
Abstract
Background:
With an aging population and growing number of patients with chronic kidney disease (CKD), integrating the latest risk factors when deciding on a treatment plan can result in better patient care. Frailty remains a prevalent syndrome in CKD resulting in adverse health outcomes. However, measures of frailty and functional status remain excluded from clinical decision making.
Objective:
To examine the degree to which different measures of frailty and functional status are associated with mortality, hospitalization, and other clinical outcomes in patients with advanced CKD.
Design:
Systematic review.
Setting:
Observation studies including cohort study, case-control study, or cross-sectional study examining frailty and functional status on clinical outcomes. There were no restrictions on type of setting or country of origin.
Patients:
Adults with advanced CKD, including both types of dialysis patients.
Measurements:
Data including demographic information (e.g., sample size, follow-up time, age, country), assessments of frailty or functional status and their domains, and outcomes including mortality, hospitalization, cardiovascular events, kidney function, and composite outcomes were extracted.
Methods:
A search was conducted using databases Medline, Embase, and Cochrane Central Register for Controlled Trials. Studies were included from inception to March 17, 2021. The eligibility of studies was screened by 2 independent reviewers. Data were presented by instrument and clinical outcome. Point estimates and 95% confidence intervals from the fully adjusted statistical model were reported or calculated from the raw data.
Results:
A total of 117 unique instruments were found among 140 studies. The median sample size of studies was 319 (interquartile range, 161-893). Most studies focused on incident and chronic dialysis patient populations, with only 15% of studies examining non-dialysis CKD patients. Frailty and lower functional status were associated with an increased risk for adverse clinical outcomes such as mortality and hospitalization. The 5 individual domains of frailty were also found to be associated with poor health outcomes.
Limitations:
Meta-analysis could not be performed due to significant heterogeneity between studies and methods used to measure frailty and functional status. Many studies had issues with methodological rigor. Selection bias and the validity of data collection could not be ascertained for some studies.
Conclusion:
Frailty and functional status measures should be integrated to help guide clinical care decision making for a comprehensive assessment of risk for adverse outcomes among patients with advanced CKD.
Registration (PROSPERO):
CRD42016045251
Introduction
The prevalence of chronic kidney disease (CKD) and end-stage kidney disease has been growing, resulting in a greater need for renal replacement therapies including kidney transplantation. 1 Predicting outcomes in patients with CKD is an integral part of clinical care, decision making, and resource allocation. However, this remains a challenge, particularly in those eligible for kidney transplantation. 2 Prediction models have been developed to estimate survival of patients with CKD, assist clinicians with decisions on transplant eligibility, and identify risk factors for adverse outcomes.2 -6 These models have variable predictive performances4 -6 such that there is no standardized, accepted way of determining transplant eligibility.7,8
Frailty and functional status have emerged as novel risk factors associated with adverse outcomes among patients with CKD, subsequently impacting their quality of life and survival.9 -13 Frailty has multiple causes and is defined as an increased state of vulnerability due to decreases in strength, endurance, and physiologic function.14,15 To accurately capture the syndrome of frailty, a comprehensive examination is required. This assessment should encompass the 5 domains that make up the Fried frailty phenotype. 16 Functional status reflects an individual’s ability to perform normal activities to meet their basic needs, maintain their health and well-being, as well as fulfill usual roles. 11 Frailty is highly prevalent among patients with CKD affecting up to 73% of patients on dialysis, and there is an increased risk of lower functional status among these patients.15,17 Despite the growing body of evidence, these risk factors remain excluded from most prediction models for adverse outcomes in CKD patients. Conventional comorbidity assessments do not accurately capture physiological decline associated with frailty and functional status. 18 The purpose of this systematic review was to examine the degree to which different measures of frailty and functional status are associated with mortality and adverse clinical outcomes in patients with advanced CKD.
Methods
The study methodology has been previously reported. 19 This systematic review was conducted in accordance with the guidelines outlined in the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement. 20 This review has been registered in the PROSPERO database (CRD42016045251).
Literature Search
A literature search was conducted using online databases Medline, Embase, and Cochrane Central Register for Controlled Trials. We searched for studies from inception to March 17, 2021, using search terms such as end-stage renal disease, frailty, sarcopenia, functional status, and activities of daily living (Item S1). Eligibility was restricted to articles published in the English language.
Peer reviewed published articles were included if they met our predefined inclusion criteria. Specifically, we included primary research studies that used the following designs: cohort study, case-control study, or cross-sectional study. Case series were included if they had more than 20 participants. Interventional studies were included if the intervention could not have influenced the outcomes of interest. There were no restrictions on length of follow-up, type of setting, or country of origin. Other inclusion criteria were as follows: (a) Population: Adults (≥18 years of age) with CKD stages 4 or 5 (including dialysis patients but excluding kidney transplant recipients and those waitlisted); (b) Instrument: An assessment of frailty or functional status using an instrument that specifically measures overall frailty or functional status or one of their individual domains. Frailty was defined as a syndrome resulting from various factors and contributors characterized by reduced strength, endurance, and physiological function, thus making an individual more susceptible to developing increased dependency and/or mortality. 21 Functional status was defined as an individual’s ability to carry out the normal activities of daily living required to meet basic needs, fulfill usual roles, and maintain health and well-being. 22 Performance-based measures and self-reported measures were accepted; (c) Outcome: Mortality was the primary outcome of interest. We also included other important clinical outcomes such as hospitalization, cardiovascular events, kidney function, composite outcomes (i.e., mortality or need for renal replacement therapy; mortality, hospitalization, or need for renal replacement therapy; mortality or hospitalization; mortality or functional status decline; mortality or cardiovascular disease; in-hospital mortality or discharge to assisted care facility), peritonitis, serious fall injuries, withdrawals from dialysis, discharge from assisted care facility, transplantation, dialysis-related complications, discharge home, and discharge to assisted care facility.
Article selection and data extraction
The eligibility of studies was examined by 2 independent reviewers. Titles and abstracts for all references were screened. Full texts were retrieved for articles passing this initial process, and subsequently screened in greater detail by 2 reviewers. Disagreements regarding the inclusion of studies were resolved by consensus or a third reviewer. The references of included studies were scanned for additional articles, and 2 further studies were included.
A standardized data abstraction form was created and used by reviewers to extract data from the included studies. To minimize any discrepancies, both reviewers compared their extractions to reach consensus. The following data were abstracted from each study: study design, subject characteristics, instrument used to assess frailty and/or functional status, outcomes, and results.
Quality assessment
The methodological quality of the included studies was evaluated using a modified version of the Quality in Prognosis Studies (QUIPS) tool.23 -25 This tool assesses bias through several prompting questions across the following 6 domains: study participation, study attrition, instrument measurement, outcome measurement, study confounding, and statistical analysis and reporting. Each of the 6 domains was rated as having high, moderate, or low risk of bias by one reviewer and verified by a second.
Data analysis and presentation
Results were organized by subgroup of kidney disease: non-dialysis CKD, incident dialysis, and prevalent (chronic) dialysis. Frailty and functional status instruments were analyzed separately as the exposure for each of these subgroups and were grouped based on the domain the instrument was measuring (Box 1). Frailty instruments were classified according to the following domains of frailty: overall frailty, sarcopenia, slow gait, strength measurement, and physical activity and fatigue. 16 Although the World Health Organization’s International Classification of Functioning Disability and Health uses a biopsychosocial model incorporating the impact from environmental, social, and cognitive factors among others to overall functioning and disability, 26 the studies retrieved from our literature search used tools that mostly examined physical measures of functional status. These tools were classified into 3 categories, each of which have established measurement techniques: Activities of Daily Living (ADL),27,28 performance scale, 29 and physical performance. 30
Definition of frailty and functional status and their groupings.

Outcome data were presented by instrument used and clinical outcome. We reported the point estimate and 95% confidence intervals from the fully adjusted statistical model, if available, otherwise the unadjusted estimate was reported. Hazard ratios, relative risks, and odds ratios were obtained directly from the study or calculated from the raw data provided. When studies reported the same measurements in different units, data were converted to the same units mathematically (e.g., studies reporting on the 6-minute walk test were all presented as 100m unit measures). Due to the large degree of heterogeneity between the study populations, instruments used, and study design, we did not statistically pool the results. Finally, main findings from studies were reported as assessments. Multiple assessments of instruments and/or outcomes were possible for 1 article. For example, if a study measured a particular frailty domain using 5 different instruments, this was reported as 5 separate assessments of that frailty domain.
Results
Overview
The literature search identified 7860 unique citations, and 478 articles were assessed for the eligibility criteria at the full-text level. At this stage, a further 338 articles were excluded, resulting in 140 articles included in the review (Figure 1).

Search results and study selection.
The characteristics of the included studies are reported in Table S1 (references available in Item S2). In total, 68 studies used a prospective cohort design and 48 studies performed secondary analysis of established cohorts. Other data sources included hospital records (n = 17) and registry data (n = 7). Publication dates ranged from 1976 to 2021, with a median publication year of 2016. Most studies were from the United States (n = 45), followed by Japan (n = 16), Brazil (n = 10), and Canada (n = 9). Eighty-eight studies (62.8%) exclusively studied chronic dialysis patients with a total sample size of 1,574,214, n = 28 studies (20%) assessed incident dialysis patients accounting for 245,013 patients, n = 21 studies (15%) assessed non-dialysis CKD patients with a sample size of 9923, and 3 studies could not be grouped into any of these single patient populations and therefore categorized as “other” with a sample size of 2342. The overall median sample size of included studies was 319 (interquartile range [IQR], 161-893). Specifically, the median was 306 patients (IQR, 157-835) for chronic dialysis studies, 325 patients (IQR, 183-1516) for incident dialysis studies, 287 patients (IQR, 128-450) for non-dialysis CKD studies, and 907 patients (IQR, 679-946) among studies classified as other.
Instruments
Table S2 describes the frailty and functional status instruments used in the included studies. Overall, 117 unique instruments were reported in 140 studies. There were 91 different instruments that measured frailty across its 5 domains: 29 instruments for sarcopenia (e.g., Appendicular Skeletal Muscle Index) used across 28 studies; 27 for overall frailty (e.g., Fried Frailty Index) across 46 studies; 20 for measuring physical activity and fatigue (e.g., Exhaustion) across 34 studies; 10 for strength measurement (e.g., Handgrip Strength) across 32 studies; and 5 for gait (e.g., Gait Speed) across 19 studies.
There were 26 unique instruments that measured functional status among the included studies. Sixteen functional status instruments for ADL (e.g., Katz ADL) were used across 29 studies; 6 different performance scales (e.g., Karnofsky Performance Scale) were used across 14 studies; and 4 measuring physical performance (e.g., SF-36 Physical Component Summary) were used across 30 studies.
Mortality was the most frequent outcome examined (124 studies), followed by hospitalization (30 studies), cardiovascular events (14 studies), and kidney function (9 studies). Other reported clinical outcomes are listed in Table S3.
Critical appraisal of quality
The quality assessment of the studies is summarized in Table S4. Only 6 studies (4.3%) were assessed as having a low risk of bias across all 6 categories, and 23 studies (16.4%) had a low risk of bias across 5 of the categories. There were 82 studies (58.6%) assessed to have a high risk of bias in at least 1 of the categories. Overall, the studies performed the worst in the statistical analysis and reporting category, with 40 studies (28.6%) identified as high risk of bias in this category.
Mortality
Table 1 provides an overview of the association between various instruments used to measure frailty and functional status and mortality, classified by patient population. The relationship between overall frailty and mortality was analyzed in non-dialysis CKD patients (5 assessments among 5 studies), incident dialysis patients (10 assessments among 6 studies), and chronic dialysis patients (24 assessments among 16 studies). One study examined patients listed in the “other” population category. When analyzed as a categorical variable, being frail was associated with a 2- to 4-fold increased risk of death in most included assessments. The findings were consistent across the different patient subgroups (Figure 2A). The findings were similar when frailty was assessed as a continuous variable (Figure 2B).
Overview of the Association Between Frailty and Functional Status Instruments and Mortality, Classified by Patient Population.

Note. References are available in supplementary material; McClellan, 1991, KPS reported as 0-10, converted to 0-100. ADL = Activities of Daily Living; aHR = adjusted hazard ratio; aOR = adjusted odds ratio; aRR = adjusted relative risk; ASMI = Appendicular Skeletal Mass Index; BI = Barthel Index; BMI = body mass index; BSA = body surface area; BW = body weight; CFS = Clinical Frailty Scale; CI = 95% confidence interval; CKD = chronic kidney disease; CrI = Creatinine Index; DASI = Duke Activity Status Index; ECOG-PS = Eastern Cooperative Oncology Group Performance Status; HD = hemodialysis; HGS = handgrip strength; HR = unadjusted hazard ratio; IADL = Instrumental Activities of Daily Living; KPS = Karnofsky Performance Scale; LMI = Lean Mass Index; LTLM = Limb/Trunk Lean Mass Ratio; LTPA = Leisure Time Physical Activity; MAMC = midarm muscle circumference; MET = metabolic equivalent; OR = unadjusted odds ratio; PASE = Physical Activity Scale for the Elderly; PCS = Physical Component Summary; PD = peritoneal dialysis; PF = Physical Function; POS-S = Palliative Care Outcome Scale–Symptoms; PRISMA = Preferred Reporting Items for Systematic Review and Meta-analysis; RASM = Relative Appendicular Skeletal Muscle; Ref = reference value; SGA = Subjective Global Assessment; SMI = Skeletal Muscle Mass Index; TUG = Timed Up-and-Go Test; RR = unadjusted relative risk; 6MWT = 6-Minute Walk Test.
All models adjusted for a minimum of age and sex, unless otherwise noted. Where a choice of models exists, the most fully adjusted model is presented.
Median.
Multiple adjusted models available.
Model not adjusted for sex.
Converted to years.
Model not adjusted for age or sex.
RR calculated from event data, or cumulative survival event data.
Scale inverted.
Scale change.
Mean.
Unadjusted model.
Reference group and comparator not reported, unit of measure not clearly reported.
Change defined as a clinically relevant decline or improvement.

(A) Forest plot of the association between frailty as a categorical variable and mortality.a (B) Forest plot of the association between frailty as a continuous variable and mortality.a
Twenty-five unique instruments were used to evaluate sarcopenia among 35 assessments. The point estimate for most of the categorical assessments (n = 32 of 34) were above 1.0 suggesting a positive association between the presence of sarcopenia and the risk of death (Figure 3). Effects were similar among both dialysis subgroups; however, a weaker association was noted among non-dialysis CKD patients. One study examined sarcopenia as a continuous measure and did not find a significant association (Figure S1).
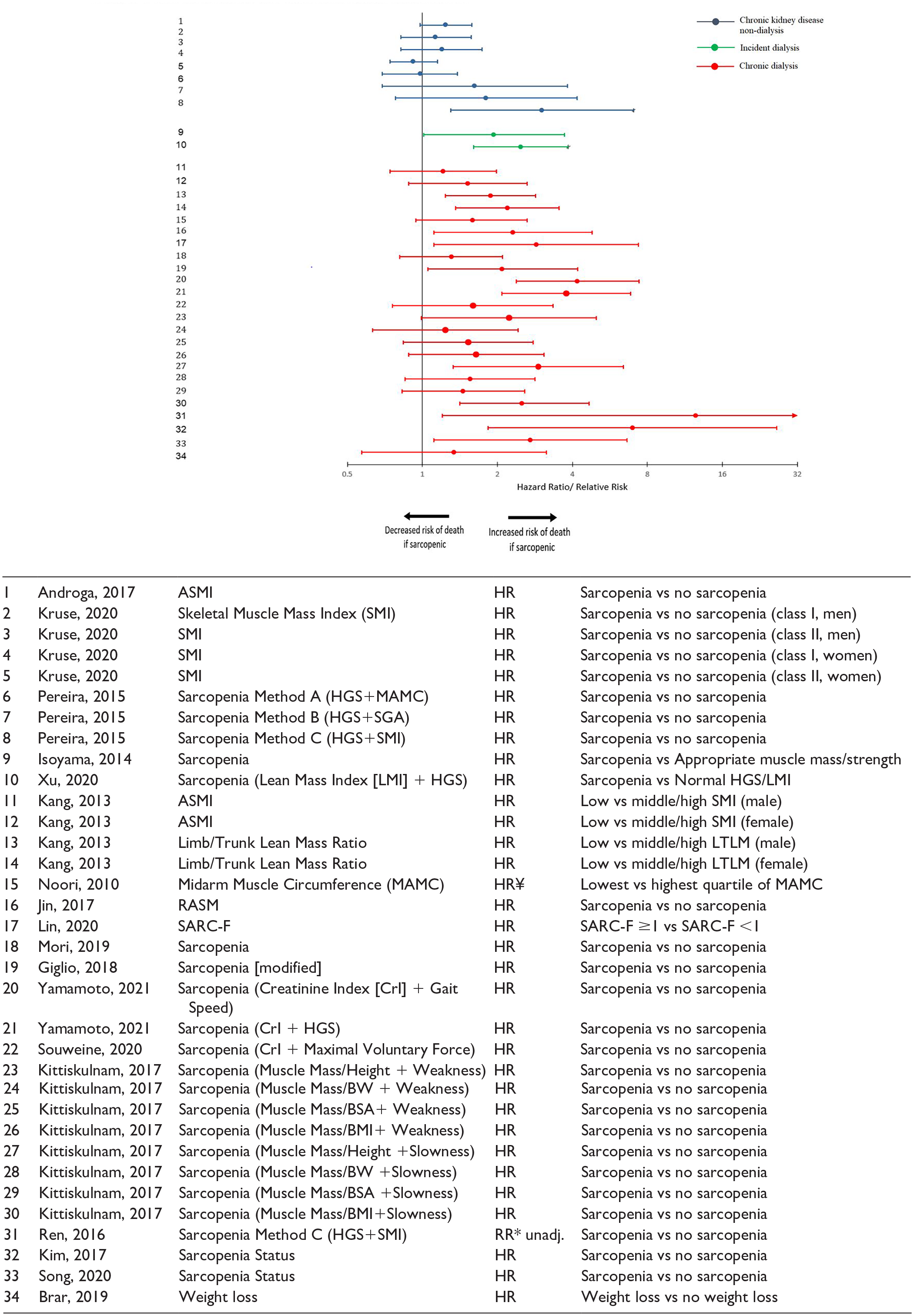
Forest plot of the association between sarcopenia as a categorical variable and mortality.a
The association between frailty’s gait domain and mortality was examined in chronic dialysis patients (11 assessments among 9 studies), non-dialysis CKD patients (7 assessments among 2 studies), and incident dialysis patients (1 assessment among 1 study). Among categorical assessments of gait, most revealed a 2- to 3-fold risk of death consistent across all patient subgroups (Figure 4A). There was also a consistent increased risk of death when gait was examined as a continuous measure (Figure 4B).

(A) Forest plot of the association between gait speed examined as a categorical variable and mortality.a (B) Forest plot of the association between gait speed examined as a continuous variable and mortality.a
There were 33 assessments reported among 20 studies that examined the relationship between strength measurement and mortality in all patient subgroups. Categorical assessments of this frailty domain revealed an increased risk of death among patients with lower strength in nearly all assessments, with most estimates reporting around a 2- to 3-fold risk (Figure 5A). However, when strength was assessed as a continuous variable, risk estimates tended to be lower (Figure 5B). Effects were similar in the dialysis patient subgroups but less so among CKD non-dialysis patients where risk estimates were closer to 1.

(A) Forest plot of the association between strength measurement as a categorical variable and mortality.a (B) Forest plot of the association between strength measurement as a continuous variable and mortality.a
Thirteen unique instruments were used to examine the relationship between physical activity and fatigue and mortality in all patient subgroups. Patients with lower physical activity and increased fatigue had a higher risk of death, with a point estimate between 1.5 and 2 among categorical assessments (Figure S2). All continuous assessments of physical activity and fatigue revealed a positive point estimate above 1, suggesting an increased risk of death (Figure S3).
The relationship between functional status and mortality was reported among 24 assessments in 19 studies. Most studies using categorical assessments of ADL found that patients with lower functional status had an increased risk of death, usually around 2- to 4-fold (Figure S4). Among continuous assessments of ADL impairment, all studies found a positive association between lower functional status and death (Figure S5).
There were 14 assessments among 11 studies that examined the relationship between performance scale and mortality in 3 patient subgroups. A positive association was reported between lower functional status and death. Specifically, a 1.5- to 4-fold increased risk of death was found among studies measuring performance scale as a categorical variable (Figure S6). Similarly, when assessed as a continuous variable, studies tended to show a positive association between lower performance and the risk of death (Figure S7).
Four instruments were used to assess physical performance in 20 studies among incident and chronic dialysis patients. All categorical assessments of physical performance were associated with a 1.5- to 4-fold increased risk of death (Figure S8). When examined as a continuous variable, decreased physical performance was associated with increased risk of death in the vast majority of reported assessments (Figure S9). Results were consistent in both dialysis populations.
Hospitalization
Table 2 provides an overview of the association between various instruments used to measure frailty and functional status and hospitalization, classified by patient subgroup.
Overview of the Association Between Frailty and Functional Status Instruments and Hospitalization, Classified by Patient Population.

Note. References are available in supplementary material. ADL = Activities of Daily Living; aHR = adjusted hazard ratio; aOR = adjusted odds ratio; aRR = adjusted relative risk; aβ = adjusted beta; BADL = Basic Activities of Daily Living; CKD = chronic kidney disease; HD = hemodialysis; HGS = handgrip strength; HR = hazard ratio; IADL = Instrumental Activities of Daily Living; KPS = Karnofsky Performance Scale; PCS = Physical Component Summary; PD = Peritoneal dialysis; Ref = reference; RR = relative risk.
All models adjusted for a minimum of age and sex, unless otherwise noted. Where a choice of models exists, the most fully adjusted model is presented.
Converted to years.
Multiple adjusted models available.
RR calculated from event data, or cumulative survival event data.
Mean.
Scale inverted.
Median.
Unadjusted model.
Model not adjusted for sex.
Discrepancy reported between study data and conclusion.
Model not adjusted for age or sex.
Reference group and comparator not reported; unit of measure not clearly reported.
Scale change.
The relationship between frailty and hospitalization was assessed in 17 studies across all frailty domains in all patient subgroups. There was an approximately 2-fold increased risk of hospitalization among frail patients. This was consistent in the 3 patient subgroups. Frailty examined on a continuous scale also revealed a positive association with the risk for hospitalization (Figure S10). Few studies examined the association between measures of sarcopenia (n = 1, Figure S11), gait speed (n = 3, Figure S12), strength (n = 4, Figure S13), physical activity and fatigue (n = 2, Figure S14) and hospitalization; these studies tended to show a positive association among dialysis patients but revealed a weaker association among non-dialysis patients.
The relationship between functional status and hospitalization was reported among 18 assessments in 10 studies among incident and chronic dialysis patients. In both dialysis subgroups, there was a positive association between lower functional status, by categorical measurement of ADL impairment, and increased risk of hospitalization, around 1.5- to 2-fold (Figure S15). Only 2 studies examined the relationship of performance scale score and hospitalization (Figure S16). Finally, 10 studies assessed physical performance among dialysis patients (Figure S17). Decreased physical performance was associated with increased risk of hospitalization in most studies.
Finally, Table S3 provides additional details on the association of frailty and functional status tools with various other adverse effects.
Discussion
This systematic review identified 140 studies and 117 unique instruments used to examine the association of frailty and functional status with various clinical outcomes in patients with advanced CKD. Most studies focused on incident and chronic dialysis patient populations, with only 15% of studies examining non-dialysis CKD patients. Our study found that frailty was a predictor of mortality among all patient populations. When the specific domains of frailty were examined individually, they were also each found to be associated with mortality. Similarly, lower functional status was also associated with an increased risk of mortality among all patient populations. Parallel trends were noted when examining hospitalization as an outcome. These findings highlight that frailty and lower functional status are risk factors for adverse outcomes in patients with advanced CKD and on dialysis and emphasize the importance of considering them as prognostic metrics among these patients.
Previous systematic reviews have examined the association of frailty status and negative health outcomes in patients with CKD. The prevalence of frailty increases with kidney function decline, and these systematic reviews demonstrate a greater risk for adverse outcomes with frailty such as mortality and hospitalization.9,31 -35 Our findings are consistent with these prior systematic reviews. Our study also assessed the relationship between functional status and adverse outcomes, something which has not been thoroughly considered in prior reviews. Therefore, our findings shed further light onto the significance of functional status in predicting adverse outcomes in CKD while further supporting the importance of frailty as a known prognostic factor.
Patients with advanced CKD often have various physiologic impairments resulting from chronic co-morbidities that are either caused by or associated with CKD. As a result of limited physiologic reserves, patients with CKD are much more susceptible to being frail 36 resulting in a high prevalence of frailty32,37 particularly among those undergoing dialysis, with rates ranging from 14% to 73%. 9 As a consistent predictor for adverse outcomes in CKD, it is not surprising that guidelines recommend evaluating frailty when assessing potential kidney transplant candidates, 38 similar to other factors such as the management of blood pressure and diabetes.39,40 However, in contrast to blood pressure and diabetes management which have clear indicators or adequate control, it remains unclear for both the degree to which frailty is potentially reversible and how interventions aimed at treating frailty may improve outcomes post-kidney transplant. Studies have explored the impact of an exercise intervention in patients prior to transplantation, finding significant improvements in frailty status and a reduction in adverse outcomes.41,42 Other interventions have explored the use of senolytic (removal of senescent cells) drugs and oral nutritional supplements to target frailty in the CKD population.43,44 Furthermore, by focusing on and improving functional status, relief from uremia and kidney failure, kidney transplantation may itself improve frailty. 45 The finding that patient frailty improves following kidney transplant complicates the decision-making process regarding the acceptable level of frailty for surgery. Excessive frailty puts the patient at clear risk for adverse outcomes, however, there is a potential for improvement with enhanced kidney function post-transplant. Additional research is needed to address how frailty should be considered when evaluating patients with advanced CKD for transplant candidacy, an area priority also highlighted by the 2020 KDIGO guidelines. 38
Given that frailty is a complex, multi-dimensional condition where deficits across multiple different domains (physical, cognitive, and social), are at play, the need for consistent and reliable measures for this concept/syndrome are extremely important. As underscored by our study and other systematic reviews,46,47 there is substantial heterogeneity in the tools used to measure frailty. Although the Fried frailty tool is one of the most used frailty measurement tools, 46 the optimal test to use in clinical practice to identify and grade the severity of frailty, particularly in the setting of CKD, has not been identified.48,49 This makes it difficult for clinicians to choose the optimal instrument when evaluating frailty. Most would be considered cumbersome, time-consuming, or require specific tools which would not make them practical for implementation into every day clinical practice, for example, in a dialysis unit or general nephrology clinics. If frailty is to become an important component of clinical care for primary care physicians and nephrologists, finding a practical and valid measurement tool will be crucial. Validation and standardization of frailty tools in patients with advanced CKD would enhance the clinician’s ability to properly counsel patients on their suitability for major medical procedures, but also improve the applicability of future interventions aimed at improving frailty.
Major strengths of our review are its size and broad scope, which increases the clinical applicability of our findings. We examined the effect of all domains of frailty on a variety of clinical outcomes, across all dialysis patients as well as non-dialysis CKD patients. Also, we examined the effect of functional status on adverse outcomes, something prior systematic reviews have not properly characterized. In addition, we did not restrict measurement methods; therefore, numerous instruments measuring functional status and the 5 domains of frailty were included in this review. Nonetheless, this study has limitations. There was considerable variation in methods used to measure frailty and functional status contributing to heterogeneity between studies. As such, conducting a meta-analysis and pooling statistics could not be performed. Second, most studies (n = 72) included in this review used data sources other than a primary cohort, including registry data, hospital charts, or performed secondary analysis of established cohort. This may impact the validity of data collection, assessment of exposure and outcomes, and the potential for selection bias in these studies, thus affecting the validity of the findings in our review. Furthermore, there were issues with the methodological rigor of some studies, as 28.6% of studies were rated as having a high risk of bias. Finally, we only included studies published in English.
Conclusion
Based on the findings summarized in this review, there is evidence to suggest that frailty and lower functional status are predictors of poor clinical outcomes such as mortality and hospitalization among patients with advanced CKD, including dialysis and non-dialysis patients. Our findings highlight the need to assess, monitor, and integrate frailty and functional status measures during clinical care decision making ensuring a comprehensive assessment of risk for adverse outcomes among these patients. Future research should focus on examining these findings among non-dialysis CKD patients, given the paucity of research among this population. Additional research is needed to identify the optimal method for measuring frailty in patients with CKD, and how best to incorporate frailty and functional status assessments in prognosis to guide decision-making surrounding eligibility for certain major medical interventions such as kidney transplant. Finally, studies are needed to identify targeted program initiatives to prevent frailty developing in CKD, treatments for reversal of frailty in CKD, and the role kidney transplantation plays in improving frailty in CKD.
Supplemental Material
sj-pdf-1-cjk-10.1177_20543581231181026 – Supplemental material for Physical Frailty and Functional Status in Patients With Advanced Chronic Kidney Disease: A Systematic Review
Supplemental material, sj-pdf-1-cjk-10.1177_20543581231181026 for Physical Frailty and Functional Status in Patients With Advanced Chronic Kidney Disease: A Systematic Review by Priscilla Karnabi, David Massicotte-Azarniouch, Lindsay J. Ritchie, Shawn Marshall and Greg A. Knoll in Canadian Journal of Kidney Health and Disease
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a peer-reviewed grant from the Canadian Institutes of Health Research (Grant #FDN-143239).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.