
Abstract
Purpose of program:
Adolescents and young adults with chronic disease face many personal and systemic barriers that may impede their successful transition from pediatric to adult care, putting them at risk for treatment nonadherence, loss to follow-up, and poor health outcomes. Such barriers include impaired socioemotional functioning, overreliance on adult caregivers, lack of disease-specific knowledge, and poor coordination between pediatric and adult health care services. In 2007, we established a specialized youth to adult nephrology transition clinic at a tertiary care center to address these barriers and provide adolescents and young adults with renal disease followed at the affiliated children’s hospital with a seamless transition to adult care.
Sources of information:
The attending clinic nephrologist collected data prospectively for this quality improvement report.
Methods:
The features of this specialized clinic included (1) single point of entry and single triage adult nephrologist, (2) ongoing follow-up with a single adult nephrologist who communicated with the pediatric nephrologists, and (3) a single specialized clinic nurse who provided disease-specific education and helped to ensure ongoing patient engagement and follow-up. Importantly, the transition patients were booked into regular appointment slots in the adult nephrologist’s general clinic, which facilitated regular follow-up without additional resources. The salary of the transition clinic nurse was covered by an unrestricted grant. Patient visits were in-person, except between 2020 and 2021 when visits were by telephone due to the pandemic.
Key findings:
A total of 213 patients were referred and assessed in the transition clinic from February 2007 until October 2022. Most referrals were from pediatric nephrologists. Among the patients, 29% had a hereditary kidney disease; in 71%, the disease was acquired. The most common disease was glomerulonephritis and ~30% of the patients suffered from a “rare” disease. Of the 213 patients, 123 (58%) continue to be followed up (mean follow-up: 4.8 years), 27 (13%) were transferred to other physicians, in part to accommodate treatment closer to patients’ homes, and 29 (14%) without ongoing care needs were discharged. Only 33 (15%) were lost to follow-up. There were several advantages to the clinic, including the maintenance of accurate records, a process to minimize loss to follow-up, and a “critical mass” of patients with rare diseases, which facilitated development of special expertise in rare disease pathogenesis, diagnosis, treatment, and management of complications. Patients with glomerulonephritis demonstrated a stable serum creatinine over 3 to 15 years, and morbidity (as reflected by emergency room visits and hospitalizations) was low.
Limitations:
Due to the relatively small numbers of patients in the disease categories, it was not possible to determine conclusively whether attendance of patients in the transition clinic reduced the rate of progression of kidney disease or morbidity.
Implications:
A dedicated referral, triage, and follow-up process post-transition with only modest financial resources and personnel can result in accurate tracking of clinic data, as well as consistent and reliable follow-up and expert patient care.
Purpose of Program
As children affected by kidney disease are fortunately living longer, the number of patients requiring transfer of care from pediatric to adult nephrologists is increasing.1-5 This transfer usually occurs at or shortly after the age of 18 years. There are major structural differences between child and adult-centered health systems, and attention to these young adult patients may decrease as they become a small proportion of the total patients treated in the adult setting. As a result, these young adults must take on increasing responsibility to manage their own health problems. Often, these patients are inadequately prepared for this transition, putting them at risk for treatment nonadherence, loss to follow-up, and poor health outcomes.1,3,5,6 Barriers to successful transition to adult care include impaired socioemotional functioning, overreliance on adult caregivers, lack of disease-specific knowledge, and poor coordination between pediatric and adult health care services. Even simple things such as change of clinic location have been shown to be a barrier to successful transition. 3 Adolescence is a time of increasing independence and experimentation. Risk-taking behavior may lead to nonadherence with medications and reduced engagement with health care providers.1,3,5,6
The pediatric literature suggests that transition is best served by dedicated clinics to teach principles of self-reliance in adolescence prior to transfer. Various recommendations have been proposed to optimize transition care. For example, adolescents with special health care needs and their families should receive medical, educational, and psychosocial support from their health care teams during the transition, 7 and financial funding models should support practices that lead to optimal longitudinal health outcomes. 7 Guidelines recommend children be taught to develop self-management skills, and their readiness be assessed pretransition. Most importantly, pediatric and adult providers should receive education and organizational support from the health care systems in which they work. Extensive reviews concluded that transition processes need to be coordinated between the professionals involved in patient care, and that a transition coordinator, facilitator, or navigator should be identified.8,9 The latter is key for identification of young people with special health care needs and families requiring support, to ensure that adolescents be provided with the appropriate links and resources to engage with adult services, and to provide continuity of care. Good communication between pediatric and adult specialists and even primary care physicians is paramount, which may be facilitated by a joint synchronous clinic.10,11 Continuation of supports, such as social worker, educational counselor, psychologist, and so on, is also important for those patients who may be most vulnerable. It is unreasonable to believe that a 17-year-old individual with chronic kidney disease (CKD) who required extensive medical, educational, and psychosocial supports in the pediatric clinic no longer needs these on the day of their 18th birthday. To evaluate the success of transition, it has also been proposed that transitioning adolescents should be monitored into their mid-20s with various health care transition tools. 12
While the above guidelines are laudable, it is unclear whether teaching provided to transitioning adolescents is uniformly retained or effective. Resource constraints often preclude implementation of guidelines, even in tertiary care centers. Furthermore, guidelines and studies on how to optimally care for young adults post-transition are limited. Few disease-specific guidelines exist, and to our knowledge, none exist for kidney diseases. 8 Yet despite these constraints, the number of children with kidney disease reaching adult care has been increasing over the last decade.
Recognizing the need to better plan, provide support, and reduce adverse outcomes associated with transfer from pediatric to adult care in this growing population, a special referral and clinical follow-up process was established for patients with kidney disease approaching age 18 years at the McGill Royal Victoria Hospital in Montreal in 2007. This process is herein referred to as the “transition clinic.” The goal was to provide the Montreal Children’s Hospital pediatric patients who required ongoing nephrology care with a seamless referral and transfer process, which would assure that the young patient arrives in the clinic at an associated adult institution and receives close follow-up and monitoring despite the absence of dedicated resources. In this quality improvement report, we present our real-world experience of the McGill pediatric to adult nephrology transition clinic over the last 15 years. We demonstrate that a dedicated referral, triage, and follow-up process with only modest financial resources and personnel can result in accurate tracking of clinic data, as well as consistent and reliable follow-up and expert patient care.
Methods
Transition Process
The Montreal Children’s Hospital and the adult Royal Victoria Hospital are components of the McGill University Health Centre in Montreal, Quebec. In Quebec, pediatric patients are required by law to transition to adult care at age 18 years, although exceptions have been made for occasional patients. Nephrology patients at the Montreal Children’s Hospital are under the care of pediatric nephrologists. Two pediatric nephrology nurses have also been involved in the care of more complex patients. 4 Prior to 2007, transitioning pediatric patients were referred to multiple adult nephrologists without a systematic referral process.
To improve the continuity of care, a youth to adult nephrology transition clinic was started at the Royal Victoria Hospital in February 2007. The features of this specialized clinic included the following: (1) single point of entry and single triage nephrologist (A.V.C.), (2) ongoing follow-up with a single nephrologist (A.V.C.) who communicated with the pediatric nephrologists, and (3) a single specialized clinic nurse (L.C.) who provided disease-specific education and helped to ensure ongoing patient engagement and follow-up (1.5-2.0 h/week). Other personnel such as clinic secretary and multidisciplinary services (dietician, social worker, and most other specialists) were the same as those used for the regular adult nephrology clinics. There were no specific financial resources allocated to the transition clinic, except that the salary of the transition clinic nurse was covered by an unrestricted grant. From 2007 and 2015, the transition clinic was situated at the original Royal Victoria Hospital, at a distance of 2.5 km away from the Montreal Children’s Hospital. In 2015, both adult and pediatric hospitals moved into different pavilions of a single new facility connected by indoor hallways.
Transition Clinic Structure
As the transfer of care deadline approached, pediatric nephrologists would refer patients directly to the dedicated adult nephrologist (A.V.C.). All patients followed up by pediatric nephrologists were eligible for the transition clinic, with the exception of pediatric patients receiving dialysis or with a kidney transplant. Pediatric patients receiving dialysis were transferred directly to the adult dialysis program, while transplanted patients were transferred to the adult transplant clinic. Referrals were triaged by A.V.C. according to medical urgency and the day of the last pediatric visit. A single administrative assistant handled clinic bookings, organized investigations, and transmitted referrals to other specialists, although over 15 years, at least 5 different administrative assistants filled the position. Hospital clerks called patients in advance of their appointments during the past 4 to 5 years, but these calls were not made regularly due to lack of hospital resources.
A single adult nephrologist (A.V.C.) assessed all patients over the period of time encompassing this analysis (February 2007 to October 2022; 15.75 years). A single electronic medical record contained patient information from both the pediatric and adult units. As transition patients comprised a minority of A.V.C.’s total adult nephrology practice, the transition patients were booked into regular appointment slots in A.V.C.’s general nephrology clinic. All patient visits were in-person up to the time of the COVID-19 pandemic (2020), at which time, visits were carried out via telephone. A significant portion of visits returned to in-person in 2021 to 2022. Many newly referred patients arrived to the first clinic visit with 1 or both parents, and for some patients, this practice continued for follow-up visits. As per transition guidelines,3-5 written communication was typically provided by the attending staff pediatric nephrologist. A physical visit by the pediatric nephrologist sometimes took place, but was not always possible because of time constraints and travel distances between pediatric and adult venues, conflicting schedules, and in more recent years, due to COVID-19. After the first visit, there was informal communication between the adult and referring pediatric nephrologists as needed, although there was no formal participation of pediatric nephrologists or pediatric nurses in the post-transition process.
A part-time transition clinic nurse was specifically employed from August 2020 to November 2021 and during October 2022. The role of the transition clinic nurse was to contact patients in advance of appointments to remind them about the appointment, verify prescribed medications and compliance with medications, as well as to inquire about the patient’s occupation and whether there were any social issues or other problems that could then be discussed with the physician during the visit. In addition, the nurse provided advice on how the patient could access a provincial repository of his/her laboratory data and radiologic studies, and how a patient could locate a family doctor. It should be noted that where appropriate, certain patients transitioning to adult nephrology care were at the same time referred to other adult specialists for follow-up, for example, urology, cardiology, hematology, endocrinology, and psychiatry. A dietician who was part of all adult medical clinics was available for consultations. A nurse covering all medical clinics was available for organization of certain tests, such as ambulatory blood pressure monitoring. A social worker could be contacted on an ad hoc basis if needed.
Data Collection and Analysis
Medical summaries of all patient visits and of telephone calls were entered into the hospital medical record. In addition, the attending nephrologist maintained an Excel spreadsheet of all patients assessed in the clinic, including demographic data, principal diagnoses, and dates of initial and most recent assessments, or dates and reasons for discharge, transfer, or loss to follow-up. This record was used routinely to identify patients who missed scheduled appointments and to reschedule when appropriate.
This article is based mainly on a descriptive analysis of the clinic record. Statistical data are presented as mean ± SD. Comparisons between 2 groups were done by a 2-tailed Student’s t test. For 3 or more groups, statistical differences were assessed using 1-way analysis of variance. Where significant differences were found, post hoc analyses were performed using Šidák’s multiple comparisons test. Excel and Graphpad Prism analytic and graphic tools were employed.
Key Findings and Discussion
Characteristics of Patients Assessed
A total of 213 patients were assessed in the transition clinic from February 2007 until October 2022 (Table 1). Most referrals were from pediatric nephrologists at the Montreal Children’s Hospital; a small number of patients were referred by other pediatric or adult specialists, and by the emergency department. Of the referred patients, 123 (58%) continue to be followed up in the transition clinic as of October 2022 (“active” patients, Table 1). The number of patients assessed and remaining active has increased over time (Table 1, Supplemental Figure 1), and was significantly greater in the last 5 years, compared with the previous 10 years (Supplemental Figure 2). It is unclear whether this is due to increased disease prevalence in children, longer follow-up in the pediatric clinic, or increased awareness of the transition clinic.
Baseline Characteristics and Follow-up of Transition Clinic Patients.

Note. ADPKD = autosomal dominant polycystic kidney disease; FSGS = focal segmental glomerulosclerosis; IgA = immunoglobulin A; MCD = minimal change disease; GN = glomerulonephritis.
Diagnoses were established by clinical presentation, family history, radiologic imaging, biochemical testing, and/or DNA sequencing.
No clear link to a monogenic mutation.
One of the 2 patients with C3 glomerulopathy (C3GN) did not demonstrate any mutations in complement genes and had no nephritic factors; the second patient had a nephritic factor, but DNA sequencing was not performed.
Includes suspected renal dysplasia/hypoplasia, congenital anomalies of the kidney and urinary tract (CAKUT), obstruction, and other undefined conditions. A single case was associated with congestive heart failure.
Includes congenital absence of a kidney or severe atrophy, and nephrectomy for obstruction or reflux.
Eighty percent of patients were referred at the age of 18 to 19 years, 44% were female, and 29% had hereditary renal diseases (Table 1). In the initial planning phase, the transition clinic was to focus on genetic kidney diseases (typically due to monogenic mutations) or congenital renal diseases, but after a review of potential referrals, it became apparent that the majority of pediatric nephrology patients who required adult follow-up had “acquired” kidney diseases (71%, see below). There were no significant differences in baseline characteristics between those who remained active versus those who were discharged or lost to follow-up.
Follow-up
The mean follow-up of all 213 patients was 3.8 years (range <1-15 years) (Figure 1, Supplemental Table 1). As noted above, of the 213 assessed patients, 123 (58%) remain actively followed up. Of the 90 who are no longer followed up, 30 (14%) were discharged, 27 (13%) were transferred to other physicians, and 33 (15%) were lost to follow-up (Figure 1, Table 1).

Patient activity.
The majority of patients who were discharged did so within the first 2 years of follow-up. Most transfers also occurred within 3 years, but a number of patients were transferred after 3 years; thus, the years of follow-up of transfers exceeded those of discharges (Figure 1, Supplemental Table 1). The principal reasons for discharges and transfers are presented in Figure 2. Most discharged patients no longer required or were not interested in nephrology follow-up, and could often be seen by another specialist or family doctor. Among the transfers, 4 patients reached an advanced stage of CKD and their care was transferred to a multidisciplinary CKD clinic, while 1 patient required start of emergency dialysis and was then transplanted. Several patients with autosomal dominant polycystic kidney disease (ADPKD) were transferred to a specialty ADPKD clinic in the same hospital to initiate treatment with tolvaptan. A few patients who became pregnant were temporarily transferred to a nephrologist who subspecializes in high-risk pregnancy. The remainder were transferred to physicians closer to their homes. In Montreal, pediatric nephrology care is concentrated in a few centers, while availability of adult nephrologists is more widespread. Once patients turn 18 years, there are increased opportunities to see physicians closer to their homes and reduce travel time to appointments. In addition, some patients of college age moved to other areas to study and were consequently transferred to other physicians.
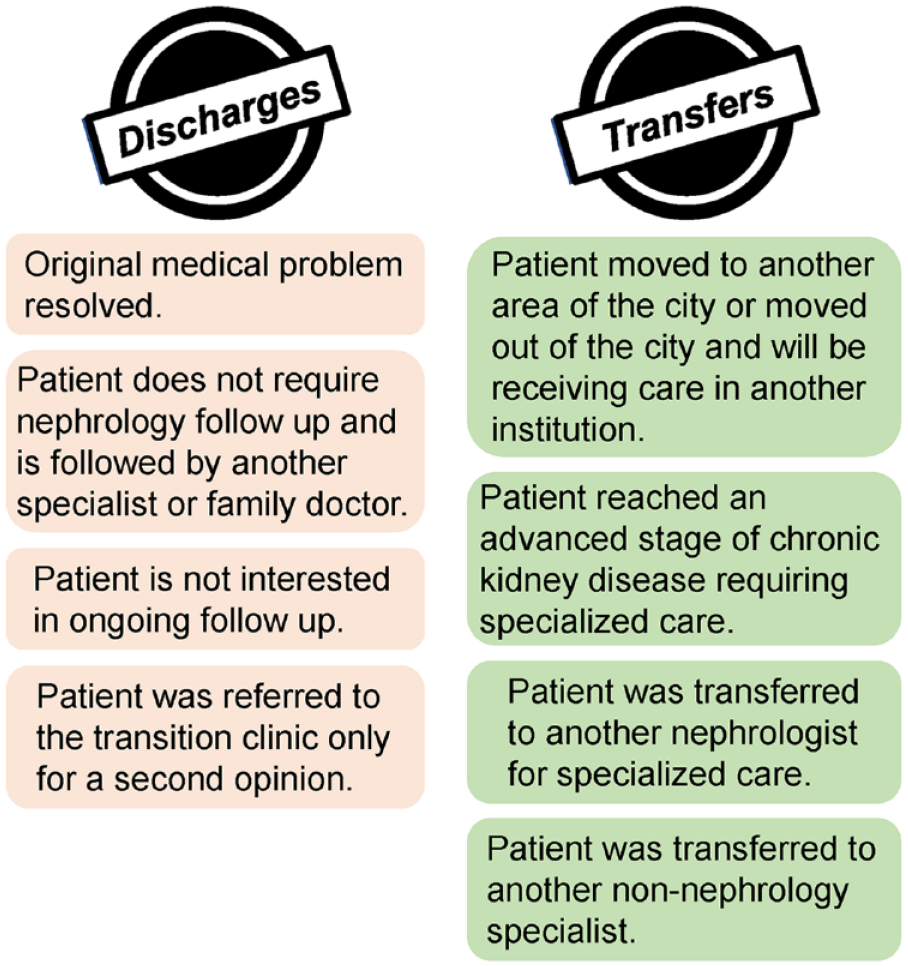
Principal reasons for discharges or transfers from the transition clinic.
The losses to follow-up were concentrated in the first 3 years (Figure 1, Supplemental Table 1). When analyzed by the year of the event, most losses to follow-up occurred between 2012 and 2016, after which time, these declined (Supplemental Figure 1). These individuals usually did not arrive for scheduled appointments despite reminders. Some of these patients or family members were then contacted, but ultimately did not rebook appointments, and were then officially discharged from the clinic. Some patients or families could not be located as their coordinates were outdated in the hospital record. Data on losses to follow-up in ambulatory clinics (outside of clinical study protocols) are limited. For comparison, losses ranged from 16% to 61% over 4 to 5 years in adult ophthalmology clinics13,14 and 21% over 5 years in a breast cancer clinic. 15 Another ophthalmology clinic reported a loss to follow-up of 11% after 6 months. 16 In these studies, it was noted that patients who lived farther from the clinic were more likely to be lost. Loss to follow-up was estimated at 14% over a median time of 5.9 years in a well-characterized cohort of children and adolescents with chronic endocrine diseases followed up at a single university center. 17 In a Quebec population survey of children with congenital heart disease diagnosed before age 6 years, it was found that loss to follow-up with cardiology was 28%, 47%, and 61% by the 6th, 13th, and 18th birthdays, respectively, although up to 93% retained some contact with the health care system into early adulthood. 18 Finally, a survey of adult patients in our general nephrology clinic, which involved 88 patients assessed during the first half of 2016, showed a loss to follow-up of 13% over the next 6 years. Thus, the 15% loss to follow-up in the transition clinic compares favorably with these analyses.
Renal Diagnoses
The prevalence of specific renal diagnoses is provided in Table 1. Most diagnoses had an active follow-up rate of 45% to 100% over the follow-up time, except for patients with hypertension, of whom 40% remain in active follow-up.
The proportion of patients in our cohort labeled with hereditary diseases was 29% (61/213, Table 1). This is similar to recent studies employing next-generation DNA sequencing which suggest that ~24% to 37% of patients with CKD may have a monogenic basis for their disease.19,20 However, it should be noted that our patients with acquired disease did not undergo DNA testing.
Among the hereditary diseases, the most common diagnoses of assessed patients are presented in Table 1. Autosomal dominant polycystic kidney disease was the most prevalent hereditary disease, and 50% of these patients were transferred to a specialty clinic at the same institution for tolvaptan treatment. Alport’s nephritis was the most prevalent hereditary glomerulopathy. Two of the 9 patients with Alport’s nephritis reached advanced CKD. Other diagnoses with smaller numbers of patients included nail-patella syndrome (LMX1B mutation), nephrogenic diabetes insipidus, and sickle cell nephropathy (3 or fewer patients per category).
The most frequent diagnoses in the acquired category were glomerulonephritis (most commonly IgA nephropathy or minimal change disease), CKD, and hypertension (in most cases without a secondary cause) (Table 1). Patients with minimal change disease had either a history or had ongoing relapses of nephrotic syndrome. Several patients were followed up for hematuria; some of these may have had glomerulonephritis, but this was not confirmed by kidney biopsy. A significant number had reflux nephropathy or a solitary kidney (various etiologies, Table 1). Two patients had nutcracker syndrome. Other diagnoses with smaller numbers of patients included acute kidney injury that recovered, noncystinuric kidney stones, and type I diabetic nephropathy (3-5 patients per category). The proportion of active patients versus those who were no longer followed up in the clinic was relatively similar across the acquired and hereditary disease categories.
Outcomes
An interesting question is whether a specialized nephrology clinic improves renal outcomes. In our transition clinic, there were few active patients in each disease category, with variable lengths of follow-up, precluding us from ascertaining whether attendance of patients in the transition clinic (compared with adolescent patients in other settings without oversight) reduces the rate of progression of kidney disease or morbidity. Nevertheless, we collected outcomes in the cohort of active patients with glomerulonephritis with at least 3 years of follow-up data. Mean serum creatinine did not change significantly over the follow-up period (73 ± 24 vs 81 ± 34 μM, N = 18; Supplemental Figure 3). This cohort of 23 patients experienced 33 emergency room visits over 128 patient-years. Of the 33 visits, 8 were related to relapse of nephrotic syndrome, 1 to immunosuppressive medication toxicity, and 24 were unrelated to glomerulonephritis. Importantly, 23/33 visits were accounted for by a single patient (7 related to glomerulonephritis and 1 unrelated). There were no hospitalizations in this cohort. The frequency of emergency room visits for glomerulonephritis—a chronic disease—compares favorably with the overall number of emergency room visits in Canada, which is 495 per 1000 population/year. 21
Some information on outcomes of transition care is available in kidney transplantation. Outcomes of 16 kidney transplant recipients who attended a transition clinic were compared with 16 historical control patients who were transferred before the transition clinic was established. Nonadherent behavior in the year post-transfer, which included missing clinic visits, blood tests, and medications, was significantly lower in the cohort that attended the transition clinic. 22 Another study of young kidney transplant recipient suggested that recipients in a young adult clinic have better clinical and psychosocial outcomes than those in a regular adult clinic. These outcomes included graft loss, episodes of rejection, number of hospitalizations, and adherence to medications. 23
Advantages of the Transition Clinic
In our opinion, the clinic, despite modest resources, has provided several apparent benefits to the young adults transitioning to adult care. A key factor noted previously is having a dedicated “transition team.” 3 In this case, a single point of referral to a single adult nephrologist who assumed responsibility for these patients helped to ensure referrals were not “lost” and uniform processes were implemented to minimize losses to follow-up. Accurate records of patients have been maintained by the attending nephrologist throughout the duration of the clinic, facilitating clinical care. New referrals were sent directly to the attending nephrologist, and patients were then booked as necessary. Appointment dates were reviewed regularly. Patients who missed or were not scheduled for follow-up visits were identified and rebooked, or other arrangements were made. The attending nephrologist verified that referrals for investigations or to other specialists were booked and had subsequently taken place. Although labor intensive, this approach, including follow-up reminders for missed visits, has been noted to contribute to successful transition in a prior study. 3
The recent addition of part-time nurse dedicated to the transition clinic not only allowed for assistance with these follow-up tasks and data collection but also served as an appreciated and useful resource to these young patients. A telephone call from the nurse prior to appointments has been suggested to improve patient attendance. 24 However, in contrast to a general clinic nurse, the dedicated transition clinic nurse became familiar with the transition patients, providing continuity of care. This relationship with patients allowed the nurse to successfully educate patients about their medications, encourage and verify adherence, and explore and address any psychosocial issues. Identification of these issues during phone calls allowed the nurse to provide a summary of such issues to the nephrologist in advance of the clinic visit, facilitating timely treatment and referrals to other specialists, as appropriate. The nurse also helped patients better understand their disease and promoted development of patient responsibility, for example, by encouraging patients to access and follow their laboratory data in a provincial repository. 25 Our experience is in keeping with the literature suggesting that a dedicated nurse should be considered standard for pediatric to adult transition clinics.
Formal establishment of the clinic also helped to facilitate regular communication between the adult and pediatric nephrologists. This is of paramount importance, as it helps to ensure that both teams act uniformly to prioritize issues, treatment plan, and follow-up. Hearing a single message from both teams reduces confusion for patients, potentially improving understanding, confidence to self-manage, and adherence to suggested treatments.
The total number of transition patients was relatively small, and several conditions affecting ~30% of these patients (eg, glomerulonephritis, Alport’s nephritis, tuberous sclerosis, cystinuria, Bartter’s syndrome) fall into the category of “rare diseases” with population prevalences of <1:1500 or <1:2000.26-28 Therefore, assigning these patients to be managed by a single nephrologist allows the nephrologist to gain experience and a deeper understanding of pathogenesis of these rare diseases, their diagnosis and management, and how to handle complications and adverse effects of therapies.26,29 There are several examples of this. Management of relapsing nephrotic syndrome involves prescription of a spectrum of immunosuppressive medications and use of rituximab. 30 The indications for use of rituximab to prevent relapses of proteinuria have been evolving over the past 10 to 15 years and the clinic has been informative on developing practices for initiating and stopping this treatment, and recognizing complications. In glomerulonephritis, the clinic has facilitated conversion of patients from pediatric treatment protocols to adult regimens.31,32 The clinic has enhanced the development of expertise in managing cystinuria, including general preventive measures for stone formation and use of more specific medications, as well as collaboration with a urologist in surgical aspects. 33 Other diseases included management of ADPKD and decision when to initiate tolvaptan in this population, 34 fluid and electrolyte replacement in Bartter’s syndrome, and medical versus surgical management of angiomyolipomas (in patients with tuberous sclerosis). 35 With the advent of next-generation DNA sequencing, genetic testing for diagnostic and prognostic purposes and for family planning plays an increasingly important role in this population. 36 In parallel, there has been increasing collaboration with a medical geneticist to assist with the interpretation of DNA sequencing results. Indeed, with increasing use of genetic testing, monogenic mutations may eventually explain the pathogenesis of at least some of the diseases presently labeled as “acquired,” including some cases of CKD and reflux (Table 1).
Limitations
A limitation of this report is that clinical outcome data were not analyzed systematically for all patients and there is a lack of a comparator group. As noted above, due to the relatively small numbers of patients in the individual disease categories, it was not possible to determine whether attendance of patients in the transition clinic reduced the rate of progression of kidney disease or morbidity. One of the main goals of the transition clinic was to ensure reliable follow-up by providing transition patients with the opportunity to continue their care in the same institution. Interestingly, a substantial number of referred patients (or their parents) did not appear to view this as a priority and switched their care to physicians practicing closer to their homes or did not return for follow-up. Second, due to the clinic structure and the architectural design of the hospitals (lack of waiting room space), it was not possible to establish a system that would group transition patient appointments. This could allow transition patients an opportunity to communicate with each other around the time of their appointments with the supervision of the clinic nurse. For example, with consent, older patients could present their experiences to newly transitioned patients. Moreover, since 2020, such communication was further complicated by COVID-19.
Implications
While there is no universally agreed upon definition of successful transition, the nephrology transition clinic at the Royal Victoria Hospital has been running for almost 16 years and has provided a number of benefits to patients, with only modest financial resources. A key goal of the clinic was to provide transition patients with the opportunity to continue their care in the same institution. 3 The majority of referred patients took advantage of this, but a subset of patients evidently did not view this as a significant priority. In agreements with transition care recommendations, 8 maintenance of accurate records ensured that transfers and discharges of patients were orderly and loss to follow-up was relatively low. A transition care nurse provided useful psychosocial support. 7 By accumulating a critical mass of patients with various rare diseases, the clinic allowed for a greater understanding of disease pathogenesis, the development of specific expertise in diagnosis and management, and a better appreciation of complications, even in the absence of a formal education process. 7 Thus, a dedicated referral, triage, and follow-up process with only modest financial resources and personnel can result in accurate tracking of clinic data, as well as consistent and reliable follow-up and expert patient care.
Among future goals is to employ effective communication and education strategies to promote health literacy and understanding of disease management, based on patient values and preferences. Such approaches have been implemented or recommended in multidisciplinary CKD clinics. 37 Another objective will be to enhance meaningful patient-patient interactions through peer support programs, perhaps under direction of the clinic nurse. Qualitative interviews with patients on their experiences (and testimonials) are a potential avenue that would provide rich information on the benefits and areas for improvement of our clinic. Furthermore, we will look into employing online information portals (or “apps”) for patients who are likely to benefit. These have been useful in providing information, as well as fostering parental interaction, mutual support, and collaboration. 38 A final goal will be to develop a set of quality care indicators, or a “scorecard” that provides more objective measures of the transition clinic processes. 37
Supplemental Material
sj-docx-1-cjk-10.1177_20543581231191836 – Supplemental material for Transition From Pediatric to Adult Nephrology Care: Program Report of a Single-Center Experience
Supplemental material, sj-docx-1-cjk-10.1177_20543581231191836 for Transition From Pediatric to Adult Nephrology Care: Program Report of a Single-Center Experience by Andrey V. Cybulsky, Leonor Cercena, Paul R. Goodyer and Rita S. Suri in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-png-2-cjk-10.1177_20543581231191836 – Supplemental material for Transition From Pediatric to Adult Nephrology Care: Program Report of a Single-Center Experience
Supplemental material, sj-png-2-cjk-10.1177_20543581231191836 for Transition From Pediatric to Adult Nephrology Care: Program Report of a Single-Center Experience by Andrey V. Cybulsky, Leonor Cercena, Paul R. Goodyer and Rita S. Suri in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-png-3-cjk-10.1177_20543581231191836 – Supplemental material for Transition From Pediatric to Adult Nephrology Care: Program Report of a Single-Center Experience
Supplemental material, sj-png-3-cjk-10.1177_20543581231191836 for Transition From Pediatric to Adult Nephrology Care: Program Report of a Single-Center Experience by Andrey V. Cybulsky, Leonor Cercena, Paul R. Goodyer and Rita S. Suri in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-png-4-cjk-10.1177_20543581231191836 – Supplemental material for Transition From Pediatric to Adult Nephrology Care: Program Report of a Single-Center Experience
Supplemental material, sj-png-4-cjk-10.1177_20543581231191836 for Transition From Pediatric to Adult Nephrology Care: Program Report of a Single-Center Experience by Andrey V. Cybulsky, Leonor Cercena, Paul R. Goodyer and Rita S. Suri in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors would like to thank Dr Daria Trojan (McGill University) for helpful discussion.
Ethics Approval and Consent to Participate
The study was approved by the Director of Professional Services and received an exemption from Research Ethics Board review at the McGill University Health Centre.
Consent for Publication
All authors have reviewed the manuscript and consented to publication.
Availability of Data and Materials
Data used in this article were derived from patient medical records. The data source and approval for use has been noted in the article. Requests to access the anonymous aggregate data with the consent of the Research Ethics Board at the McGill University Health Centre can be made by contacting the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The transition clinic nurse was supported by an unrestricted grant from Amgen Canada Inc from 2020 to 2022. A.V.C. and R.S.S were supported by the Catherine McLaughlin Hakim Chair.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.