
Abstract
Background:
Patients with end-stage kidney disease face high mortality and morbidity after dialysis initiation. Transitional care units (TCUs) are typically 4- to 8-week structured multidisciplinary programs targeted toward patients starting hemodialysis during this high-risk time in their care. The goals of such programs are to provide psychosocial support, provide dialysis modality education, and reduce risks of complications. Despite apparent benefits, the TCU model may be challenging to implement, and the effect on patient outcomes is unclear.
Objective:
To assess a newly created multidisciplinary TCUs’ feasibility for patients newly started on hemodialysis.
Design:
Before-and-after study.
Setting:
Kingston Health Sciences Centre hemodialysis unit in Ontario, Canada.
Patients:
We considered all adult patients (age 18+) who initiated in-center maintenance hemodialysis eligible for the TCU program, although patients on infection control precautions and evening shifts were not able to receive TCU care due to staffing limitations.
Measurements:
We defined feasibility as eligible patients completing the TCU program in a timely fashion without additional need for space, no signal of harm, and without explicit concerns from TCU staff or patients at weekly meetings. Key outcomes at 6 months included mortality, proportion hospitalized, dialysis modality, vascular access, initiation of transplant workup, and code status.
Methods:
The TCU care consisted of 1:1 nursing and education until predefined clinical stability and dialysis decisions were satisfied. We compared outcomes among the pre-TCU cohort who initiated hemodialysis between June 2017 and May 2018, and TCU patients who initiated dialysis between June 2018 and March 2019. We summarized outcomes descriptively, along with unadjusted odds ratios (ORs) and 95% confidence intervals (CIs).
Results:
We included 115 pre-TCU patients and 109 post-TCU patients, of whom 49/109 (45%) entered and completed the TCU. The most common reasons for not participating in the TCU included evening hemodialysis shifts (18/60, 30%) or contact precautions (18/60, 30%). The TCU patients completed the program in a median of 35 (25-47) days. We observed no differences in mortality (9% vs 8%; OR = 0.93, 95% CI = 0.28-3.13) or proportion hospitalized (38% vs 39%; OR = 1.02, 95% CI = 0.51-2.03) between the pre-TCU cohort and TCU patients. There was also no difference in use of home dialysis (16% vs 10%; OR = 1.67, 95% CI = 0.64-4.39), non-catheter access (32% vs 25%; OR = 1.44, 95% CI = 0.69-2.98), initiation of transplant workup (14% vs 12%; OR 1.67; 95% CI = 0.64-4.39), and choosing “do not resuscitate” (DNR) orders (22% vs 19%; OR = 1.22, 95% CI = 0.54-2.77). There was no negative patient or staff feedback on the program.
Limitations:
Small sample size and potential for selection bias given inability to provide TCU care for patients on infection control precautions or evening shifts.
Conclusions:
The TCU accommodated a large number of patients, who completed the program in a timely fashion. The TCU model was determined to be feasible at our center. There was no difference in outcomes due to the small sample size. Future work at our center is required to expand the number of TCU dialysis chairs to evening shifts and evaluate the TCU model in prospective, controlled studies.
Introduction
The increased vulnerability of patients with end-stage kidney disease during the first 3 months of hemodialysis initiation is well known. 1 Transitional care units (TCUs) were developed with this sensitive period in mind and are gaining momentum in Canada and the United States.1 -4 These dedicated care programs aim to bridge the care gaps that exist for incident hemodialysis patients, including dialysis modality education, access creation, and transplant eligibility.3 -6 They also provide more intensive nursing care (ie, 1:2 nurse to patient ratios) and more consistent multidisciplinary care, aiming to reduce the psychosocial burden of dialysis initiation and the corresponding risks of hospitalization and death. 1
Despite these hypothesized benefits of TCUs, studies evaluating TCU models of care for patients starting dialysis remain few in number, with a recent systematic review suggesting the potential for an increased uptake of home dialysis, increased noncatheter access, and reduced mortality. 7 Due to the low rates of home dialysis and noncatheter access at our center, we piloted a TCU in June 2018. Here, we describe our experience along with patient outcomes at 6 months after initiation of dialysis.
Methods
We conducted a before-and-after study at Kingston Health Sciences Centre (KHSC) from June 2017 to March 2019. The KHSC is a tertiary hospital in Ontario, Canada, and the regional renal care program for South Eastern Ontario. Our hemodialysis program serves approximately 400 patients on in-center hemodialysis spread among the main hemodialysis unit at Kingston General Hospital and 7 satellite units. We also have a home dialysis program of 100 patients and perform 25 to 30 kidney transplants annually. We obtained ethics approval from Queen’s University Health Sciences & Affiliated Teaching Hospitals Research Ethics Board prior to study initiation, which waived the need for patient consent.
The KHSC TCU program was designed in 2018 in response to low local rates of home dialysis and noncatheter access, 2 key quality metrics that might be improved by TCUs as shown in previous studies. 4 It is a 4-week program with 1:1 nursing and a multidisciplinary team. Week 1 included pharmacist, social work, and dietician review in addition to nephrologist-driven goals of care and advance care planning discussions. Week 2 included dialysis modality education by a specialized nurse educator with a focus on home dialysis modalities, dialysis access planning, and wound and foot care assessments. Week 3 included transplant eligibility assessment and referral. In the last week, assessment was made of whether predefined clinical stability markers were met, which included achieving dry weight, no incidences of intradialytic hypotension, presence of long-term dialysis plan, and agreement among the TCU multidisciplinary team that the patient was stable and ready for transfer out of the TCU at a weekly meeting. Once these parameters were satisfied, patients transferred to the main hemodialysis unit, satellite hemodialysis unit, or started home dialysis training based on their goals of care.
We considered all adult patients (age 18+) who initiated in-center maintenance hemodialysis eligible for the TCU program, including those switching from a previous renal replacement therapy such as peritoneal dialysis and transplantation. Cognitively impaired and frail patients were also considered eligible for TCU care as they were felt to still benefit from home dialysis modalities such as assisted peritoneal dialysis. 8 Patients on infection control precautions and evening shifts were not able to receive TCU care due to staffing limitations. The TCU program was implemented in June 2018. We compared outcomes among a pre-TCU cohort who started dialysis between June 2017 and May 2018 and TCU patients who initiated dialysis between June 2018 and March 2019. The post-TCU time period was further divided into patients who entered the TCU program and those who were unable to join the program (eg, no shift or nurse available), with outcomes also compared between these 2 groups.
We defined feasibility of the TCU model at our center as enrolled patients completing the TCU program in a timely fashion without additional space required, no signals of harm (ie, mortality, hospitalization), and without explicit concerns from TCU staff or patients at weekly meetings. Key outcomes measured at 6 months after initiation of hemodialysis included mortality from any cause, proportion hospitalized (defined as nonelective hospitalizations), dialysis modality, dialysis access, initiation of transplant workup (defined as one documented visit with a transplant nephrologist indicating clearance to start transplant work up), and code status (defined as the patient’s wishes regarding resuscitative measures in the setting of cardiac arrest).
We summarized baseline characteristics using descriptive statistics. We expressed continuous variables as the mean (standard deviation, SD) or median (lower quartile (Q1) – upper quartile (Q3)) and categorical variables as frequencies (proportions). For each outcome, we also calculated unadjusted odds ratios (ORs) and 95% confidence intervals (CIs).
Results
From June 2017 to May 2018, 115 patients started in-center hemodialysis (pre-TCU), and from June 2018 to March 2019, 109 patients started in-center hemodialysis (post-TCU). Of these 109 patients, 49 (45%) entered and completed the TCU. The most common reasons for not participating in the TCU included evening hemodialysis shifts (18/60, 30%) or contact precautions (18/60, 30%). Other reasons included a combination of availability of TCU chairs, nursing availability, and patient transportation challenges. Baseline characteristics were largely similar between the pre-TCU and post-TCU groups, including predialysis care, defined by any visit to our multidisciplinary chronic kidney disease clinic in the preceding 12 months (73% vs 65%). However, diabetes mellitus as a cause of end-stage renal disease was more common in the pre-TCU group (Table 1).
Baseline Characteristics and 6-Month Outcomes for Patients Newly Started on ICHD.
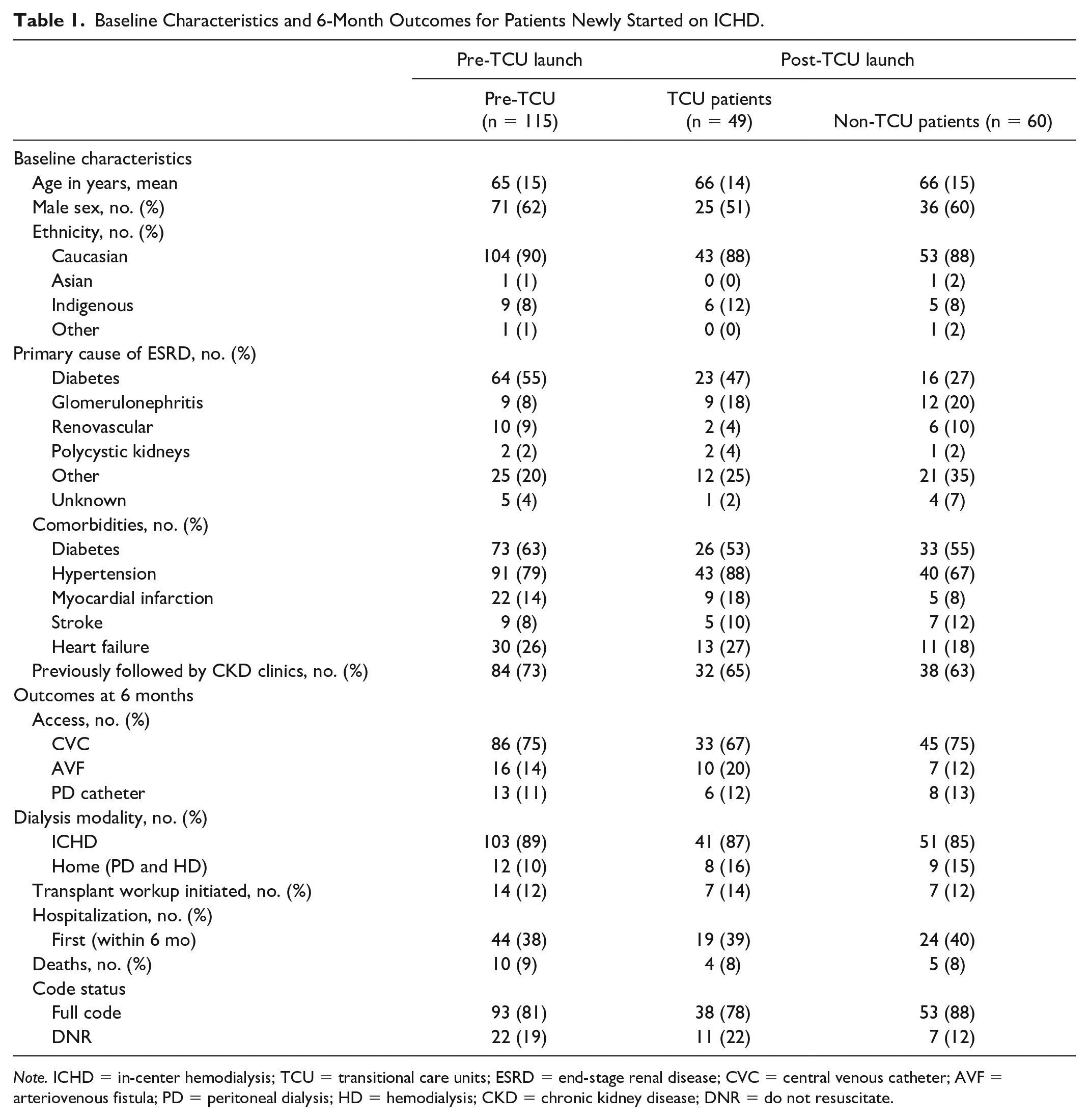
Note. ICHD = in-center hemodialysis; TCU = transitional care units; ESRD = end-stage renal disease; CVC = central venous catheter; AVF = arteriovenous fistula; PD = peritoneal dialysis; HD = hemodialysis; CKD = chronic kidney disease; DNR = do not resuscitate.
Of the 49 patients who entered the TCU, all completed the program in a median of 35 (25-47) days. All 49 patients received 1:1 nursing care for the duration of the program and were cared for in the main dialysis unit without the need for additional physical space. Informal comments at weekly multidisciplinary team meetings were positive of the new model of care.
We observed no differences in mortality (9% vs 8%; OR = 0.93, 95% CI = 0.28-3.13) or proportion hospitalized (38% vs 39%; OR = 1.02, 95% CI = 0.51-2.03) between pre-TCU and TCU patients. There were also no statistically significant differences in choosing home dialysis (16% vs 10%; OR = 1.67, 95% CI = 0.64-4.39), having noncatheter access (32% vs 25%; OR = 1.44, 95% CI = 0.69-2.98), initiating transplant workup (14% vs 12%; OR = 1.67, 95% CI = 0.64-4.39), and choosing “do not resuscitate” DNR orders (22% vs 19%; OR = 1.22, 95% CI = 0.54-2.77) (Table 1).
When we compared post-TCU patients who did and did not enter the TCU, the outcomes for non-central venous catheter (CVC) access (32% vs 25%; OR = 1.45, 95% CI = 0.63-3.35) and initiating transplant workup (14% vs 12%; OR = 1.48, 95% CI = 0.49-4.41) were similar to the pre-TCU versus TCU patient analysis. There were also no differences observed in the post-TCU launch cohort between patients who entered the TCU and those who did not participate in the TCU with respect to choosing home dialysis (16% vs 15%; OR = 1.11, 95% CI = 0.39-3.12) and choosing DNR orders (22% vs 12%; OR = 2.19, 95% CI = 0.78-6.17) (Table 1).
Discussion
Our small before and after study demonstrates that our TCU model is feasible to institute without additional dedicated space and with some redistribution of nursing resources for the 4- to 5-week duration of the program. All patients who entered the TCU completed the program in a timely fashion without explicit concerns from TCU staff or patients. These initial experiences support continuation and expansion of the TCU model at our program, as we await a large sample size to adequately assess patient outcomes, experiences, and cost-effectiveness.
While our sample size was underpowered for clinical outcomes, other dedicated care programs found modest effects on home dialysis and non-catheter access.4,9,10 For example, the systematic review by Attalla and colleagues reported that TCUs increased the odds of home dialysis fourfold and the odds of arteriovenous access twofold, although pooled analysis was not possible due to study heterogeneity. 7
There was initial concern that patients would spend too much time in the TCU and consume nursing resources for several months, but this rarely occurred. Most patients completed the pathway in just over 1 month, and few patients could not enter the TCU due to lack of nursing availability (outside of evening shifts). Although patient and staff feedback was not formally collected, unsolicited comments were highly positive of the TCU experience.
Strengths of our work include the comparison of all incident patients on maintenance hemodialysis over a 2-year period and the availability of goals of care data that are often missing from similar TCU program reporting. We hypothesized that DNR status could increase in the TCU model due to planned nephrologist-led goals of care discussions in week 1. Our study also has limitations. These include the small sample size, potential for selection bias, and lack of multivariable adjustment. While isolation precautions and evening hemodialysis were limiting factors for TCU participation at our center, they may not be in other TCU models at other sites. Furthermore, despite similar baseline characteristics, it is possible that TCU patients were inherently different on several unmeasured factors such as self-management, caregiver support, and adherence.
Based on these initial results, future directions for our TCU program include expanding availability of the TCU to more patients, especially those on evening hemodialysis shifts and under infection control precautions. Future areas of study for our program include evaluation of the physical and emotional functioning of patients as a result of TCU care.
Conclusions
We found that a goal-directed multidisciplinary TCU model with 1:1 nursing care was a feasible program to institute for incident patients in our hemodialysis unit without additional physical space. Future studies adequately powered to detect clinical significance and cost-effectiveness are needed to assess the impact of the TCU model on robust patient outcomes. Potential evaluation strategies should be pragmatic, considering stepped-wedge and registry-based designs, both of which have been successfully used in the hemodialysis population.11,12
Footnotes
Acknowledgements
The authors thank the TCU nurses at Kingston General Hospital for their work in implementation of the TCU program.
Ethics Approval and Consent to Participate
Ethics approval was obtained from Queen’s University Health Sciences & Affiliated Teaching Hospitals Research Ethics Board prior to study initiation which waived the need for patient consent.
Consent for Publication
All listed authors provided consent for publication of this work.
Availability of Data and Materials
Data and materials may be made available upon written request to the corresponding author. Reasonable requests for data access will be assessed in consultation with the appropriate Research Ethics Boards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.