI = 1.52-1.83), lupus nephritis (HR = 1.86, 95% CI = 1.71-2.03), and vasculitis (HR = 1.55, 95% CI = 1.41-1.71). This study was the largest to demonstrate heterogeneity in CV risk among specific forms of GN but had some limitations, including potential misclassification of GN based on physician reporting as opposed to a biopsy, and lack of information about risk factors, such as dyslipidemia or hypertension. Most importantly, the index date only started after initiation of dialysis, whereas one would ideally want to identify high-risk patients much earlier in the course of their kidney disease.
Few studies have evaluated the risk of CV events from the time of kidney biopsy in patients with GN. A study from 2 centers in the United States and Canada examined the incidence of CV events from the time of biopsy in patients with membranous nephropathy, with kidney failure treated as a competing risk. 10 The cumulative incidence of CV events was 4.4% at year 1 and 8.8% at year 5. In the first 2 years after diagnosis, the risk of a CV event exceeded the risk of kidney failure among patients with preserved kidney function at baseline. A population-based study from British Columbia (BC), Canada, expanded on this study to include other forms of primary GN. 11 The investigators employed administrative data linkages to estimate the absolute risk of major CV events in 1912 adult patients with IgA nephropathy (n = 759), FSGS (n = 540), membranous nephropathy (n = 387), and minimal change disease (MCD, n = 226). During a median follow-up time of 6.8 years, 212 patients experienced a CV event, representing an incidence rate of 24.7 per 1000 person-years, some 2.5 times as high as the age- and sex-matched general adult population. The 10-year risk of CV events was 16% (95% CI = 13.8-18.3) and differed by GN type, being highest in FSGS (27%) and lowest in IgA nephropathy (7.7%). Notably, each type of GN had an incidence rate that exceeded 10 events per 1000 person-years, the threshold suggested by KDIGO to initiate lipid-lowering therapy for primary prevention of CV disease. Although this study provided population-level estimates of absolute CV risk, the lack of a control population with other forms of CKD, such as diabetic kidney disease precluded an assessment of relative risk across different causes of CKD at similar levels of eGFR and albuminuria. This, and other limitations from prior studies are summarized in Table 2.
Summary of Studies Examining the Incidence of and Risk Factors for Cardiovascular Events in Patients With Glomerular Disease.

Note. CV = cardiovascular; CI = confidence interval; eGFR = estimated glomerular filtration rate; GN = glomerulonephritis; HR = hazard ratio; IgAN = IgA nephropathy; FSGS = focal segmental glomerulosclerosis; MN = membranous nephropathy; MPGN = membranoproliferative glomerulonephritis; ADPKD = autosomal dominant polycystic kidney disease; MCD = minimal change disease; CKD = chronic kidney disease.
What Are the Risk Factors for CV Disease?
There are limited data available in the literature, which describe specific risk factors for CV events in this population. A single-center study of 298 consecutive patients with nephrotic syndrome showed that traditional risk factors, such as male sex, older age, diabetes, smoking, and hypertension were associated with arterial thromboembolic events. 12 Proteinuria and serum albumin levels were predictors of venous but not arterial thromboembolic events. This analysis was likely underpowered due to small sample size and low event rate. In the 2 aforementioned studies from Canada, older age, the presence of diabetes, and a prior history of CV disease were all independently associated with higher risk of a CV event during follow-up.10,11 In the BC cohort, a multivariable model that incorporated traditional risk factors had a C-statistic of 0.82 (95% CI = 0.79-0.85). Adding type of GN, magnitude of proteinuria and level of kidney function at the time of biopsy to the model led to improvements in model fit, discrimination (C-statistic 0.84, 95% CI = 0.81-0.87) and reclassification, suggesting that the inclusion of GN-specific variables can improve CV risk stratification. 11 Consistent with this finding, the severity of nephrotic syndrome over time was identified as an independent risk factor for CV events among patients with membranous nephropathy (HR = 2.2, 95% CI = 1.1-4.3). 10 Although identification of CV risk factors can refine an individual patient’s risk profile, they do not necessarily tell us what is driving the risk in patients with GN. In the next section, we explore potential mechanisms of CV disease in this population.
Mechanisms of CV Disease in GN
Mechanisms of CV disease in GN can be broadly classified as traditional and non-traditional. Traditional risk factors for CV diseases are highly prevalent in patients with GN. They include hypertension, diabetes mellitus, obesity, and dyslipidemia. However, non-traditional risk factors, such as inflammation,13 -16 endothelial dysfunction,17 -25 oxidative stress,13,26 -28 and vascular calcification 29 also contribute to the increased CV disease risk (Table 3). Most of these risk factors are also implicated in CKD pathophysiology; however, some are disease or treatment specific. As an example, immunosuppressive drugs, such as prednisone, calcineurin inhibitors and antimetabolites, can contribute to the development of CV disease through the promotion of cardiac hypertrophy and fibrosis, mitochondrial dysfunction, arrhythmia, hypertension, vascular remodeling, and dyslipidemia development. 30 Importantly, relevant studies on how the pathophysiology of CV disease in GN patients compares with CKD have not been done.
The extent to which the factors discussed in Table 3, alone or in combination, contribute to development of CV disease in patients with GN requires further interrogation. Compared with patients with undifferentiated CKD who often present quite late in the disease course, individuals with GN usually have a defined time of disease onset at the time of kidney biopsy. This can help to disentangle the contribution of GN to subsequent CV risk over and above the development of reduced kidney function from chronic injury. For example, a window of opportunity for advanced study in GN patients is through careful analysis of histopathological findings from their kidney biopsy. It is not uncommon for patients with GN to undergo several biopsies throughout their life. This would allow for correlation of biopsy findings at presentation, as well as subsequent changes on biopsy (vascular, tubulointerstitial, or glomerular), with subsequent CV risk. A comprehensive approach that encompasses histopathology data, biomarkers, and vascular studies could provide fundamental insights into disease pathogenesis.
Non-Traditional Mechanisms of CV Disease in GN.

Note. CV = cardiovascular; GN = glomerulonephritis; NO = nitric oxide; CKD = chronic kidney disease; ANCA = antineutrophilic cytoplasmic antibody; FSGS = focal segmental glomerulosclerosis; IgA = immunoglobulin A; ROS = reactive oxygen species; VSMC = vascular smooth muscle cells.
Clinical Targets to Treat and Prevent CV Diseases in GN Patients
Whereas the inflammatory component of GN is likely addressed through immunosuppressive treatments that achieve disease remission, the management of traditional CV risk factors requires a separate CV risk assessment to inform the use of adjunctive cardioprotective medications.
Lifestyle Modification
Lifestyle modification should be considered for all people with GN and with risk factors for CV disease. This includes adherence to a heart healthy diet, increasing physical activity, weight loss, and smoking cessation. There are no dedicated clinical trials of lifestyle modification in people with GN but it is reasonable to anticipate that the relative benefits of lifestyle modification for reducing CV risk in the general population are generalizable to people with GN. Importantly, given that children and young adults with GN are generally at low CV risk in the absence of a family history of premature heart disease, lifestyle modifications should be considered the first-line treatment.
Hypertension
Chronic hypertension is common among people with GN. In a case series of 708 people with biopsy-proven, primary GN, the prevalence of hypertension at the time of diagnosis ranged from 44% in adults with mesangioproliferative GN to 81% in people with membranoproliferative GN. 31 In the few studies that have leveraged 24-hour ambulatory blood pressure monitors in people with GN, up to 15% of people with GN have masked hypertension and 25% of people with GN have isolated nighttime hypertension. 32 While the variability in hypertension prevalence may reflect differences in age and clinical comorbidities at the time of GN diagnosis, the pathogenesis of hypertension in GN is likely similar across etiologies and includes sodium and water retention in the context of glomerular and tubulointerstitial damage, renin-angiotensin system (RAS) upregulation due to renal ischemia and increased sympathetic system activity arising from the kidney. 33 Hypertension may also be a consequence of immunosuppressive treatments employed in the management of GN, including corticosteroids and calcineurin inhibitors, which can make management of hypertension in GN particularly challenging.
Given that people with GN are at high absolute risk for a CV event, all individuals should be considered for non-pharmacologic and pharmacologic strategies for managing hypertension. Non-pharmacologic treatments include restricting dietary sodium, increasing exercise, weight loss, and smoking cessation. Pharmacologic treatment involves the initiation of blood pressure lowering medications, among which RAS blockade with angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) are first-line treatments due to their proteinuria lowering effects. These medications should be titrated to their maximally tolerated dose and adjunctive medications, such as diuretics should be used to mitigate side effects of RAS blockade, such as hyperkalemia.
With respect to blood pressure treatment targets, currently, the guideline recommended systolic blood pressure target for adults with CKD is < 120 mmHg, which is based on the SPRINT (Systolic Blood Pressure Intervention Trial). 34 Compared with a systolic blood pressure target of < 140 mmHg, intensive systolic blood pressure lowering to a target of < 120 mmHg was associated with lower rates of the primary composite outcomes of myocardial infarction, non-myocardial infarction acute coronary syndrome, acute decompensated heart failure, stroke, and death from CV disease causes (HR = 0.81, 95% CI = 0.63-1.05). Importantly, the SPRINT study excluded people with proteinuria 1 g per day or more and people with GN on immunosuppression. However, people with GN that were not on immunosuppression were included. Although an intensive versus liberal systolic blood pressure target has yet to be formally examined in a dedicated randomized controlled trial (RCT), multiple meta-analyses have demonstrated a consistent benefit-risk profile of blood pressure lowering, regardless of baseline proteinuria.35,36 While the benefits of treating hypertension and blood pressure lowering are consistent, irrespective of the etiology of CKD or the degree of proteinuria, there is limited information regarding the impact of intensive blood pressure lowering in young adults. In children, there is even less information regarding the treatment of hypertension and the guideline recommended target is a 24-hour mean arterial pressure that is less than the 50th percentile for age, sex, and height using a 24-hour ambulatory blood pressure monitor. 37 Therefore, blood pressure lowering medication in children and young adults should be initiated after a shared decision-making process.
Hyperlipidemia
Similar to hypertension, hyperlipidemia may also be a complication of GN itself and is indeed a diagnostic criterion for nephrotic syndrome. Hyperlipidemia may also be secondary to immunosuppressive medications, such as calcineurin inhibitors or glucocorticoids. The underlying principles for the management of hyperlipidemia are also similar to hypertension. Lifestyle modification should be considered for all people with GN and with persistent hyperlipidemia. Some adults with GN may be at high absolute risk for CV disease, and statins should be considered as first-line treatment for hyperlipidemia in appropriate people, with the target dose determined based on the predicted absolute risk of CV disease. In the absence of established risk prediction tools for people with GN, the KDIGO guidelines recommend a CV risk assessment based on the totality of CV risk factors, such as lipid parameters, chronic inflammatory conditions, genetic ancestry, and sex-specific risk factors, such as pre-eclampsia and menopause. 38 Non-statin treatments, such as ezetimibe, can also be added in people intolerant of statin or who are at high CV risk and fail to achieve a reduction in their low-density lipoprotein (LDL) cholesterol by ≥50% or to normal limits, despite a statin. However, such recommendations are extrapolated data from CKD patients in general, and the benefits to control lipids to treat and prevent CV diseases were never prospectively tested in GN patients.
Sodium Glucose Co-Transporter 2 Inhibitors
Beyond targeting CV risk factors, sodium glucose co-transporter 2 inhibitors (SGLT2i) are novel reno-protective medications that have generated interest regarding the potential for CV benefits in people with GN. SGLT2i confer consistent relative risk reductions across the full spectrum of CV risk and irrespective of traditional CV risk factors, such as blood pressure, 39 glycemic control, 40 and body weight. 41 SGLT2i work by inhibiting glucose and sodium reabsorption in the proximal tubule that increases the sodium concentration within the filtrate and results in tubuloglomerular feedback at the juxtaglomerular apparatus triggering afferent arteriolar vasoconstriction. 42 This results in an initial decline in intraglomerular pressure, an elevation in creatinine and decrease in GFR. However, over the long term, there is glomerular hemodynamic adaptation and the decrease in intraglomerular pressure reduces the rate of GFR decline. Importantly, SGLT2i have been proven beneficial in people with CKD, 43 including reducing the incidence of all-cause mortality (HR = 0.87, 95% CI = 0.78-0.97), CV death or heart failure (HR = 0.74, 95% CI = 0.66-0.82), and progression of CKD (HR = 0.60, 95% CI = 0.53-0.68) as compared with placebo, without evidence of effect modification based on diabetes status. 43 SGLT2i confer particularly large reductions in the incidence of heart failure (HR = 0.68, 95% CI = 0.61-0.76). 44 They also have a small but nonetheless important effect on atherosclerotic CV disease and reduce the incidence of the composite of CV death, myocardial infarction, and stroke by 10% (HR = 0.90, 95% CI = 0.85-0.95), particularly in people with established CV disease. 44
While the benefits of SGLT2i for kidney progression have been clearly demonstrated in people with GN, the effects on CV outcomes have not been directly examined. Although people with GN were included in the kidney outcome RCTs and a pre-specified subgroup analysis in IgA nephropathy demonstrated compelling evidence of renal benefit, 45 there were too few participants to specifically study CV outcomes. Nonetheless, SGLT2i may be readily used in people with GN who have an alternate indication for the medication, such as concomitant type 2 diabetes. Likewise, the utility for SGLT2i for reducing CKD progression may also be a pathway to cardioprotective benefits, given that advanced CKD in-and-of-itself contributes to CV disease.
However, the use of SGLT2i for primary prevention of CV disease in people with an isolated diagnosis of GN will require further study, including consideration for potential differences in efficacy related to the pathophysiology of GN. For instance, in a small mechanistic study of people with FSGS, use of SGLT2i did not alter renal hemodynamic function or reduce proteinuria, possibly due to decreased SGLT2 receptor expression in FSGS. 46 Herein also lies an important barrier to ultimately preventing CV disease in people with GN. Despite knowledge of the clinical factors contributing to CV disease in GN, the overarching challenge continues to be the lack of risk prediction models to identify people with GN who would benefit from cardioprotective medications and the lack of direct evidence regarding the CV efficacy of treatments targeting traditional and non-traditional risk factors. This lack of evidence is further compounded by methodological challenges related to conducting RCTs in GN, including the relative rarity of GN compared with other causes of CKD, the slow but progressive nature of GN and the relative underfunding of research in GN. 38 This means that the benefit/risk profile of initiating new medications to prevent CV disease in people with GN remains unclear and will likely require multinational collaborative efforts to advance this clinically important question.
Antiplatelet Treatment
Although antiplatelet therapies are indicated in the secondary prevention of CV disease, there is little evidence to support their use for the primary prevention of CV disease, in large part because any cardioprotective benefit from antiplatelets are largely counterbalanced by an increased risk of bleeding. 47 Although people with specific subtypes of GN may have more risk for hypercoagulability, there have been no dedicated studies of antiplatelet treatment in people with GN for CV disease prevention. Given the risks of bleeding, empirical use of antiplatelets for primary prevention cannot be recommended in the absence of dedicated clinical trials.
Emerging Treatments for CV Disease
Beyond SGLT2i, other novel treatments, such as glucagon-like peptide 1 (GLP-1) receptor agonists are emerging as important adjunctive cardioprotective medications in people with CKD. Endogenous GLP1 is an incretin hormone that is produced in the intestinal L cells via receptors in pancreatic beta cells in response to food intake, and results in an insulinotropic response. 48 Due to the presence of GLP1 receptors in extra-pancreatic tissues such as the brain, heart, kidneys, and vasculature, GLP1 receptor agonists have been shown to have other beneficial effects. Specific to CV disease, GLP1 receptor agonists reduce the incidence of the composite of CV death, myocardial infarction, or stroke, versus placebo, with consistent effects in people with and without diabetes.49,50 GLP1 receptor agonists are recommended in people with diabetes at high CV risk, including people with CKD. 51 Guidelines have yet to be updated to include the more recent evidence in people without diabetes. There is little evidence regarding the effects of GLP1 receptor agonists in people with GN and there are no forthcoming clinical trials. Given their favorable benefit-risk profile, these medications may be considered for high-risk patients.
Non-steroidal mineralocorticoid receptor antagonists (nsMRAs), namely, finerenone, have also emerged as important adjunctive treatments for preventing CV disease in people with CKD and diabetes. 52 Non-steroidal mineralocorticoid receptor antagonist has a distinct chemical structure compared with steroidal mineralocorticoid receptor antagonists (sMRAs), such as spironolactone, thereby resulting in nsMRAs having more selectivity for the mineralocorticoid receptor and less side effects. 53 The role of nsMRAs in people with non-diabetic CKD and in people with GN remains to be clarified.
Glomerular Disease and CV Risk in Children
Glomerulopathies present both acute and chronic complications in children. Initial considerations are around the degree of renal involvement with subsequent determination of glomerular filtration rate, as well as managing hyperkalemia, and fluid overload. Longer-term complications include chronicity associated with relapsing disease, as well as medication side effects. Furthermore, these children affected by glomerulopathies may have traditional risk factors for CV disease, while others have both traditional and non-traditional risk factors. 54 Traditional risk factors for CV disease in children include obesity, metabolic syndrome, dyslipidemia, as well as pre-existing hypertension. Non-traditional CV disease risk is often associated with proteinuria, or degree of renal involvement, exposure to second-hand smoking, or first-hand exposure, as well as prematurity that is associated with lower nephron mass. 54
In a Cure Glomerulonephritis (CureGN) study by Ashoor et al, 54 761 children with glomerulopathies (283 with MCD, 177 with FSGS, 36 with MN, and 265 with IgA) were enrolled at median 16 months from glomerular disease origin and assessed for traditional and non-traditional CV disease risk factors. Importantly, several traditional CV disease risk factors were identified in this patient population, including, 21% of children having hypertension, 51% being overweight or obese, and 71% having dyslipidemia. Non-traditional risk factors included exposure to second-hand smoke, which was observed in 24% of children enrolled. Furthermore, 12% were born premature (as defined by < 37 weeks of gestation at delivery).
Another important study by Shah et al, 55 looked at associations between obesity and CV disease risk factors. They used the Nephrotic Syndrome Study Network (NEPTUNE) cohort and prospectively analyzed 541 patients. The prevalence of obesity in the pediatric arm of this cohort was 38%, and obesity over time was associated with higher systolic blood pressure index and hypertension. Furthermore, obesity was associated with a lower likelihood of achieving complete remission of proteinuria. 55 Thus, it is apparent that increased focus must be placed on targeting weight management in children with glomerular disease as hypertension and proteinuria are both independent risk factors for CV disease.
The above important studies also revealed that children with glomerular disease, particularly MCD, had infrequent monitoring for dyslipidemia and were less likely to be offered lipid-lowering treatment. 54 In addition, a recent study in children with IgA nephropathy showed that those with dyslipidemia may have a lower probability of renal survival, 56 highlighting the urgent need for diagnosis and management of these common sequelae associated with glomerular disease. In the Ashoor study, another important factor noted was that up to 14% of children with hypertension were not being treated, 54 thus contributing further to their CV disease risk burden.
A recent area of intense research interest is on legacy effects of pediatric disease and CV disease risk factors on adult CV disease outcomes.57 -59 In a study by Jacobs et al, 57 the HR for fatal CV events was elevated in those participants who smoked as a youth (HR = 1.61, 95% CI = 1.21-2.13), who were obese as a youth (HR = 1.44, 95% CI = 1.33-1.57), who had elevated cholesterol (HR = 1.30, 95% CI = 1.14-1.47) or triglycerides (HR = 1.50, 95% CI = 1.33-1.70), and for those with elevated systolic blood pressure (HR = 1.34, 95% CI = 1.19-1.50). In addition, children with glomerulopathies are exposed, in most cases, to high-dose steroids, which lead to obesity, dyslipidemia, glucose intolerance, and frank diabetes, as well as hypertension.
These studies reveal an unmet need in pediatric glomerular disease. An increased focus needs to be on identifying children with glomerulopathy who have modifiable risk factors for CV disease and intervening early and effectively. Importantly, the first choice for intervention would be lifestyle modification, including increased exercise and dietary counseling. Pharmacological intervention must only be initiated after careful shared decision-making with the child or youth and their caregivers while weighing the risks versus the benefits. In certain instances, particularly patients with proteinuria refractory to therapy, renin-angiotensin-aldosterone (RAS) blockade and statins are cautiously employed. However, there is evidence to suggest they may be under-prescribed in dyslipidemic children with GN. 54 It is therefore clear that large, collaborative studies are paramount to address these key issues for children with glomerular disease.
Conclusion
It is clear that CV disease risk is elevated in patients with GN; however, there are few studies directly investigating GN patients and their CV disease risk. Much of our practice is an extrapolation from patients with CKD. Dedicated epidemiological, basic science, and translational studies with multicenter collaboration will be needed to address the evidence gaps in the prevention and targeted management of CV disease in people with different forms of GN across the age spectrum. Of equal importance is effective engagement with patient partners and those with lived experience to prioritize research questions, inform the feasibility of study designs and ensure that the needs of patients with GN are being met. 60
Footnotes
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
All authors provided consent for publication.
Availability of Data and Materials
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.