
Abstract
Background:
Updates to the Kidney Disease Outcomes Quality Initiative Clinical Practice Guideline for Vascular Access emphasize the “right access, in the right patient, at the right time, for the right reasons.” Although this implies a collaborative approach, little is known about how patients, their caregivers, and health care providers engage in vascular access (VA) decision-making.
Objective:
To explore how the perspectives of patients receiving hemodialysis, their caregivers, and hemodialysis care team align and diverge in relation to VA selection.
Design:
Qualitative descriptive study.
Setting:
Five outpatient hemodialysis centers in Calgary, Alberta.
Participants:
Our purposive sample included 19 patients receiving maintenance hemodialysis, 2 caregivers, and 21 health care providers (7 hemodialysis nurses, 6 VA nurses, and 8 nephrologists).
Methods:
We conducted semi-structured interviews with consenting participants. Using an inductive thematic analysis approach, we coded transcripts in duplicate and characterized themes addressing our research objective.
Results:
While participants across roles shared some perspectives related to VA decision-making, we identified areas where views diverged. Areas of alignment included (1) optimizing patient preparedness—acknowledging decisional readiness and timing, and (2) value placed on trusting relationships with the kidney care team—respecting decisional autonomy with guidance. Perspectives diverged in the following aspects: (1) differing VA priorities and preferences—patients’ emphasis on minimizing disruptions to normalcy contrasted with providers’ preferences for fistulas and optimizing biomedical parameters of dialysis; (2) influence of personal and peer experience—patients preferred pragmatic, experiential knowledge, whereas providers emphasized informational credibility; and (3) endpoints for VA review—reassessment of VA decisions was prompted by access dissatisfaction for patients and a medical imperative to achieve a functioning access for health care providers.
Limitations:
Participation was limited to individuals comfortable communicating in English and from urban, in-center hemodialysis units. Few informal caregivers of people receiving hemodialysis and younger patients participated in this study.
Conclusions:
Although patients, caregivers, and healthcare providers share perspectives on important aspects of VA decisions, conflicting priorities and preferences may impact the decisional outcome. Findings highlight opportunities to bridge knowledge and readiness gaps and integrate shared decision-making in the VA selection process.
Introduction
More than 2.5 million people worldwide receive kidney replacement therapy as life-sustaining treatment for kidney failure, and this number is expected to double by 2030.1,2 As the most common form of kidney replacement therapy, hemodialysis requires a safe, reliable mechanism to access the bloodstream, termed vascular access (VA). 3 Historically, arteriovenous fistulas were recommended as first-line VA due to lower complication rates and mortality than its alternatives, arteriovenous grafts or central venous catheters, reported in observational studies.4-6 Vascular access selection has been largely driven by patients’ eligibility for an arteriovenous fistula, although contemporary data suggesting access type alone does not explain the difference in observed outcomes have challenged the “fistula first” approach.7-9 As one VA type is not clearly superior under all circumstances, health care providers and patients are increasingly engaging in individualized approaches to VA selection.10,11
Shared decision-making is recommended as a collaborative approach to medical decisions, particularly when no single best option exists. 12 Patients and their loved ones actively participate in shared decision-making by discussing their values and preferences with their health care providers, who share clinical knowledge, expertise, and best available evidence about risks and benefits.12,13 In recent qualitative work by our group characterizing conditions that favor and undermine VA-related shared decision-making, patients and health care providers emphasized upstream decisions about dialysis over VA type and a need for iterative, balanced discussions, and they recognized how failure to enact timely decisions about VA almost always resulted in hemodialysis via a central venous catheter. 14 As the success of shared decision-making relies in large part on establishing mutual understanding of one another’s perspectives, an important question arising from this work is the extent to which patients’ and caregivers’ views on VA decisions align with those of health care providers. Whereas other reports suggest that patients weigh anticipated VA benefits with complication risks and impacts on daily life15-18 and health care providers prioritize reliable and durable VA,19-22 to our knowledge no study has compared the perspectives of patients and health care providers on aspects of the VA decisional process qualitatively.
With Kidney Disease Outcomes Quality Initiative Clinical Practice Guidelines for Vascular Access emphasizing the “right access, in the right patient, at the right time, for the right reasons,” 23 VA clinicians are compelled to consider individuals’ circumstances, priorities, and values alongside their medical eligibility for a given access type. Recognizing their unique roles in the VA decision, an appreciation of the similarities and differences among the perspectives of patients, their caregivers, and health care providers on this issue is a critical first step toward shared decision-making in VA practice. Whereas shared views can identify common goals and how to achieve them, areas of divergence may suggest opportunities to bridge gaps in decision-making needs. Thus, to address a distinct and complementary research question emerging during our study of VA-related shared decision-making, we sought to explore the alignment among the perspectives of patients receiving hemodialysis, their caregivers, and health care providers regarding hemodialysis VA selection.
Methods
Study Design and Setting
We used a qualitative descriptive methodology to guide our study.24,25 This approach allows for exploration of insights regarding phenomena, such as VA selection, with implications for clinical practice. 26 This study took place across 5 outpatient, in-center hemodialysis units in the Alberta Kidney Care–South program in Alberta, Canada. We adhered to principles of rigor in qualitative research, including clear statement of purpose, data collection, and analytic techniques appropriate to the methodology, provision of data extracts to support our findings, researcher and data triangulation, and reflexive note taking. 27 We have reported this study in accordance with the Consolidated Criteria for Reporting Qualitative Research. 28 The University of Calgary’s Conjoint Health Research Ethics Board approved this study (REB18-1727).
Participants
Participants included adults ≥18 years of age from one of the following eligible groups: patients receiving maintenance hemodialysis for >3 months via an arteriovenous fistula or central venous catheter, their informal caregivers, and health care providers for people undergoing maintenance hemodialysis (ie, nephrologists, hemodialysis nurses, and VA nurses). Patients were excluded if they had a life expectancy of <1 year, cognitive impairment, or inability to communicate in English. Using a maximum variation approach, we sampled participants across relevant sociodemographic (age, sex, etc) and clinical characteristics (eg, dialysis duration and VA history [patients] and clinical role [health care providers]) to capture a range of experiences. A hemodialysis clinician identified eligible patients and health care provider participants, whom the research coordinator approached to discuss the study and assess their interest in participating. Eligible patients were asked to nominate potential caregiver participants, whom the research coordinator approached separately by telephone if not present during hemodialysis. Participants provided informed consent prior to each interview.
Data Collection
A research coordinator (S.L. and M.O.) with qualitative research training and experience conducted semi-structured interviews in person in hemodialysis units or by telephone, depending on participant preference, that lasted 20 to 60 minutes. The interviewer had no prior knowledge of study participants. We developed and pilot tested distinct interview guides for patients/caregivers and health care providers to explore their needs, experiences, and perceived roles related to VA decision-making (Supplementary Material). Both interview guides included open-ended questions with prompts to elicit participants’ experiences of selecting and/or living with VA. Interviews were audio-recorded and transcribed verbatim, except for one patient interview where detailed notes were taken instead at the participant’s request. Data saturation, defined as the point at which no new information was produced from interviews, was attained. 29 We collected demographic data from all participants for the purposes of summarizing our sample and informing recruitment of potential participants by the research coordinator in hemodialysis centers to achieve a diverse sample in keeping with our purposive sampling approach.
Data Analysis
Interview transcripts were uploaded into NVivo 12 (QSR International Pty Ltd) to facilitate data management and storage. Two research team members (A.S. and M.J.E.) used a thematic analysis approach to inductively and systematically code, analyze, and interpret the data to address our emergent research question after data collection was completed.30-32 We first reviewed interviews repeatedly to obtain a high-level understanding of the data and key concepts. We discussed the ideas raised by patients, their caregivers, and health care providers and generated initial, descriptive codes to capture distinct concepts. We applied preliminary codes to transcripts independently and in duplicate and met after every 3 to 4 transcripts to revise our coding scheme. We then applied final codes systematically across remaining transcripts. We developed separate coding schemes for patients/caregivers and health care providers to identify unique concepts arising from different participant types. The 2 team members compared and contrasted codes and organized them into preliminary themes. We refined final themes through team discussion and presented them as key concept areas in which patient/caregiver perspectives on VA selection aligned with or diverged from those of health care providers.
Results
In total, 42 individuals participated in this study (19 patients, 2 caregivers, and 21 health care providers). We conducted interviews by telephone with 23 participants and in person with 19 participants. Most patients (n = 12) had initiated hemodialysis less than 1 year previously. Most patients (n = 15) started hemodialysis using a catheter, and over half were dialyzing with a fistula at the time of interview (n = 10) (Table 1). Six patient participants had experience with both VA types. The 2 caregivers were spouses of patient participants in the study. Participating health care providers included 8 nephrologists, 7 hemodialysis nurses, and 6 VA nurses; most were women and had a range of clinical experiences (Table 2).
Characteristics of Patient (n = 19) and Caregiver Participants (n = 2).

Characteristics of Health Care Provider Participants (n = 21).
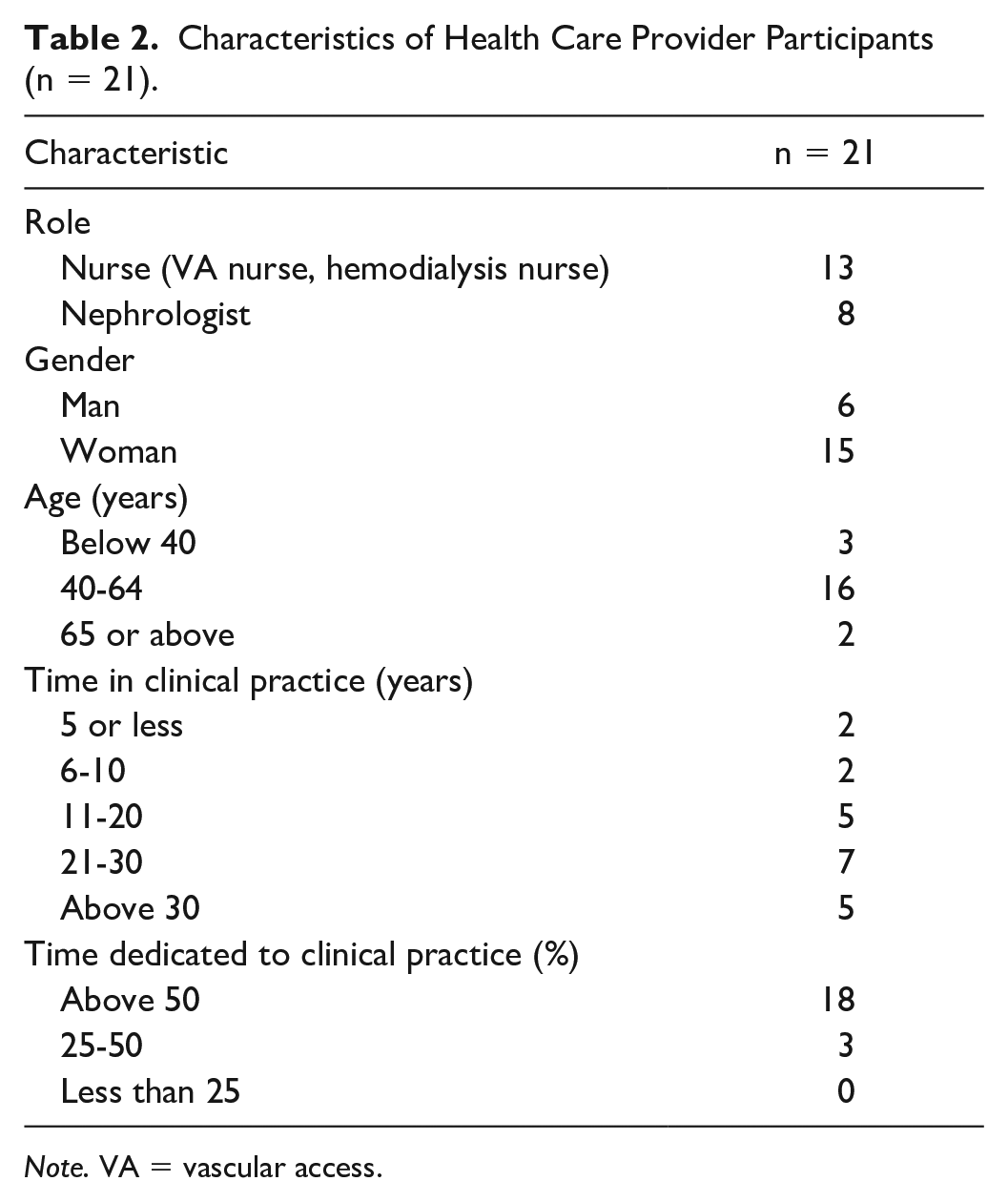
Note. VA = vascular access.
We identified 2 themes where patient, caregiver, and health care provider perspectives aligned in VA decision-making: (1) optimizing patient preparedness, and (2) value placed on trusting relationships with the kidney care team. We characterized 3 themes where patient and caregiver perspectives diverged from those of health care providers: (1) access priorities and preferences, (2) influence of personal and peer experience, and (3) endpoints for VA review. Relationships between themes are depicted in Figure 1, and exemplar quotes supporting each theme and conceptual category are provided in Tables 3 and 4.

Patient and health care provider perspectives on vascular access–related decision-making.
Exemplar Quotes for Themes and Subthemes of Perspective Alignment Among Patients, Their Caregivers, and Health Care Providers.

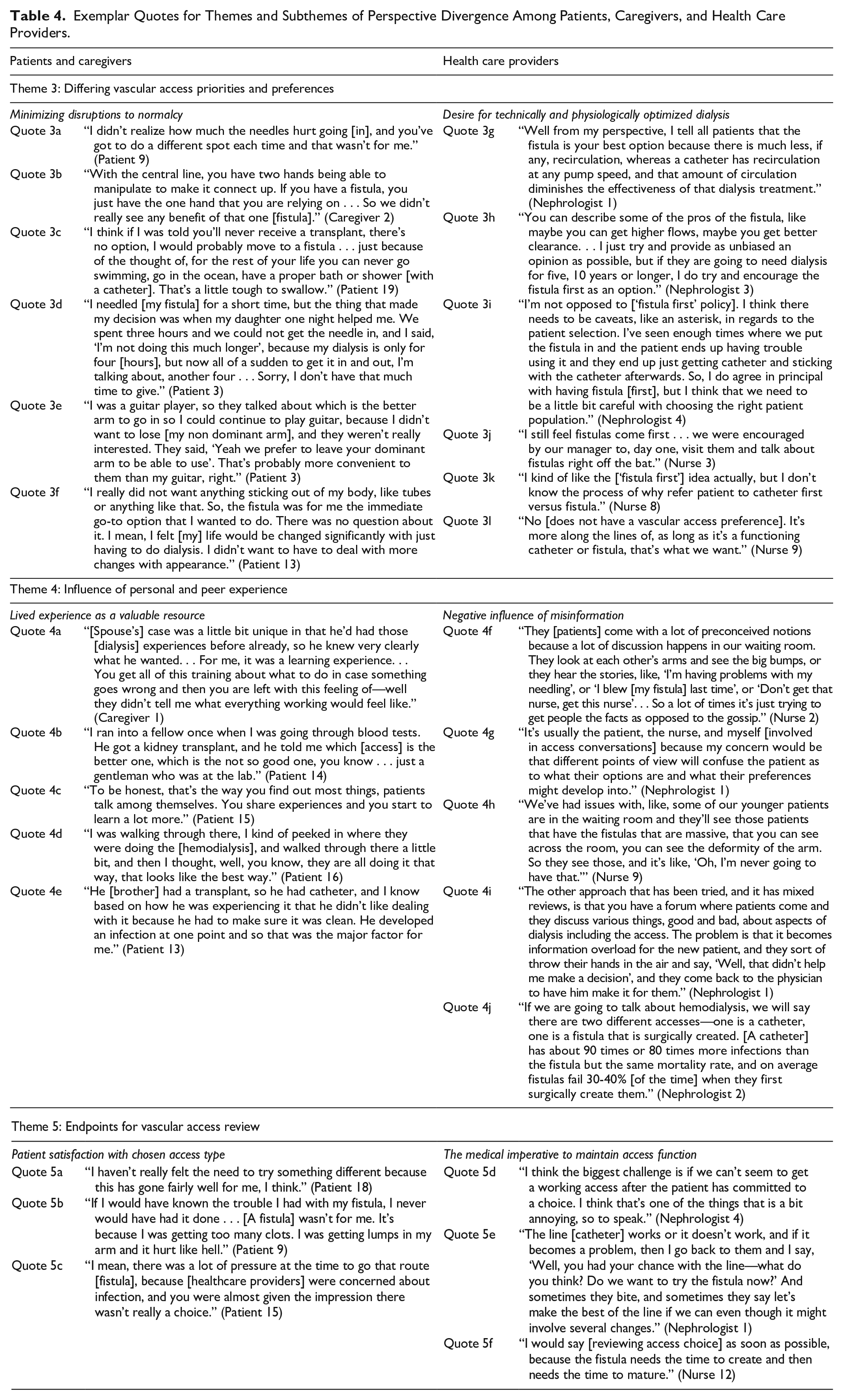
Exemplar Quotes for Themes and Subthemes of Perspective Divergence Among Patients, Caregivers, and Health Care Providers.
Perspective Alignment
Optimizing patient preparedness
Patients, their caregivers, and health care providers all identified the importance of adequately preparing patients for decisions about VA, yet acknowledged the difficulty of timing and engaging in VA decisions well in advance of dialysis need (Table 3). Despite efforts to address patient and caregiver knowledge gaps, participants noted that most patients lacked readiness to make informed decisions about dialysis and VA.
Defining ideal timing
Participants across roles discussed how difficulty predicting when a person might require kidney replacement therapy made it challenging to plan for VA discussions in predialysis kidney care programs (quotes 1a-b). Whereas several patients indicated that delaying conversations about access led to insufficient time for deliberation about their options, providers described how premature access discussions could lead to low information retention and precipitate unnecessary anxiety (quote 1c). Nephrologists suggested introducing dialysis modality and transplant options followed by VA when patients’ eGFR declines below 10 to 15 mL/min/1.73 m2 and/or they are progressing rapidly toward kidney failure (quotes 1c-d).
Tailoring to informational needs
Patients and providers emphasized the need to adapt the content of access discussions to patients’ informational needs (quotes 1e-g). Patients and caregivers varied in the amount, type, and format of information they felt was needed to support an informed, confident VA decision (quotes 1g-h)—whereas most appreciated the educational sessions provided by their care team and/or materials they could review independently, some suggested this information was difficult to digest and heightened their fears about dialysis. Participants across roles agreed that information should be shared in an incremental, iterative, and individualized manner to avoid overwhelming patients preparing for kidney failure.
Preparedness gap
Even where repeated discussions about VA options take place during clinical encounters, participants across roles noted that many patients lacked knowledge and confidence to select a VA when a decision was needed (quotes 1i-j). Some patients did not recall having discussed VA with their health care providers, and several had unanswered questions at the time of fistula or catheter placement that they felt should have been addressed earlier in their disease course (quote 1k). These included how different access types are established and used (eg, surgery and needling with a fistula), how to care for their access (eg, keeping a catheter clean), and impact of each VA type on activities (eg, ability to swim). One nurse suggested that patients’ lack of readiness or willingness to receive VA information adversely influenced their attempts to close this preparedness gap (quote 1l).
Value placed on trusting relationships with the kidney care team
Participants discussed how trusting relationships between patients and their healthcare providers facilitated VA decision-making. Moreover, once a decision about VA was made or needed imminently, enacting that decision ultimately required physician support (Table 3).
Reliance on the healthcare team to inform decisions
Patient and provider participants noted how the degree of desired autonomy in VA decisions varies across individual patients. While some patients held firm preferences for VA types and advocated for their choice, many patients and their loved ones relied on their kidney care providers to guide the decision-making process (quotes 2a-b). Providers suggested that patients who play an active role in the VA decision are more likely to pursue a fistula, which they recognized as invariably requiring more advanced planning than a catheter. However, several patients described not having a clear VA preference or not being ready to select one access type and deferring the decision to their nephrologist, whom they trusted to make the “right” decision in their best interests (quotes 2c-d).
Confidence in longitudinal relationship with nephrologist
Patients, their caregivers, and other health care providers identified the nephrologist as the provider who knows the patient best through longitudinal relationships established early in their kidney disease journey. Patient and nurse participants described turning to the primary nephrologist for guidance about VA decisions given their breadth of clinical experience and knowledge of their patients’ medical status, preferences, and support structures (quotes 2e-f).
Nephrologists as gatekeepers
Although many health care providers discussed the importance of informed decision-making about VA with support from their care team, participants across roles indicated how establishing VA could only proceed with endorsement from the physician, meaning the nephrologist or access surgeon must ultimately approve the request to create a fistula or place a catheter (quotes 2g-h). Participants suggested that although the decision about VA ultimately lay with the nephrologist, it should be informed by previous discussions and patients’ expressed preferences where possible (quote 2i).
Perspective Divergence
Differing VA priorities and preferences
Most patients and their caregivers prioritized minimizing disruptions to their predialysis life over a specific access type. This contrasted with health care providers’ prioritization of physiologically and technically optimized hemodialysis, resulting in a predominant preference for fistulas (Table 4).
Minimizing disruptions to normalcy
Patients did not uniformly prefer one access type over another, but rather that which would optimize their quality of life. For some, this meant minimizing pain and technical difficulty associated with the creation, potential revision, and use of a fistula (quotes 3a-b). For others, this included maintaining their ability to engage in recreational activities and minimizing time dedicated to dialysis-related tasks (quotes 3c). For example, one patient described how the additional time required to needle his fistula underlay his preference for a catheter, and another worried about how fistula creation in his nondominant hand might affect his ability to play the guitar (quotes 3d-e). Several patients also described wanting to avoid notable changes to their physical appearance, which might occur with both access types—whereas some preferred a catheter that they could hide under clothing, others preferred a fistula to avoid living with a visible device (quote 3f).
Desire for technically and physiologically optimized dialysis
Nephrologists largely prioritized physiological optimization and access longevity, resulting in a predominant preference for fistulas (quote 3g-h). However, they acknowledged that fistulas were not suitable for all patients and endorsed instead an approach that one nephrologist referred to as fistula first with “caveats” (quote 3i). In other words, they preferred a fistula for someone they perceived was an ideal candidate (eg, younger age, suitable vascular anatomy, and anticipated long-term hemodialysis) but indicated that a catheter would be a reasonable alternative under many circumstances, such as shorter life expectancy, unfavorable vascular anatomy, or anticipated transplantation.
Most VA nurses, whose training had largely encouraged fistula use, indicated a preference for fistulas for most individuals (quotes 3j-k). In contrast, bedside hemodialysis nurses did not express a preferred access type but rather whichever VA would facilitate a complete dialysis session free of technical complications (quote 3l). Despite acknowledging their VA preferences, most providers discussed attempts to balance their own priorities with those of their patients and individualize VA choice to their medical and personal context.
Influence of personal and peer experience
Patients and their caregivers discussed the value of their own and others’ experiences as an important resource for access-related decision-making (Table 4). Health care providers described how others’ negative VA experiences could unduly influence patients’ decisions and underscored a need for accurate, unbiased information.
Lived experience as a valuable resource
Patients discussed how their own prior experiences with VA influenced their willingness to consider a given access type (quote 4a). For example, patients who had experienced catheter infections or fistula revisions described being more likely to opt for the alternative when presented with the choice. They also described learning about living with hemodialysis and VA from other patients, whose anecdotes often centered on negative experiences with a given access type and left lasting impressions on patients making VA decisions (quotes 4b-e).
Negative influence of misinformation
While healthcare providers acknowledged the potential positive impact of others’ lived experiences on access decisions, they cautioned that fixating on poor VA experiences or outcomes could perpetuate misinformation (quote 4f-g). Several nurses and nephrologists gave the example of a patient observing aneurysmal fistula dilatation and concluding that this was an inevitable outcome (quote 4h). They recognized that patients may have difficulty discerning the accuracy of VA information and indicated it was providers’ responsibility to ensure patients have access to varied, pragmatic, and evidence-informed resources on the risks and benefits of VA options (quotes 4i-j).
Endpoints for VA review
While participants across roles conveyed the importance of reviewing VA selection once established, they differed in the indications and timing prompting VA reassessment (Table 4).
Patient satisfaction with chosen access type
Patients and caregivers appreciated periodic check-ins from their health care providers to ensure ongoing VA satisfaction. However, unless they had experienced complications, access-related pain, or repeated access interventions, they indicated they were unlikely to want to switch to the alternative VA type (quote 5a). Conversely, unintended negative VA sequelae, such as pain and needling difficulty described by one patient upon their switch from catheter to fistula, led to dissatisfaction and a desire to review their chosen access type (quote 5b). Some patients with catheters disclosed feeling pressured to pursue a fistula as a result of routine VA review initiated by health care providers, regardless of their satisfaction with their existing catheter (quote 5c).
The medical imperative to maintain access function
While health care providers wanted patients to be satisfied with their chosen VA, they indicated that regular access review went hand in hand with assessment of the ongoing safety and efficacy of hemodialysis. Nephrologists and VA nurses described a professional responsibility to review VA proactively both before and after starting hemodialysis and identify complications early that might prompt intervention or a change in VA type, such as progressive central vein stenosis from catheter use or poor fistula maturation (quote 5d). Health care providers acknowledged their tendency to review patients with catheters more readily than those with fistulas, which they related to their training, preferences for fistulas, and/or recognized need for advanced planning to establish a fistula (quotes 5e-f).
Discussion
In characterizing the perspectives of patients, their caregivers, and health care providers related to hemodialysis VA decision-making, we identified opportunities and strategies to promote alignment and collaboration in the VA selection process (Figure 1). Although participants recognized the importance of timely information sharing and a strong foundation of trust in the care relationship, they noted that many patients remained underprepared to choose their preferred access when a decision was needed. Our observed differences in perspectives across participant roles could challenge the VA decision-making process when, for example, providers’ preferences for a given access type influence how access options are introduced and reviewed or if they conflict with patients’ own priorities and goals. The experiences of patient participants and others with specific access types emerged as a valuable resource that could help patients prepare for decisions about VA, provided the information is credible and accurate.
Our findings underscore variability in the extent to which patients and their caregivers want to engage in VA decision-making—while some preferred a greater degree of involvement, others deferred the decision to their providers, particularly their nephrologist. This finding is compatible with medical decision-making literature that distinguishes patient participation in decision-making processes from decisional autonomy. 33 Whereas patients may defer a decision for reasons, including lack of medical and experiential knowledge or perceived contextual barriers (eg, too little time to decide), most want to be involved in the deliberative processes leading up to the decision.34-36 As “deciding not to decide” about VA would nearly always lead to central venous catheter placement as the most accessible and least invasive option,14,37 our findings underscore how reviewing the implications of VA options and patients’ preferences can engage patients in the decisional process, even for those who choose to defer the decision.
When providers neglect to initiate or invite patients to engage in decision-making discussions, patients may be unsure if or how they are meant to contribute.35,38 In an international survey on VA-related decision priorities, the low priority assigned by providers to patient involvement in care suggests the role of patients in VA selection may be underappreciated and that providers may not sufficiently consider patients’ needs and values in the decision. 20 For many providers, involving patients in decision-making does not come naturally but is a learned skill that requires training and practice.39,40 A historical lack of patient involvement in VA selection and clinician familiarity and experience with shared decision-making may amplify the VA “preparedness gap” identified by our study participants. 10
Patients’ prioritization of enhanced quality of life contrasted with health care providers’ focus on delivery of complication-free dialysis through access longevity and physiological optimization of dialysis delivery. Although these are not mutually exclusive, for some patients prioritizing access functionality and longevity comes at the cost of pain, procedures, and complications (eg, fistula aneurysm). 41 Participants indicated that most VA informational resources available to patients tend to focus on the medical risks and benefits of each access type and underemphasize their implications for day-to-day living. Across roles, participants suggested that integration of hands-on experiences into VA patient education, including exposure to others with experience of different VA types, could help patients anticipate the impact of VA on quality of life while minimizing inaccuracies that may be shared during informal peer encounters.42-44
Most health care providers expressed a preference for fistulas or, at minimum, an individualized approach to access selection, whereas patients did not endorse a uniformly preferred VA type. Providers’ support for a “fistula first” approach may reflect their training, adherence to historical guideline recommendations or local policy, and the fact that while no randomized trial evidence has demonstrated fistula superiority over catheters, no compelling data have suggested fistula inferiority either.7,45 In a 2014 survey of European VA experts, 85% of respondents indicated the evidence base was sufficiently robust to support a “fistula first” policy, although authors acknowledged a potential disconnect between perceived and actual evidence strength. 21 Emerging evidence has since characterized both patient- and access-related influences on VA outcomes and underscores the need for individualization.46-48 Moving away from “fistula first” policy does not mean fistula avoidance, but rather supporting appropriate fistula use among eligible and interested individuals. 49 Although several of our patient and provider participants suggested that fistulas offer the best clinical outcomes and quality of life, they acknowledged that a blanket approach was inappropriate and could conflict with patients’ priorities.
Our study provides a strong rationale for the integration of shared decision-making in VA selection. Shared decision-making does not mean patients and their health care providers agree on all aspects of a medical decision, but rather that they reach a mutual understanding of patients’ priorities and implications of the decision. 50 However, there remains a paucity of primary research on how to “do” shared decision-making in VA practice. By examining complementary perspectives, our study presents pragmatic aspects of VA care that can be targeted by future interventions to enhance shared decision-making. For example, recognizing alignment on the need to optimize patient preparedness could justify development of decision support resources (eg, decision aids) to enhance knowledge, decisional readiness, and relationships between patients and their care team (Figure 1). Conversely, identifying how VA preferences and priorities diverge could prompt changes to how clinicians are trained in VA selection and create opportunities for VA exposure for patients. Bridging such gaps can help reduce decisional conflict, distill informational burden, and improve patient satisfaction with the outcome. 51 Our findings support standardized, iterative VA review processes with the kidney care team, leading up to and after hemodialysis initiation and irrespective of VA type.
Our study was strengthened by the inclusion of diverse perspectives on an issue with implications for practice and policy, yet we acknowledge some limitations. As participation was limited to English-speaking participants from urban, in-center hemodialysis units, it is possible that individuals from other regions or predialysis care programs may have expressed differing views. Furthermore, as few women, younger patients, and people from ethno-cultural minority groups participated, we could not explore or present findings attributable uniquely to these subgroups. We also had few caregiver participants, which we attribute to the lack of caregiver presence on site during hemodialysis sessions and reliance on nomination by patient participants. We recommend further dedicated study of VA selection perspectives in the populations underrepresented in our study or not captured by our inclusion criteria (eg, home hemodialysis). Our study also included many participants dialyzing via a catheter, whereas outside of Canada fistula use is much more common. 52 As arteriovenous graft use is low in Canada (<5%), we did not include individuals dialyzing via this access type. However, we did capture perspectives from several individuals who had changed VA type and with varying VA experiences, which provided depth to our findings. Last, participant perspectives reflect regional practices and policies, which may differ from hemodialysis programs internationally with different care models or where fistula use is tracked as a quality indicator and/or is financially incentivized. As expressed VA views and preferences relate both to long-held VA practices and to a more recent global shift toward VA individualization, findings are likely to be transferable to other similar contexts.
Conclusions
Our findings underscore opportunities to enhance the experience of VA selection for people receiving hemodialysis. Although many patients and caregivers lack readiness to engage in VA decisions, they wish to be informed of their options and involved in the deliberative process. Preference-focused discussions and pragmatic educational approaches that integrate the implications of VA for day-to-day living can promote confidence and satisfaction with the VA choice. The fact that many patients receiving hemodialysis described deferring the VA decision to their nephrologist suggests a high degree of trust in their physician’s judgment but also a burden of responsibility to ensure that the decisional outcome reflects patients’ priorities and values. Acknowledging how the diverse perspectives of patients, caregivers, and kidney care providers align and diverge is a critical first step toward innovative decision support resources, such as decision aids and “hands-on” educational opportunities, that bridge knowledge and readiness gaps.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581231215858 – Supplemental material for Alignment Among Patient, Caregiver, and Health Care Provider Perspectives on Hemodialysis Vascular Access Decision-Making: A Qualitative Study
Supplemental material, sj-docx-1-cjk-10.1177_20543581231215858 for Alignment Among Patient, Caregiver, and Health Care Provider Perspectives on Hemodialysis Vascular Access Decision-Making: A Qualitative Study by Angela R. Schneider, Pietro Ravani, Kathryn M. King-Shier, Robert R. Quinn, Jennifer M. MacRae, Shannan Love, Matthew J. Oliver, Swapnil Hiremath, Matthew T. James, Mia Ortiz, Braden R. Manns and Meghan J. Elliott in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
We thank Ms Sarah Gil for her graphic design expertise in figure development and Ms Corri Robb for her transcription services.
Ethics Approval and Consent to Participate
This study was approved by the University of Calgary’s Conjoint Health Research Ethics Board (REB18-1727).
Consent for Publication
All authors contributed to critical revisions of the article and approved the final draft.
Availability of Data and Materials
This study used individual, participant-level data collected during interviews. We are unable to make our data set available due to restrictions on sharing potentially identifiable data as outlined in our Research Ethics Board certification. Inquiries related to this study’s data set can be directed to the corresponding author.
Author Contributions
A.R.S., M.J.E., K.M.K.-S., and P.R. contributed to research idea and study design. S.L. and M.O. contributed to participant recruitment and data collection. A.R.S. and M.J.E. contributed to data analysis and thematic generation. M.J.E. contributed to supervision or mentorship. All authors contributed to interpretation. Each author contributed important intellectual content during manuscript drafting or revision and agrees to be personally accountable for the individual’s own contributions and to ensure that questions pertaining to the accuracy or integrity of any portion of the work, even one in which the author was not directly involved, are appropriately investigated and resolved, including with documentation in the literature if appropriate.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.H. serves on the board of NephJC (![]() ), which is a 503c organization that supports social media in medical education and has multiple industry and academic supporters. S.H. receives no remuneration for this position. M.J.O. is sole owner of Oliver Medical Management Inc which is a private corporation that licenses the Dialysis Measurement Analysis and Reporting (DMAR) software system; has received honoraria from Baxter Healthcare; and is contracted Medical Lead at Ontario Renal Network, Ontario Health. R.R.Q. is co-inventor of the Dialysis Measurement Analysis and Reporting (DMAR) software system and has received honoraria from Baxter Healthcare. No other authors have disclosures.
), which is a 503c organization that supports social media in medical education and has multiple industry and academic supporters. S.H. receives no remuneration for this position. M.J.O. is sole owner of Oliver Medical Management Inc which is a private corporation that licenses the Dialysis Measurement Analysis and Reporting (DMAR) software system; has received honoraria from Baxter Healthcare; and is contracted Medical Lead at Ontario Renal Network, Ontario Health. R.R.Q. is co-inventor of the Dialysis Measurement Analysis and Reporting (DMAR) software system and has received honoraria from Baxter Healthcare. No other authors have disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a Canadian Institutes of Health Research project grant (FRN162369) and Kidney Foundation of Canada Health Research grant (KFOC190009). The funders had no role in study design, data collection, analysis, reporting, or the decision to submit for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.