
Abstract
Purpose of Program:
Glomerulonephritis (GN) is a group of rare kidney diseases that is increasingly being managed with higher cost immunosuppressive (IS) agents in Canada. Ontario Health’s Ontario Renal Network (ORN) oversees the management and delivery of GN services in the province. Stakeholder surveys previously conducted by ORN identified that both clinicians and patients do not perceive access to GN medications as comprehensive or timely. The program conducted a focused jurisdictional scan among 7 provinces to inform ORN initiatives to improve access to GN medications. Specifically, the program examined clinician experience with GN access, public drug coverage criteria, and timelines for public coverage for select IS agents (ie, tacrolimus, cyclosporine, mycophenolate mofetil [MMF], mycophenolate sodium, rituximab, and eculizumab) used to manage GN in adults who live in Canada.
Methods:
For the selected IS agents, a focused jurisdictional scan on medication access was conducted by ORN in 2018 and updated in July 2022. Information was obtained by searching the gray literature and/or credible online sources for public funding policies and eligibility criteria. Findings were supplemented by personal communications with provincial drug programs and consulting GN clinical experts from 7 provinces (ie, Alberta, British Columbia, Saskatchewan, Manitoba, Ontario, Nova Scotia, and Quebec).
Key Findings:
Clinicians from different provinces prescribe IS agents similarly for GN indications, despite distinctions in public drug funding policies. While patients can obtain public funding for many IS agents, for GN, most provinces rely on case-by-case review processes. In addition, provinces can vary in their funding criteria and which IS agents are listed on the public formulary. For IS agents that require prior authorization or case-by-case review, timelines vary by province with decisions taking a few days to weeks. British Columbia, with a GN-specific drug formulary, had the most integrated and efficient system for patients and prescribers.
Limitations:
This scan primarily relied on publicly available information for drug coverage criteria and clinician experience with access in their province. Since this scan was conducted, public drug coverage criteria and/or application processes may have changed.
Implications:
While patients in most provinces have similar needs and nephrologists similar prescribing patterns, gaps still exist for publicly funded GN medications. Interprovincial differences in the drugs funded, funding criteria, and application process may affect timely and equitable access to GN medications across Canada. Given the rarity of GN, a pan-Canadian funding approach may be warranted to improve the current state.
Program Description and Objectives
Glomerulonephritis (GN) refers to a rare, heterogeneous group of kidney diseases that cause progressive kidney damage due to inflammation in the glomeruli. 1 Depending on the type of GN, the worldwide incidence ranges from 0.2 to 2.5/100 000 person years. 2 Despite being considered a rare disease, an estimated 10% of incident kidney failure is attributed to GN, and this increases to 17% to 26% for prevalent patients in Canadian provinces and territories. 3 Furthermore, GN often affects otherwise healthy young adults, resulting in devastating consequences for the affected individuals. While the management of GN varies depending on the type of disease, immunosuppressive (IS) therapy with agents such as corticosteroids, calcineurin inhibitors, antimetabolites and biologics (eg, rituximab) is the cornerstone of treatment.1,4-6 The primary goals of care are to prevent or slow progression to kidney failure and improve or maintain the patient’s quality of life. 6 Failure to prevent progression to kidney failure can result in the use of kidney replacement therapies (eg, dialysis) that are associated with poorer patient outcomes and significant health care system costs.3,7
Canada as a federation is governed by an act (Canada Health Act of 1984) assigning roles for health care delivery that are divided among federal, provincial, and territorial governments.8-10 Kidney care delivery is primarily overseen by provincial/territorial governments. Each province and territory has a distinct structure for coordinating kidney care delivery in general (eg, British Columbia has BC Renal, Alberta has Alberta Kidney Care North and South, Ontario has Ontario Renal Network [ORN]).11-13 Similarly, prescription drug coverage is mostly managed at the provincial/territorial level wherein there are variable approaches to covering GN medications. At the federal level, there are specific programs for select patient populations that cover health services, including the costs of prescription drugs (eg, noninsured health benefits [NIHB]). 14
Given only a minority of patients with GN can be managed with low-cost IS agents (eg, prednisone, cyclophosphamide), there is increasing use of other more costly agents (eg, calcineurin inhibitors, mycophenolate, rituximab, eculizumab) that have better efficacy and preferable side effect profiles.6,15 In Canada, patients are faced with navigating a variety of sources for drug coverage, including public programs at the provincial or federal level, private insurance, or individuals paying out-of-pocket. 16 Intravenous medications given in outpatient hospital clinics (eg, intravenous cyclophosphamide, rituximab) may be covered through a hospital’s global budget. In addition, pharmaceutical manufacturers may offer financial assistance to fully or partially cover drug costs. Overall, the system is complex.
Ontario Health’s ORN oversees management and delivery of kidney care services in the province of Ontario. While ORN does not fund medications for GN, they advise the government on strategies to address access issues. Stakeholder surveys previously conducted by ORN identified that both clinicians and patients do not perceive access to drugs to treat GN as comprehensive or timely. 17 To inform initiatives on improving access, ORN undertook a jurisdictional scan to examine current access, extent of public coverage, and timelines for public coverage in Canadian provinces for adults who are prescribed IS agents for GN.
Methods
This scan focused on determining funding sources (eg, public drug plan, private insurance, hospital formulary), public drug coverage criteria, and timelines to access public drug coverage for IS agents used to treat adults with GN conditions. The following IS agents were included: calcineurin inhibitors (tacrolimus, cyclosporine), mycophenolate mofetil (MMF), mycophenolate sodium, and the biologics (rituximab, eculizumab) (Supplementary Appendix Table 1.0). For the purpose of this scan, GN conditions included any of the following: ANCA-associated vasculitis (granulomatosis with polyangiitis [GPA]/microscopic polyangiitis [MPA]), anti-glomerular basement membrane (anti-GBM) antibody disease, atypical hemolytic uremic syndrome (aHUS), C3 glomerulonephritis (C3GN), immunoglobulin A (IgA) nephropathy, focal segmental glomerulosclerosis (FSGS), lupus nephritis, minimal change disease (MCD), membranous nephropathy (MN), or membranoproliferative glomerulonephritis (MPGN).
Public drug plans provide coverage for drugs under various programs and can be accessed as an unrestricted benefit or a restricted benefit. 18 For the purpose of this jurisdictional scan, the following descriptions were used to define the drug’s coverage status under a public plan:
Unrestricted benefit: Drug is listed on the drug plan’s formulary and is funded for any therapeutic use. Patients do not need to meet any clinical criteria to obtain coverage. Terms used by drug plans to refer to this listing include “general benefit,” “open benefit,” and “regular benefit.” 18
Limited use: Patient must meet specific criteria for drug coverage. Prescribers may write a prespecified code on the prescription (“reason for use code,” “limited use code,” etc.). 18
Prior authorization: The drug is listed as a restricted benefit on the drug plan. The patient must meet specific clinical criteria to be eligible for coverage. Prescribers need to submit a prior approval request on behalf of their patient. Terms used by drug plans to describe this listing include “prior authorization,” “exception drug status,” “exceptional access program,” and “special authorization.” 18
Case-by-case: Drug is not listed as a benefit on the drug plan. Drug plan will consider funding a given drug and indication based on individual patient clinical circumstances and program-specific criteria (level of evidence, availability of other treatment options, etc.). Prescribers must submit a patient-specific application for funding consideration.
This scan did not examine the funding criteria for the pediatric population, older therapies (eg, azathioprine, prednisone, and oral cyclophosphamide), or supportive care drugs (eg, anti-infectives, osteoporosis drugs, and anti-hypertensive agents).
Data Sources and Collation
Information for this jurisdictional scan was obtained by searching the gray literature and/or credible online sources for provincial funding criteria and policies, which included scanning drug formulary listings on provincial or provincial agency websites. Findings were supplemented with personal communications with provincial drug programs and consultations with GN clinicians (nephrologists and pharmacists) who practice in Canada. Experts were identified based on their geographical location and years of expertise in providing GN care. Ultimately, 12 GN care providers who routinely manage a large volume of GN patients in their practice were consulted on medication access to specific IS agents by indication and in their respective jurisdiction (2-Alberta, 2-British Columbia, 2-Manitoba, 2-Nova Scotia, 2-Ontario, 1-Saskatchewan, and 1-Quebec). Initial consultations occurred by telephone or email between October and December 2018. For both methods, a standard set of consultation questions was used to confirm medication access and public funding criteria. Subsequently, after reviewing a draft report, experts were invited to provide any updates to reflect the medication access landscape in their respective jurisdictions as of July 2022.
Key Findings
Provincial Comparison of GN Formularies
Experts consulted reported that patients often rely on existing provincial and federal drug plans for prescription drugs. In addition, eligible First Nations and Inuit persons can apply for coverage through the NIHB program for specific GN medications that are not otherwise covered through private or provincial/territorial plans. 19
As shown in Table 1, only British Columbia has a separate formulary for GN medications where drug costs are 100% covered by BC Renal, the organization that oversees all of kidney care in the province. In other provinces, government plans cover a portion of the drug costs and patients may need to pay a co-payment or deductible out-of-pocket. Out-of-pocket charges can lead to financial hardship for patients as well as the inability to access necessary medications. 20
Overview of Public Drug Plan Options for GN Medications.
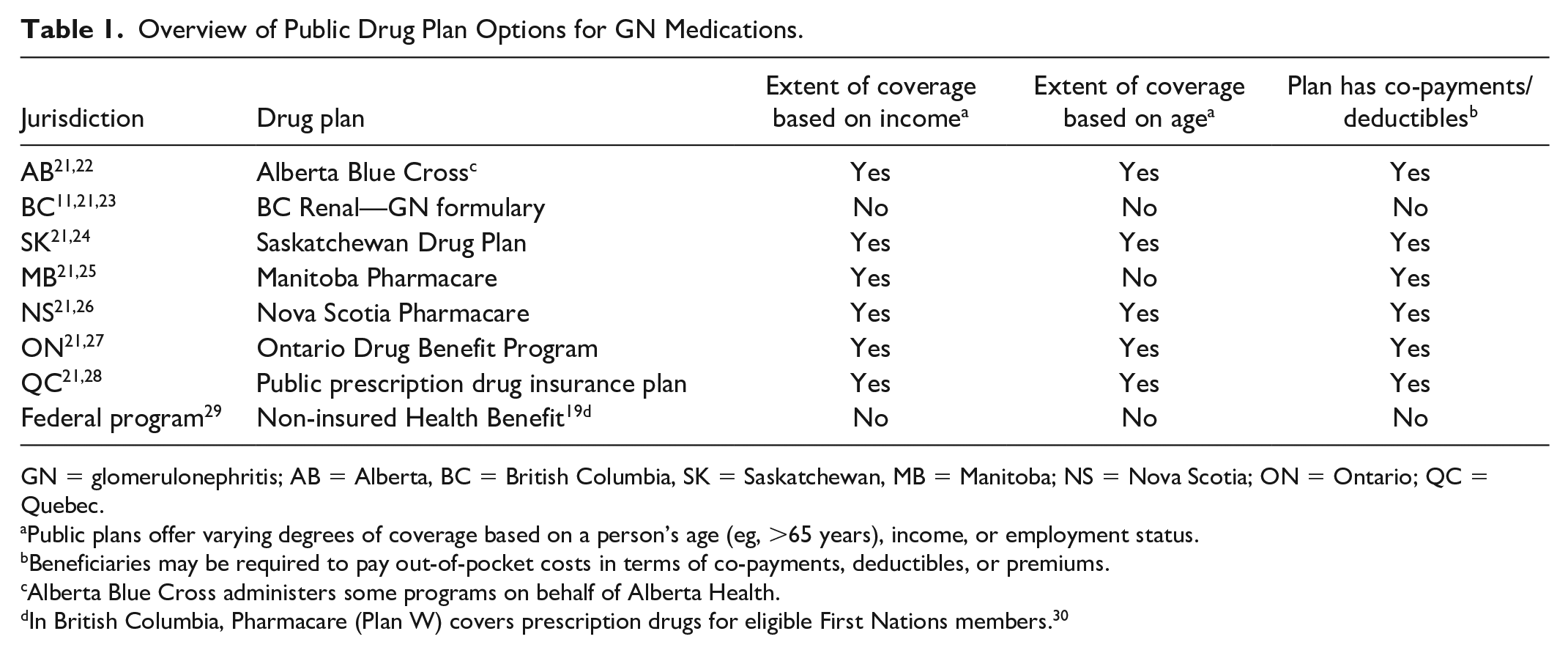
GN = glomerulonephritis; AB = Alberta, BC = British Columbia, SK = Saskatchewan, MB = Manitoba; NS = Nova Scotia; ON = Ontario; QC = Quebec.
Public plans offer varying degrees of coverage based on a person’s age (eg, >65 years), income, or employment status.
Beneficiaries may be required to pay out-of-pocket costs in terms of co-payments, deductibles, or premiums.
Alberta Blue Cross administers some programs on behalf of Alberta Health.
In British Columbia, Pharmacare (Plan W) covers prescription drugs for eligible First Nations members. 30
Cyclosporine
Experts consulted from most provinces prescribed cyclosporine for the treatment of FSGS (with nephrotic syndrome), MCD, MN, and lupus nephritis. In BC, Quebec, and Nova Scotia, cyclosporine is publicly funded as an unrestricted benefit and could be prescribed for any GN disease. Experts from Nova Scotia reported that it is not often prescribed for GN in that province.31-33 In Alberta and Saskatchewan, cyclosporine is publicly funded with prior approval for FSGS, IgA nephropathy, MCD, MN, and lupus nephritis. In Alberta, patients must be steroid-dependent or steroid-resistant. Saskatchewan does not require patients to have trialed steroids or cyclophosphamide. Previously, in Ontario, patients must have tried or could not use cyclophosphamide and/or prednisone to be eligible for public funding for nephrotic syndrome.34,35 In June 2021, Ontario transitioned cyclosporine from requiring prior authorization to an unrestricted benefit, which increased patient access (Supplementary Appendix 1 Table 2.0; Supplementary Appendix 2).
Tacrolimus
Experts consulted from all provinces prescribed tacrolimus for FSGS (with nephrotic syndrome), MCD, and MN. Experts from a few provinces prescribed tacrolimus for lupus nephritis. In Ontario, tacrolimus is the preferred calcineurin inhibitor for patients who are pregnant. 36 In, Saskatchewan, Manitoba, Ontario, and Nova Scotia, tacrolimus is publicly funded through case-by-case review processes. It is an unrestricted benefit in British Columbia and Quebec.31,33 Ontario and Nova Scotia reported using the manufacturer’s access program to obtain drug coverage for their patients. In Alberta, the public payer considers tacrolimus and cyclosporine to be equivalent so only cyclosporine is publicly funded (Supplementary Appendix 1 Table 3.0). Of note, British Columbia initially funded tacrolimus only in patients who had an intolerance or contraindication to cyclosporine. However, with the availability of a less costly generic alternative, their GN network removed this funding condition. A switching study was conducted and found no clinically meaningful differences between brand and generic tacrolimus. 23
Mycophenolate
Experts from most provinces prescribed MMF for lupus nephritis, FSGS (with nephrotic syndrome), MCD, MPGN/C3GN, and IgA nephropathy. In British Columbia, Quebec, and Manitoba, MMF is an unrestricted benefit, whereas in Alberta and Nova Scotia case-by-case review is required for public funding.21,31,33 In Saskatchewan, MMF funding can be obtained through their prior authorization program for patients with nephrotic syndrome. According to current funding criteria, patients must have biopsy-proven evidence of severe proliferative lesions or sclerosis and have not responded to a 6-month course of cyclophosphamide or are unable to tolerate cyclophosphamide. 34 For patients without nephrotic syndrome, MMF funding is considered on a case-by-case basis (Supplementary Appendix 1 Table 4.0). Ontario was the only jurisdiction where mycophenolate sodium (brand: Myfortic) was preferentially prescribed over MMF. Mycophenolate mofetil required case-by-case review while mycophenolate sodium was funded as a general benefit. In other provinces, patients must demonstrate gastrointestinal intolerability with MMF prior to being considered for coverage for Myfortic. In 2019, Ontario transitioned MMF to a general benefit. 37
Rituximab
Experts from all provinces prescribed rituximab for ANCA-associated vasculitis (induction or maintenance therapy for GPA/MPA) and membranous nephropathy (MN). Other indications may include steroid-dependent FSGS (with nephrotic syndrome), MCD, MPGN/C3GN, and less commonly other types of GN such as lupus nephritis or cryoglobulinemia. These indications typically require case-by-case review for public funding.
Rituximab is approved by Health Canada for induction therapy for ANCA-associated vasculitis, while maintenance therapy remains an off-label use, potentially contributing to variability in coverage across Canada. In most provinces, there are established public funding criteria for GPA/MPA for induction therapy for which the prescriber must seek prior approval. For induction treatment, provinces have similar eligibility criteria. Criteria generally stipulate that patients must have failed prior cyclophosphamide treatment, had an intolerance or contraindication to cyclophosphamide, or have reached the recommended cumulative dose.32,34,35,38-41 Other criteria can differ between provinces. For example, while some provinces state that patients must have “failed an adequate trial of cyclophosphamide,” Alberta and Ontario quantify a minimum trial of 6 IV cyclophosphamide pulses or failed 3 months of oral cyclophosphamide.34,38,40-42 For maintenance therapy, British Columbia and Ontario have established funding criteria. Since 2020, Ontario lists biosimilars to Rituxan (rituximab) for GPA/MPA as a limited use benefit on the formulary for both induction and maintenance therapy so prescribers no longer need to seek prior approval. 41 In Alberta, rituximab maintenance therapy can be accessed via their case-by-case review program.
For PLA2R-associated MN, 3 provinces have specific criteria for rituximab funding. British Columbia funds second-line use after a trial of calcineurin inhibitors. 39 Manitoba will consider paying for rituximab in the first-line setting for patients of child-bearing age or those who have risk factors for malignancy and for progression. They will also cover rituximab for patients with risk factors for progression who have failed or were intolerant to first-line therapy (eg, Ponticelli regimen). 40 In 2022, Ontario transitioned rituximab for MN from case-by-case review to a restricted benefit requiring prior authorization. These criteria granted funding of rituximab for a subset of adult patients defined as those with greater than 5 g of proteinuria despite 6 months of conservative therapy with renin angiotensin inhibitors. It can be given sooner if the patient has greater than 8 g of proteinuria, anti-PLA2R titer greater than 50 RU/mL, or a glomerular filtration rate (GFR) less than 60 mL/min. Patients who recur post-transplantation can also access rituximab. 43 In Alberta, public funding is available, on a case-by-case basis, for patients who have contraindications or failed other clinical alternatives (Supplementary Appendix 1 Table 5.0; Supplementary Appendix 3).
Since 2019, Health Canada has approved multiple biosimilars to the reference biologic Rituxan (rituximab). Provinces vary in which biosimilar products they cover and for which indications. In Quebec, for example, rituximab biosimilars for the treatment of GN are funded by the hospital’s global budget if given in outpatient hospital clinics. The extent of coverage varies from one hospital to the other. Well-established uses (GPA or MPA) are consistently funded throughout the province, with a required prior authorization if covered through the provincial plan (RAMQ). 33 For other uses (eg, MCD, MN), hospitals or the RAMQ may fund on a case-by-case basis. Experts from Alberta reported that their patients who access rituximab via private insurance still may face significant out-of-pocket costs for co-payments (eg, 20%) associated with private plans. Patients living in other provinces face similar out-of-pocket costs if paying by private means, hampering medication access.
Eculizumab
Experts from most provinces identified atypical hemolytic uremic syndrome (aHUS) as the main GN-related use of eculizumab. Some provinces (eg, Alberta, BC, Manitoba, Ontario, and Quebec) reported clinician interest in using eculizumab for treating other types of GN (eg, C3GN and refractory MPGN) and Manitoba may approve it for C3GN in select cases. Patients may also seek private insurance coverage or compassionate supply from the pharmaceutical manufacturer for indications that are not Health Canada–approved.
Overall, most provinces fund eculizumab on a case-by-case basis. Only Ontario has established funding criteria for aHUS that require prior authorization. Patients with a confirmed diagnosis of aHUS who meet the eligibility criteria can be approved for an initial period of 6 months. 43 In Alberta, eculizumab for aHUS can be accessed via the Short Term Exceptional Drug Therapy (STEDT). This is a case-by-case program for high-cost nonformulary drugs where other treatments must have been tried or were contraindicated. For eculizumab, patients must meet specific clinical criteria. 44 In British Columbia, eculizumab funding requests for aHUS have been considered through the Expensive Drugs for Rare Diseases (EDRD) program. A multidisciplinary expert committee reviews each request and considers the following factors: disease severity, availability of other treatment options, and clinical effectiveness of the requested drug 45 (Supplementary Appendix 1 Table 6.0, Supplementary Appendix 4).
Turnaround Times
Public funding for many of the GN indications requires prior approval through a formal prior authorization program or on a case-by-case basis. Usually, turnaround times are not publicly reported by provincial drug programs. Experts from several provinces reported that decisions on prior authorization requests may come back to the prescribers in under a week. For drug funding requests requiring case-by-case review, turnaround times range from a few business days to a month. Turnaround times may vary depending on the drug and indication requested, the availability of provincially approved reimbursement criteria, and the clinical complexity of the request. Ontario experts noted that there are frequent requests for additional information, which can significantly prolong the time to approval.
Discussion
In Canada, each province and territory is responsible for designing and administering their own drug plans for prescription drugs.21-28 In the absence of a universal drug coverage model, Canada has a patchwork system for prescription drug coverage where patients rely on a mix of public plans and private funding for medication access. 29 Differences in clinician experiences of medication access across Canada may be due to the authority held by provinces and territories to make public drug funding decisions.
Public spending in Canada on prescription drugs has been significantly increasing with $16.2 billion spent on prescription drugs in 2021. 46 To ensure value for money under public drug plans and better alignment among provincial, territorial, and federal drug plans, a pan-Canadian review process is used for many new, and often high cost, medications (eg, eculizumab, rituximab).47-49 Generally, pharmaceutical manufacturers will seek regulatory approval from Health Canada who will assess the drug’s efficacy, safety, and quality. The Canadian Agency for Drugs and Technologies in Health (CADTH) or Quebec’s Institut national d’excellence en santé et en services sociaux (INESS) will evaluate a new drug’s clinical and cost-effectiveness compared with current standard of care interventions and make a reimbursement recommendation. 50 For positive funding recommendations, the pan-Canadian Pharmaceutical Alliance conducts pricing negotiations with the manufacturer on behalf of the participating provinces and territories. Each province and territory will then make their own funding decisions. 51 Rituximab for GPA/MPA was reviewed through this type of process and was subsequently listed on many of the provincial formularies. 52
Overall, the findings of this jurisdictional scan suggest that IS agents are likely prescribed for similar indications across the country. However, there are interprovincial differences in drug plan design, public funding criteria, and time to access. For example, British Columbia was the only province with a GN-specific drug formulary, while some provinces have case-by-case review processes or other provinces have more formalized case-by-case review programs like Alberta’s STEDT Program or Ontario’s Exceptional Access Program’s Compassionate Review Policy.53,54
For some drugs, the benefit status for the same drug and indication varies between provinces (eg, the same drug and indication may require prior approval in one province but is an unrestricted benefit in another province). Where explicit funding criteria are established (eg, Rituximab for GPA/MPA, mycophenolate for nephrotic syndrome), the criteria can vary. Prior analyses have found that public plans across Canada are even less well aligned for high-cost drugs. 55 For patients, these differences may mean that they are left without drug coverage for previously covered therapies when moving between provinces.
In terms of interprovincial differences in decision timelines, contributing factors may include differences in program structure, application procedures, and request volumes. British Columbia had the most integrated prescribing and the most efficient model for GN medication access. In 2013, the BC GN Network developed a GN-specific registry and drug formulary. Patients who are registered can access oral immunosuppressants (eg, cyclosporine, tacrolimus, MMF) for any GN-related indication. These medications must be from a specific private pharmacy and mailed to the patient’s home.15,23 As the dispensing of oral drugs (eg, cyclosporine, tacrolimus) is tied to reimbursement at the pharmacy level, approvals are immediate.
In this scan, we also found that public funding criteria may not align with recent clinical guidelines that could impact prescribing practices. For example, clinical guidelines recommend similar GN indications for tacrolimus and cyclosporine given they are both calcineurin inhibitors. 6 British Columbia will pay for either cyclosporine or tacrolimus on their GN formulary. 31 In other provinces, cyclosporine may be the only calcineurin inhibitor listed on the provincial formulary. For MMF, Saskatchewan’s public funding criteria require biopsy data, a criterion that conflicts with guideline recommendations by Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guidelines for the management of glomerular disease. 6 In addition, the KDIGO guidelines recommend either the use of cyclophosphamide (in combination with glucocorticoids) or rituximab as initial therapy for patients with newly diagnosed ANCA-associated vasculitis. 6 For rituximab funding, most provinces still require prescribers to indicate whether patients have tried cyclophosphamide or have a contraindication. Prolonged mandated cyclophosphamide trial periods can jeopardize patient outcomes. 6
Of note in this scan were the number of GN medications and indications that are “off-formulary” and require prescribers to submit applications for a case-by-case funding consideration, which further prolongs time to access for patients. This finding may reflect challenges in public funding for drugs for rare diseases like GN. In a public system faced with rising health care costs, public payers can be challenged to pay for expensive therapies with limited evidence as can be the case with drugs for rare diseases.56,57 As previously mentioned for drugs to be added to public formularies, there needs to be robust clinical and cost-effectiveness data. As such, public funding approval can be hampered for rare diseases wherein there is limited evidence and/or uncertainty in magnitude of the clinical benefit. 18 Furthermore, pharmaceutical manufacturers are less likely to file for regulatory approval when the market is perceived to be too small, and the CADTH reimbursement review process is primarily for drugs with Health Canada–approved indications. 50 Many GN medications are used for unapproved indications (eg, rituximab for MCD, lupus nephritis). For GN medications and indications that have established funding criteria, public payers may lack timely processes to update criteria to keep abreast with clinical practice. Funding criteria are often closely aligned with the eligibility criteria in the drug’s pivotal clinical trials. As evidence and clinical practice evolves, these criteria may become out of date. In some cases, as lower cost generic equivalents become available (eg, mycophenolate, cyclosporine), provinces transition these medications to a restricted benefit listing that gives prescribers more flexibility to align with evolving clinical practices.37,58,59
Limitations
Information for this scan primarily relied upon publicly available drug coverage criteria. However, given the number of off-label GN medications accessed by case-by-case processes, we also relied on responses by GN care providers. Their responses are subject to recall bias as well as potential negativity or positivity biases based on their previous interactions with funding bodies. Drug coverage criteria and application processes may have changed since our scan was undertaken. Furthermore, GN experts consulted were primary GN specialists and may not have reflected access issues experienced by community nephrologists and patients living in small or remote provinces/territories. However, the complexity surrounding access is likely to have an even greater impact in community settings. Irrespective, our scan is an initial step to better understand medication access for management of GN in Canada. A further in-depth study with quantitative input, reflecting both approvals and denials, from all provinces and territories and different provider types is warranted.
Implications
This is the first environmental scan to describe medication access to GN medications in Canada. Collectively, our findings suggest that medication access for treating GN is challenging in most provinces. Interprovincial differences in public funding processes and policies may worsen as newer, more expensive treatment options become available on the market and approved for GN use. Health care administrators may need to consider pan-Canadian approaches to ensure patients have equitable and timely access to imperative therapies regardless of where they reside in Canada as delays can be detrimental to both the patient and the system. Collaborative research efforts remain necessary to provide the efficacy data required to support decisions for drug coverage. Finally, informed prescribing is the duty of all nephrologists, reaching out for guidance managing rare glomerular diseases when required.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581231190227 – Supplemental material for Focused Jurisdictional Scan of Glomerulonephritis Medication Access in Canada: A Program Report
Supplemental material, sj-docx-1-cjk-10.1177_20543581231190227 for Focused Jurisdictional Scan of Glomerulonephritis Medication Access in Canada: A Program Report by Rohini Naipaul, Catherine Marques, Jenny Ng, Sean Barbour, Clifford Lo, Ainslie M. Hildebrand, Valerie Siu, Bhanu Prasad, Louis-Philippe Laurin, Lori D. Wazny, Sean Armstrong, Jaclyn Tran, Maneka Sheffield, Arenn Jauhal and Michelle A. Hladunewich in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
All authors thank Arrti A. Bhasin, PhD candidate, for her assistance with the manuscript revisions.
Ethics Approval and Consent to Participate
Ontario Health is designated a “prescribed entity” for the purposes of section 45(1) of the Personal Health Information Protection Act of 2004. As a prescribed entity, Ontario Health is authorized to collect personal health information from health information custodians without the consent of the patient, and to use such personal health information for the purpose of analysis or compiling statistical information with respect to the management, evaluation, or monitoring of the allocation of resources to or planning for all or part of the health system, including the delivery of services. Because this study is in compliance with privacy regulations, ethics review was not required.
Consent for Publication
All authors consent to the publication of this study.
Availability of Data and Materials
The data and materials are not available for this study.
Authors’ Note
The opinions, results, view, and conclusions reported in this publication are those of the authors and do not necessarily reflect those of Ontario Health (Ontario Renal Network). No endorsement by Ontario Health (Ontario Renal Network) is intended or should be inferred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.