
Abstract
Background
Home dialysis therapies have limited uptake in most regions despite recognized benefits such as increasing patients’ independence, and several domains of quality of life with cost savings in some systems.
Objective
To perform a scoping review of published literature to identify tools and guides used in systematically screening and assessing patient suitability for home dialysis. A secondary objective was to explore barriers and enablers associated with the home dialysis assessment process. It is important to identify gaps in current research to pose pertinent questions for future work in the field.
Design
Online databases Embase, Medline (Ovid), and CINAHL were used to identify articles published between January 2007 to May 2023. A total of 23 peer-reviewed primary and secondary studies that investigated screening or selection for patients > 18 years old with kidney failure for home dialysis met the study inclusion criteria.
Results
The studies consisted of secondary studies (n = 10), observational studies (n = 8), and survey-based studies (n = 5). The major themes identified that influence patient screening and assessment for home dialysis candidacy included: screening tools and guidelines (n = 8), relative contraindications (n = 4), patient or program education (n = 9), and socioeconomic factors (n = 2).
Limitations
Consistent with the scoping review methodology, the methodological quality of included studies was not assessed. The possible omission of evidence in languages other than English is a limitation.
Conclusion
This scoping review identified tools and factors that potentially guide the assessment process for home dialysis candidacy. Patient screening and assessment for home dialysis requires a comprehensive evaluation of clinical, psychosocial, and logistical factors. Further research is required to validate and refine existing tools to establish standardized patient screening criteria and evaluation processes. Up-to-date training and education for healthcare providers and patients are needed to improve the utilization of home dialysis and ensure optimal outcomes.
What was known before
Home dialysis therapies are underutilized and there is a wide discrepancy as to how patients are screened and assessed for initiation of home dialysis, 1 and whether standardized tools or processes are used or not. 2
What this adds
This scoping review comprehensively searches the available literature for the tools and guides for systematic screening and comprehensive assessment of suitable patients and barriers and enablers for home dialysis. This provides updated knowledge and understanding of the process, suggests alignment of practice with contemporary data as well as directions for future research.
Introduction
The escalating burden of kidney failure, with initiatives to increase home dialysis use in the United States, has increased emphasis on home dialysis therapies which include peritoneal dialysis (PD) and home hemodialysis (HHD).3,4 Home dialysis offers patients with kidney failure an opportunity for increased autonomy and treatment satisfaction without any clear differences in clinical outcomes in comparison to facility-based hemodialysis (HD).5,6 Despite its recognized benefits, home dialysis has remained underutilized in many jurisdictions except for those who have implemented PD-first policies like Hong Kong. In Canada, where a home dialysis preferred policy is adopted rather than a mandatory PD-first policy, similar to Australia, New Zealand, and multiple Scandinavian countries, the prevalence rates for home dialysis are static at 17% for PD and 3% for HHD.1,5 While acknowledging that not all patients are equally suited for home dialysis, there is a critical need to update our understanding of the optimal process of identifying and evaluating individuals for home dialysis. 1 Using a systemic process to assess suitable candidates who can successfully be maintained on home dialysis can provide more effective and accessible care.
The primary objective of this scoping review was to conduct a systematic examination of existing literature to identify tools and guides utilized in the screening and assessment of patients for home dialysis by healthcare providers. Patient decision aids and tools used in the process of shared decision making were not included in this review. A secondary objective was to explore potential barriers and enablers associated with the modality suitability evaluation process.
Methods
We performed a scoping review of peer-reviewed literature on screening and assessment of patients for home dialysis based on the methodological framework proposed by Arksey and O’Malley. 7 The review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews (PRISMA-ScR) checklist guidelines.8,9 Scoping reviews were not accepted on PROSPERO (the NIH International Prospective Register of Systemic Reviews) for registration at the time this article was prepared (https://www.crd.york.ac.uk/prospero/).
Search strategy
To identify relevant articles the following bibliographic databases were searched from January 2007 to 18 May 2023: Medline (OVID), EMBASE, and CINAHL. The search strategies were drafted in consultation with an information specialist (VK) and further refined through team discussion. A pretested combination of keywords and MESH terms were used based upon the identified core concepts of the research question: (1) Patient screening/assessment; (2) Peritoneal Dialysis; and (3) Home Hemodialysis. The search strategy was first developed using Medline (OVID) and translated to other databases using each database platform's subject headings and appropriate fields (Supplemental Appendix A for Medline search strategy). Only studies published after January 2007 were examined as it was this period that home dialysis became more widely used for kidney failure treatment and policies and practices development began. 10
Study selection
Inclusion and exclusion criteria
Eligibility criteria were established based on the research question. All types of peer review articles that fulfilled the following criteria were included: (i) patients aged ≥ 18 years suffering from kidney failure, (ii) screening or assessment of patients for dialysis, (iii) dialysis at home or in a long-term care center, (iv) studies indicating facilitators or barriers for home dialysis, (v) full-text studies, and (vi) articles published in English or translated to English.
Articles excluded from this study were: (i) palliative or pediatric patients suffering from kidney failure; (ii) patients suffering acute kidney failure requiring dialysis; (iii) other kidney replacement therapies, including kidney transplantation or conservative management; and (iv) abstracts, unpublished thesis, books, and conference summaries.
Screening
All the retrieved records from the databases were imported into the Zotero reference management database (version 5.0 Corporation for Digital Scholarship, Roy Rosenzweig Center for History and New Media, George Mason University, Fairfax, VA, USA). The records were then converted into an RIS format for importation into Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia (available at www.covidence.org) which was used for screening. Two reviewers (RT and MB) independently conducted screening and selection for inclusion using the inclusion criteria described below. Both reviewers also screened full-text articles. A third reviewer (AL) was available to resolve any unresolved discrepancies.
Data extraction, summary, and reporting of results
The following information was independently extracted for all included studies by three reviewers (RT, MB, and LN) using a standardized form and entered in a Microsoft Excel spreadsheet: author, title, source, year of publication, country of the corresponding author, type of dialysis modality, study design, data collection method, number of participants, gender, age range, and key findings. We did not assess study quality given the focus of our scoping review.
Data in the literature regarding patient screening and assessment for home dialysis were analyzed qualitatively using both deductive (preidentified themes) and inductive (newly identified themes) approaches.
Results
The search strategies identified a total of 3693 citations. Of these, 23 articles met the inclusion criteria and were eligible for this scoping review. Figure 1 summarizes the search results and study selection in an adapted PRISMA-ScR flow diagram. 8
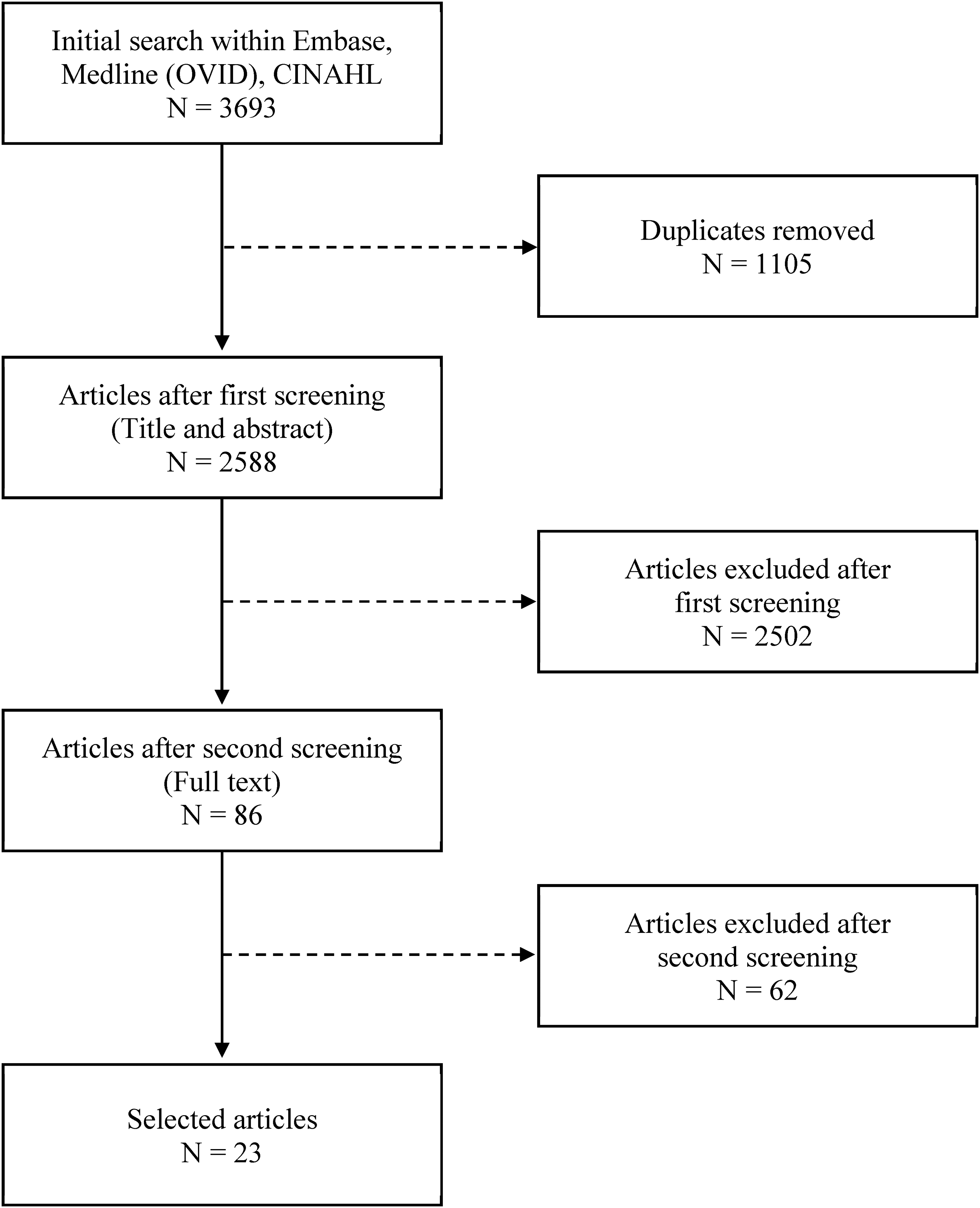
Summary of the search results and study selection in an adapted PRISMA-ScR flow diagram. 8
Study characteristics
The included articles were conducted in 11 different countries: however, most originated from Canada (n = 10, 43%). Fourteen of the included studies focused exclusively on PD, five studies focused exclusively on HHD, and four studies investigated both PD and HHD. Of the primary studies, 8 were observational studies (35%) and 5 were survey-based studies (22%) (Table 1). Ten studies were review articles (43%) (Table 2).
Characteristics of primary studies included in the scoping review (N = 13).
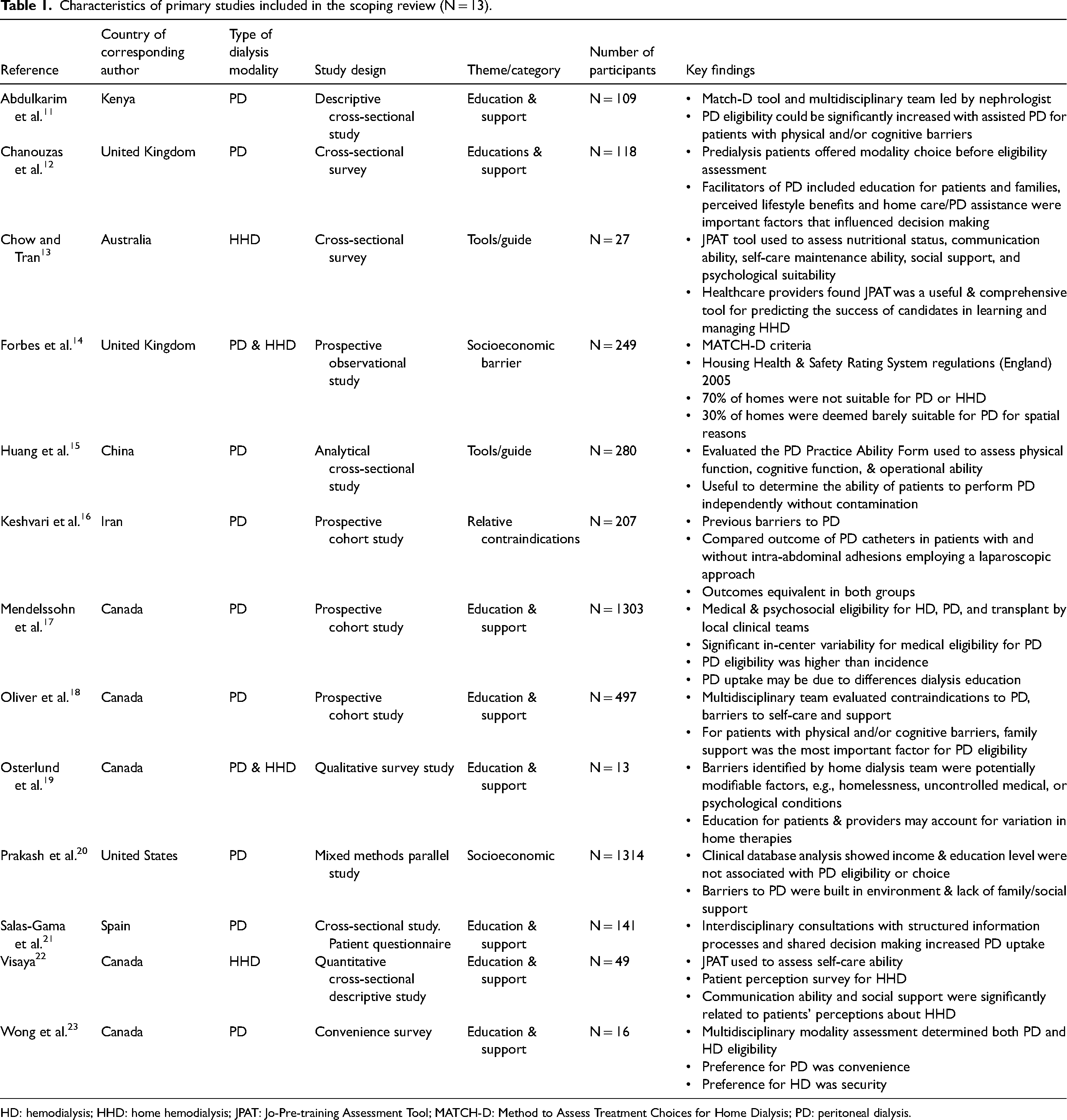
HD: hemodialysis; HHD: home hemodialysis; JPAT: Jo-Pre-training Assessment Tool; MATCH-D: Method to Assess Treatment Choices for Home Dialysis; PD: peritoneal dialysis.
Characteristics of secondary studies included in the scoping review (N = 10).

CKD: chronic kidney disease; ID: identify; HD: hemodialysis; HHD: home hemodialysis; KRT: kidney replacement therapy; MATCH-D: Method to Assess Treatment Choices for Home Dialysis; PD: peritoneal dialysis; PEG: percutaneous endoscopic gastrostomy.
Screening tools and guides
Eight articles described the utilization of screening tools and/or guides to aid decision making for home dialysis suitability. Of these, three analyzed tools that could be used to screen for suitable home dialysis candidates. Schatell 10 developed the Method to Assess Treatment Choices for Home Dialysis (MATCH-D) tool to identify candidates appropriate for home dialysis as well as to provide a framework for determining potential obstacles and strategies for transitioning to home dialysis. 10 Chow et al. 13 evaluated the applicability of the Jo-Pre-training Assessment Tool (JPAT) for predicting the success of candidates in learning and managing HHD. Huang et al. 15 evaluated the PD Practice Ability Form which assesses patients’ ability to perform PD independently.
Rioux et al. 30 provided a guide that reviewed best practices for the implementation of an HHD training program. Ibrahim et al. 27 provided reasons to prescribe HHD and a practical guide for managing kidney failure with HHD. Blake et al. 25 provided a guide for the process of PD suitability assessment and initiation. The authors discovered that variations in either offering patients the option to choose a treatment method or the absence of clearly defined criteria for eligibility led to a decrease in the use of incident PD. 25 Tregaskis et al. 32 provided a guide and indicated important assessments required for decision making before PD initiation. A review by Torreggiani et al. 31 provided a practical guide for the optimal choice of kidney replacement therapy (KRT) highlighting the pros and cons of each modality.
Relative contraindications
Relative contraindications to PD were discussed in four articles. Keshvari et al. 16 demonstrated successful laparoscopic placement of PD catheters in patients who were previously excluded from PD due to a history of abdominal surgeries. Lee et al. 29 found that most medical contraindications were not barriers to successful PD. In a review, Bargman et al. 24 concluded that many previously believed absolute contraindications for PD are no longer relevant, and PD provided similar or better survival than HD in patients with obesity, immunosuppression, and cirrhosis. Recently, Eroglu et al. 26 also determined many comorbidities, previously perceived as absolute contraindications to PD, could be overcome with few complications.
Education and support
Education and caregiver support systems, for patient decision making and home dialysis suitability, were the central theme in nine of the identified articles. Osterlund et al. 19 reported education by providers as well as provider training could account for variance in home dialysis rates among different programs. Mendelssohn et al. 17 found centers in the US rated more patients eligible for PD than Canadian centers; however, there was a higher incidence of PD in Canada attributed to educational programs provided to patients by multidisciplinary predialysis care. Chanouzas et al. 12 determined that patients with predialysis education and a strong social support network were more likely to choose PD versus in-center HD or conservative management. Salas-Gama et al. 21 indicated better patient education about dialysis modalities and shared decision making could potentially double the number of patients accepting PD. Koester 28 examined staff and patient education and patient selection, concluding that the low incidence of HHD was related to the few individuals with CKD being provided with comprehensive modality information.
Four articles discussed the importance of caregivers as treatment support for PD. Wong et al. 23 found older patients with kidney failure felt more secure selecting in-center HD versus PD. Oliver et al. 18 showed that patients, especially those with barriers to self-care, tended to choose PD if a family member was available for support. Similarly, Abdulkarim et al. 11 determined that older patients with physical and cognitive barriers could be eligible for PD if family support or home care assistance was available. This was supported by Visaya et al. 22 showing that the ability to communicate with the healthcare team and the availability of social support were the main factors related to a patient's choice regarding HHD.
Social economic considerations/challenges
Two articles addressing socioeconomic inequities in home dialysis were identified. Forbes et al. 14 determined in a local audit of patients deemed medically suitable for home dialysis using MATCH-D criteria, 67% of their homes were unacceptable for home dialysis implementation. Prakash et al. 20 found income and education were not significantly associated with PD eligibility or choice, however, lower-income patients had more barriers in terms of their physical or social environment and available family or social support.
Discussion
This scoping review provides an overview of the literature concerning patient screening and suitability assessment for home dialysis, focusing on the period from January 2007 to May 2023. Before 2007, a consistent framework to assess PD and HHD eligibility had not been developed. 10 Almost half of the articles included originated from Canada. This possibly reflects the relatively high overall home dialysis usage due to a government-funded healthcare system, improved access to predialysis education, and more home dialysis exposure by treating physicians. 33 There has been an increase in publications postpandemic which suggests renewed interest in home dialysis, especially since there is a notably lower incidence and mortality rate of COVID-19 in individuals undergoing dialyzing at home compared to facility-based HD.31,34
Screening tools and guides
The predominant approach to patient selection for home dialysis involved a nephrologist, often in collaboration with a multidisciplinary team. In our review, a limited number of guides for evaluating patient eligibility for home dialysis were identified. Of these, two guides were specifically designed for assessing PD suitability,25,32 three guides were tailored for HHD,27,28,30 and one guide was applied to both PD and HHD. 31 Similarly, a limited number of screening and assessment tools were identified, these included MATCH-D, JPAT, and PD practice ability. The MATCH-D criteria was the most frequently referenced screening tool across the various studies,10,11,14,15,19,30,32 with two studies utilizing MATCH-D to help determine patient eligibility.11,14 The MATCH-D tool lacked a clear distinction between contraindications and barriers to PD self-care. 15 The PD Practice Ability tool was specifically developed to assess the self-care ability of PD patients. 15 The JPAT tool demonstrated utility as both an adjunct to MATCH-D for evaluating HHD suitability and as a tool to assess the resources required for patient training.13,32 Another application of the JPAT was its use in evaluating a patient's self-care ability for HHD. 22
Similarly, there was a lack of comprehensive descriptions of the systematic evaluation of patient eligibility for home dialysis. The determination of eligibility for patients undergoing assessment for home dialysis has demonstrated variability.2,19,25 These differences may be attributed, in part, to diverse perceptions and biases within the nephrology team.2,19,25 The widespread implementation and adherence to a standardized multidisciplinary process could contribute to achieving more consistent and equitable decision making across healthcare settings.25,31 This approach not only has the potential to ensure that all eligible patients are offered home dialysis but also facilitates a timely transition to alternative dialysis modalities if the initial modality proves unsuccessful. 30
Relative contraindications
Regarding relative contraindications, the decision of modality eligibility can vary between different healthcare providers based on expertise and practice patterns. 24 A recent survey of physicians indicated an overall decline in confidence regarding knowledge and experience in caring for patients undergoing PD when compared to in-center HD.35,36 Assessments of physician knowledge revealed a discrepancy between perceived and actual knowledge, particularly concerning contraindications to PD. 35 Recent studies reported obese individuals starting on PD had similar outcomes as nonobese individuals and therefore, obesity should not be considered a contraindication to PD.37,38 These findings underscore persistent misconceptions across medical specialties regarding which individual is deemed a “suitable” candidate for PD and the need to enhance and maintain education for providers, focusing on PD candidacy and the advantages associated with transitioning to home dialysis.24,35 This targeted education is crucial for dispelling misconceptions, building competence and confidence, and eliminating bias education thereby fostering a more informed, modern approach to the utilization of PD. 35
Education and support
Another important aspect of the screening and selection process involves the identification of patients who demonstrate an inclination for active participation in their treatment. Therefore, acknowledging and incorporating patients’ preferences, as well as fostering shared decision making between healthcare providers and patients concerning home dialysis becomes essential.24,26,31,35 Empirical evidence indicates that satisfaction, compliance with therapy, and overall quality of life are improved when individuals are allowed to make informed decisions.24,26,31,35 The provision of predialysis education promotes informed decision making, and empowers individuals to actively engage in their healthcare, make necessary lifestyle adjustments and seek appropriate support, which ultimately contributes to favorable home dialysis outcomes.18,20,31 Although models of patient education and decision aids were outside the scope of this review, evidence indicates that structured education to support shared decision making, coupled with a robust social support network, have been associated with an increase in the number of individuals opting for home dialysis.18,36
Socioeconomic considerations/challenges
In addition to educational considerations, psychosocial and socioeconomic considerations are crucial for successful home dialysis outcomes. Family support was found to be the most important factor for patients who were not able to self-manage their treatment. 18 Moreover, PD eligibility and choice demonstrated no association with socioeconomic status, housing conditions, and caregiver availability as primary socioeconomic barriers.14,20 Recognizing and overcoming these psychosocial and socioeconomic barriers is important for the healthcare team to facilitate a successful transition to PD. This involves providing counselling on resources to manage stress, establishing connections between patients and their families with patient peer mentors, and ensuring comprehensive support system networks. 31
Limitations and direction for further studies
Limitations of this scoping review included the possible omission of evidence in languages other than English. Also, consistent with the scoping review methodology, the methodological quality of the included studies was not formally assessed.
Several gaps in the current literature on patient screening and assessment for home dialysis suitability were identified (Figure 2). This included limited studies specifically evaluating the effectiveness of screening criteria or tools in predicting patient outcomes. There is a need for more robust studies examining long-term treatment adherence, quality of life, and healthcare resource utilization in patients identified as home dialysis candidates using available guides. Additionally, there is a lack of studies addressing optimal screening specifically for HHD. Also, little has been published on patient screening and assessment in the context of guiding patients to overcome existing socioeconomic barriers to implementing home dialysis.

Guidance for future research on evaluating patients for home dialysis eligibility.
Conclusion
The literature describes multiple barriers to the widespread implementation of home dialysis, including lack of education of patients and health care providers, socioeconomic factors, and the importance of exposure to these in the context of shared decision making to enhance home dialysis adoption. Tools to evaluate or screen for PD or HHD exist, but evidence of their regular use and value relative to nonuse is lacking. Further research is required to standardize, refine, and validate the current screening and suitability assessment processes and re-evaluate the optimal type, timing, and interval for education about home dialysis for providers. Ideally, a clear up-to-date patient education pathway (addressing PD and HHD) with consistent screening criteria, well-informed interdisciplinary support and care partner involvement will allow for collaborative decisions and patient empowerment, mitigate bias and best identify a patient population suitable for home dialysis.
Footnotes
Acknowledgements
We would like to acknowledge Vanessa Kitchin at the University of British Columbia Library for her support in designing our database search strategy.
Authorship
RT and MB conceived the review and independently conducted screening and selection for inclusion using and also screened full-text articles. AL was available to resolve any unresolved discrepancies. RT, MB, and LN extracted data for the review. All authors were involved in writing up the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.