
Abstract
Background:
Compatible pair participation in kidney paired donation (KPD) may increase the likelihood of finding suitable matches for all registered pairs. Retrospective studies have shown variable enthusiasm for participating in KPD in compatible pairs.
Objective:
The study objective was to gather potential living donor (PLD) and transplant candidate (TC) perspectives on compatible pair participation in KPD.
Design:
Surveys and qualitative interviews.
Setting:
Three transplant programs in Canada: Centre hospitalier de l’Université de Montréal in Montreal (Québec), Vancouver General Hospital, and St. Paul’s Hospital in Vancouver (British Columbia).
Patients:
Both PLDs and TCs undergoing evaluation for donation/transplantation between 2016 and 2018 at 3 transplant programs in Canada.
Methods:
Descriptive statistical analysis was performed for the results of the survey and thematic and content analysis method was used for the content of the qualitative interviews.
Results:
A total of 116 PLDs and 111 TCs completed surveys and an additional 18 PLDs and 17 TCs underwent semi-directed interviews. Of those surveyed, 61.2% of PLDs and 76.6% of TCs reported a willingness to participate in KPD as a compatible pair. The possibility of a more optimally matched kidney for the TC and policies ensuring prioritization of the TC for repeat transplantation in the event of early graft failure increased willingness to participate in KPD. Major concerns expressed during the interviews included the desire to retain the emotional bond of directed donation, the fear of chain breaks or donor reneging, delays in transplantation, and additional travel associated with participation in KPD.
Limitation:
The limitations of this study are that it was conducted in only 3 Canadian transplant programs and that the interviews and surveys were in French and in English. As a consequence, the results may not be reflective of the views of individuals not living in these 2 provinces and from ethnic minority populations.
Conclusion:
Most of the compatible PLDs and TCs surveyed were willing to participate in KPD. Ensuring timely transplantation and a more optimal match for TCs and offering a policy of reciprocity to ensure timely repeat transplantation for compatible recipients if their allograft fails post KPD transplant may further increase compatible pair participation in KPD.
Introduction
Kidney paired donation (KPD) is a strategy for enabling living-donor kidney transplantation (LDKT) by matching incompatible pairs. In Canada, the national KPD program was developed in 2009.1-3 As of December 10, 2020, 765 kidney transplantations had been performed through the Canadian KPD program. 2 Despite the successes of KPD programs, some incompatible pairs are unable to find a match: only 38% of recipients with a blood group–incompatible donor and 45% of recipients with an HLA-incompatible donor have been transplanted in Canada’s national program. 3
Increasing the number of registered pairs significantly improves the yield from KPD by increasing the percentage of registry matches, particularly among the most difficult-to-transplant candidates.4,5 In 2010, Ratner and colleagues first described the participation of 2 compatible pairs in a kidney chain and reported a certain ambivalence toward participating as a compatible pair in KPD. 6 In 2012, Bingaman et al 7 reported the participation of 17 compatible pairs in their kidney exchange programs, and, more recently, Weng et al 8 described the participation of 11 compatible pairs in their single-center KPD program.
In Canada, there are no current recommendations to guide the participation of compatible pairs in KPD. 9 A survey of prior living kidney donors and transplant recipients in British Columbia (BC) showed that more than 90% of living donors and transplant recipients were willing to participate as compatible pairs in KPD. 10 However, these data are limited by the fact that those individuals had already successfully donated or received a transplant and were commenting on a hypothetical scenario. Their past experience with donation could create a cognitive bias in favor of participation in KPD. Also, participants in this study did not have the opportunity to explain in-depth their perspectives and rationale behind their willingness, or lack of willingness, to participate. No study has prospectively explored the perspectives of potential Canadian potential living donors (PLDs) who have not yet donated and TCs who have not yet received a transplantation on the participation of compatible pairs in KPD. Their perspectives are of paramount importance in designing or implementing an acceptable program for them. The objective of this study was to use mixed methods (through surveys and qualitative interviews) to prospectively gather PLD and transplant candidate (TC) perspectives on participating in KPD as compatible pairs, to inform the feasibility of enrollment of compatible pairs in KPD and the development of national policies in the Canadian KPD program.
Materials and Methods
Mixed methods were used to prospectively assess the views of TCs and PLDs who were undergoing evaluation for compatible LDKT (but had not yet donated or received a transplant) at 3 large Canadian kidney transplant centers—Vancouver General Hospital and St. Paul’s Hospital in Vancouver, BC, and the Centre hospitalier de l’Université de Montréal (CHUM) in Montréal, Quebec—between June 2016 and August 2018. Quantitative surveys and qualitative interviews were conducted sequentially to gain in-depth insight on participants’ attitudes toward participation in KPD. 11 Patients were recruited from these 2 provinces to capture the diversity of opinions from 2 regions with very different rates of living donation, BC having one of the highest rates of living donation in Canada, and Quebec having among the lowest. During the study period, there was no standardized approach or education in any of the centers with respect to the participation of compatible pairs in KPD. The CHUM and UBC Providence Health REBs approved the study and all participants provided informed consent.
Adult TCs and PLDs who were medically approved or were within the final stages of evaluation for transplantation or donation with a compatible PLD or TC were included in the study. TCs and PLDs who were working toward a compatible transplant but were unaware of their compatibility at the time of the interview were also included. Incompatible pairs, nondirected anonymous PLDs, and TCs with out-of-country PLDs were excluded.
Surveys
A published survey of prior living donors and transplant recipients on enrollment in KPD was modified for this study. 12 The final survey consisted of questions in multiple-choice format and short forced-choice questions using 3- and 5-point Likert scales. Separate surveys were developed for PLDs and TCs and were translated in English and French (see Supplementary file for full surveys). The survey questions captured key sociodemographic and disease-related characteristics (for TCs) and addressed the following themes: (1) willingness to participate as a compatible pair in KPD, (2) facilitating factors and barriers to participating as a compatible pair in KPD, and (3) the decision-making process to consider enrollment in KPD as a compatible pair. In addition, a self-reported altruism (SRA) scale 13 was used to account for the level of altruism in survey respondents. Survey questions were pilot-tested with 6 past living kidney donors and 6 transplant recipients (evenly distributed between English- and French-speaking). Both PLDs and TCs were invited to participate in the survey during their pre-assessment medical visits between June 2016 and July 2017, and completed the surveys anonymously thereafter.
Descriptive statistical analyses were performed to characterize each group in terms of age, gender, socioeconomic status, race/ethnicity, blood type, relationship to directed donor/recipient, SRA score, and dialysis status and duration (for TCs). The willingness of TCs and PLDs to participate in KPD as a compatible pair overall and under specific circumstances was described by reporting the proportion of participants who responded to each category of willingness in the Likert scale. Continuous variables were reported as means and standard deviations, whereas categorical variables were reported as proportions. Comparisons between groups were made using a chi-squared test and t test, as appropriate. Statistical analyses were performed using R v3.4.4 (2018-03-15).
Qualitative Interviews
Convenience sampling 14 was used to recruit PLDs and TCs to gain further insight into participants’ views on the participation of compatible pairs in KPD. Participants were invited to take part in semi-directed interviews between May 2017 and August 2018. Twenty-nine TCs and 16 PLDs attending the CHUM and 42 TCs and 24 PLDs attending BC transplant clinics were approached by transplant nurses, transplant coordinators, or a receptionist and received an invitation letter to participate in this project. Among the 66 PLDs and TCs from BC, 18 were no longer eligible by the time they were contacted because they had either received a transplant or donated, 23 could not be reached, and 25 agreed to participate. Among the 45 PLDs and TCs from the CHUM, 18 were ineligible because they had received a transplant, donated or were no longer suitable for kidney transplantation or donation, and 13 could not be reached. Fourteen participants from the CHUM were contacted, of which 4 declined the invitation and 10 agreed to participate. Three interviews were conducted in person and 32 by phone by a member of the research team (F.B.G.). Twenty-six interviews were conducted in English and 9 in French. The interviews lasted roughly 30 minutes (22-45 minutes) and were digitally recorded and transcribed.
The issues covered during the interviews were outlined in an interview guide with open-ended questions that was based on a literature review and the researchers’ previous work in the field.15-19 It addressed the following themes: (1) attitudes toward participation in KPD, (2) factors that could affect their willingness to participate in KPD, and (3) fears and expectations surrounding KPD (see Supplementary file for interview guide). The interview guide was pilot-tested in English and French by 3 transplant recipients and 1 living donor.
Interview transcripts were analyzed using the content and thematic analysis method described by Miles and Huberman. 20 NVivo 11 (QSR International) computer software was used to facilitate the qualitative analysis. Two members of the research team developed the coding frame (M-C.F. and F.B.G.) based on the interview topics. A deductive approach to coding was used, but new codes were also generated based on new themes that emerged during the analysis. However, F.B.G. coded all the interviews. The number of participants allowed for data saturation. 14 No new codes were created after the 31st interview. An independent researcher with experience in qualitative methods and research in the field of organ transplantation (J.A.) coded 17% of the raw data, and the rate of coding agreement was subsequently assessed at 96%. We used the consolidated criteria for reporting qualitative research checklist.14,21
Results
Participant Characteristics
Tables 1 and 2 outline the characteristics of the TCs and PLDs who completed the survey or interviews. A total of 111 TCs and 116 PLDs completed the survey, and 17 TCs and 18 PLDs took part in in-depth interviews.
Survey Respondents’ Characteristics.

Note. TC = transplant candidate; PLD = potential living donor; SRA = self-reported altruism; N/A = not applicable.
In-Depth Interview Participants’ Characteristics.

Note. ESRD = end-stage renal disease; TC = transplant candidate; PLD = potential living donor; N/A = not applicable.
This TC’s PLD is a member of his entourage, but the PLD wanted to remain anonymous.
Willingness to Enroll in KPD
Survey results
Seventy-one of PLDs surveyed (61.2%) and 85 of TCs surveyed (76.6%) reported a willingness to enroll in KPD as a compatible pair (Table 3). Table 3 outlines surveyed TC and PLD characteristics by their willingness to enroll in KPD as a compatible pair. Among TCs who were unwilling to enroll in KPD, there was a higher proportion of individuals who had a spousal potential donor, a university or college education, and a higher income. Dialysis exposure was also lower among TCs who reported an unwillingness to enroll in KPD. Among PLDs who were unwilling to participate in KPD, there was a higher proportion of individuals who were spouses or biological relatives of their intended recipient, but all other characteristics were not significantly different from those of PLDs who were willing to participate in KPD. The SRA score was not significantly different between groups.
Patient Baseline Characteristics Among Survey Respondents, by Willingness to Enroll in KPD as a Compatible Pair.
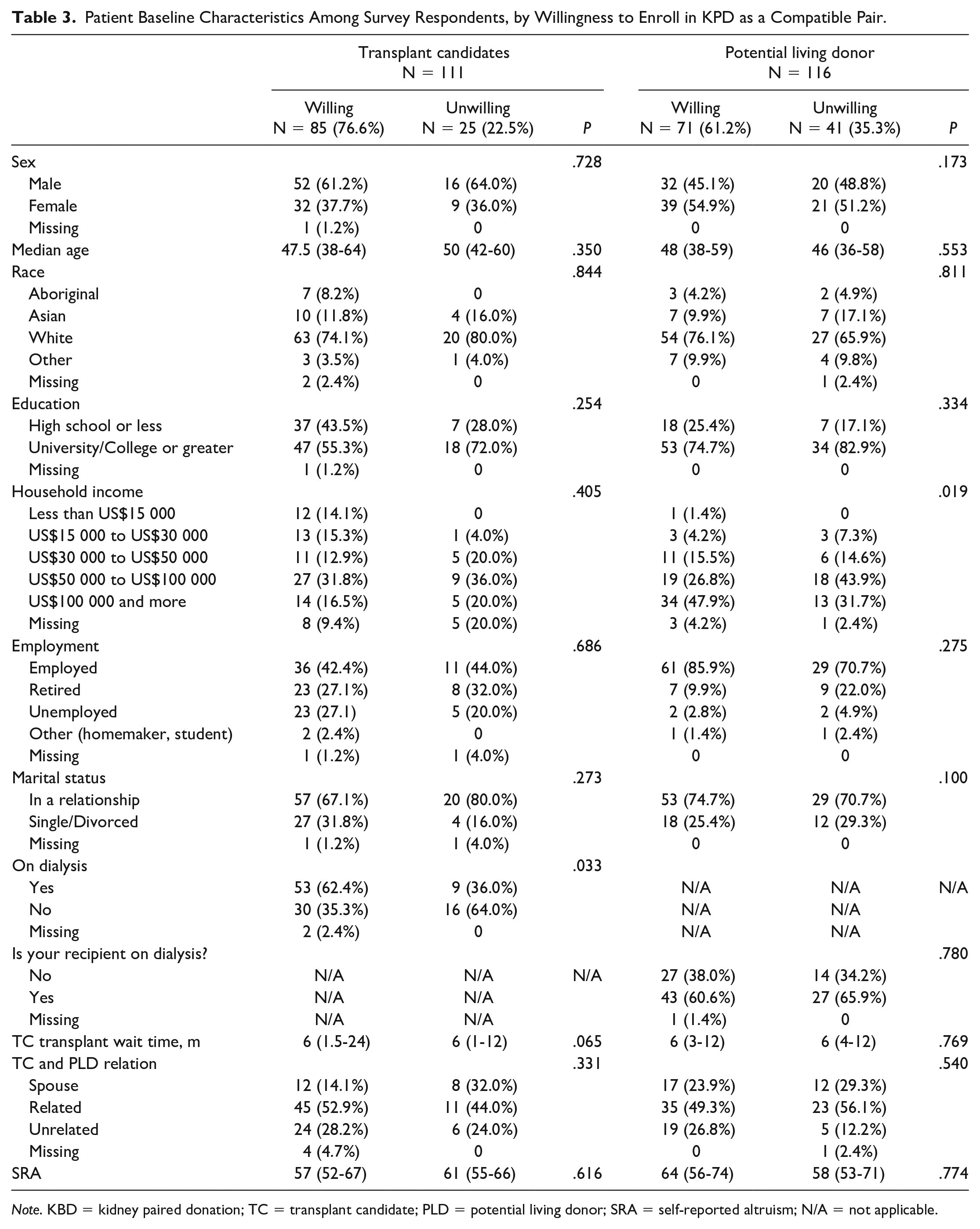
Note. KBD = kidney paired donation; TC = transplant candidate; PLD = potential living donor; SRA = self-reported altruism; N/A = not applicable.
Qualitative interviews
Two PLDs (11.1%) and 8 TCs (47.1%) interviewed were willing to participate as compatible pairs in KPD, citing the following reasons: to increase the number of transplantations performed, to help other people, and because of the possibility of the TC receiving a younger, better-matched and healthier kidney that will last longer. That being said, PLDs and TCs who were willing to participate in KPD as compatible pairs wanted assurance that the TC would receive a kidney transplant.
For most of the TCs and PLDs who were unwilling to participate or ambivalent about participating as compatible pairs in KPD, the main reason cited was the established relationship with the PLD or TC or their not knowing the donor or recipient personally. Some recipients pointed to the emotional nature of living kidney donation and the difficulty of donating an organ to a stranger, whereas others indicated that they want to donate to their intended recipient because they know them and decided to donate to this person and no one else. Transplant candidates also mentioned being more comfortable receiving a kidney from a compatible person they know than from a stranger. Some participants also needed more time to consider this option. Table 4 summarizes the themes and presents interview excerpts.
Reasons Supporting Willingness and Unwillingness to Participate as a Compatible Pairs in KPD.

Note. KBD = kidney paired donation; TC = transplant candidate; PLD = potential living donor.
Factors That Influence Willingness to Enroll in KPD
Survey results
The vast majority of PLDs (87.1%) and TCs (85.4%) felt the decision to enroll in KPD should be shared between the PLD and TC (Tables 5 and 6). When asked which single factor most increased willingness (Figure 1), the largest group of PLDs (67%) reported getting a “better kidney” for their intended recipient, whereas 38% of TCs reported getting a “better kidney” as the most important factor in their decision-making. However, more TCs (39%) reported wanting to help as many other people as possible as the most important factor. Conversely, ending up with a “lesser quality kidney” for the recipient was the most important factor that would deter PLDs and TCs from pursuing compatible KPD, with 56% of PLDs and 48% of TCs reporting this as the most important factor (Figure 2).
Factors Modifying Willingness of PLDs to Participate in KPD as a Compatible Pair.
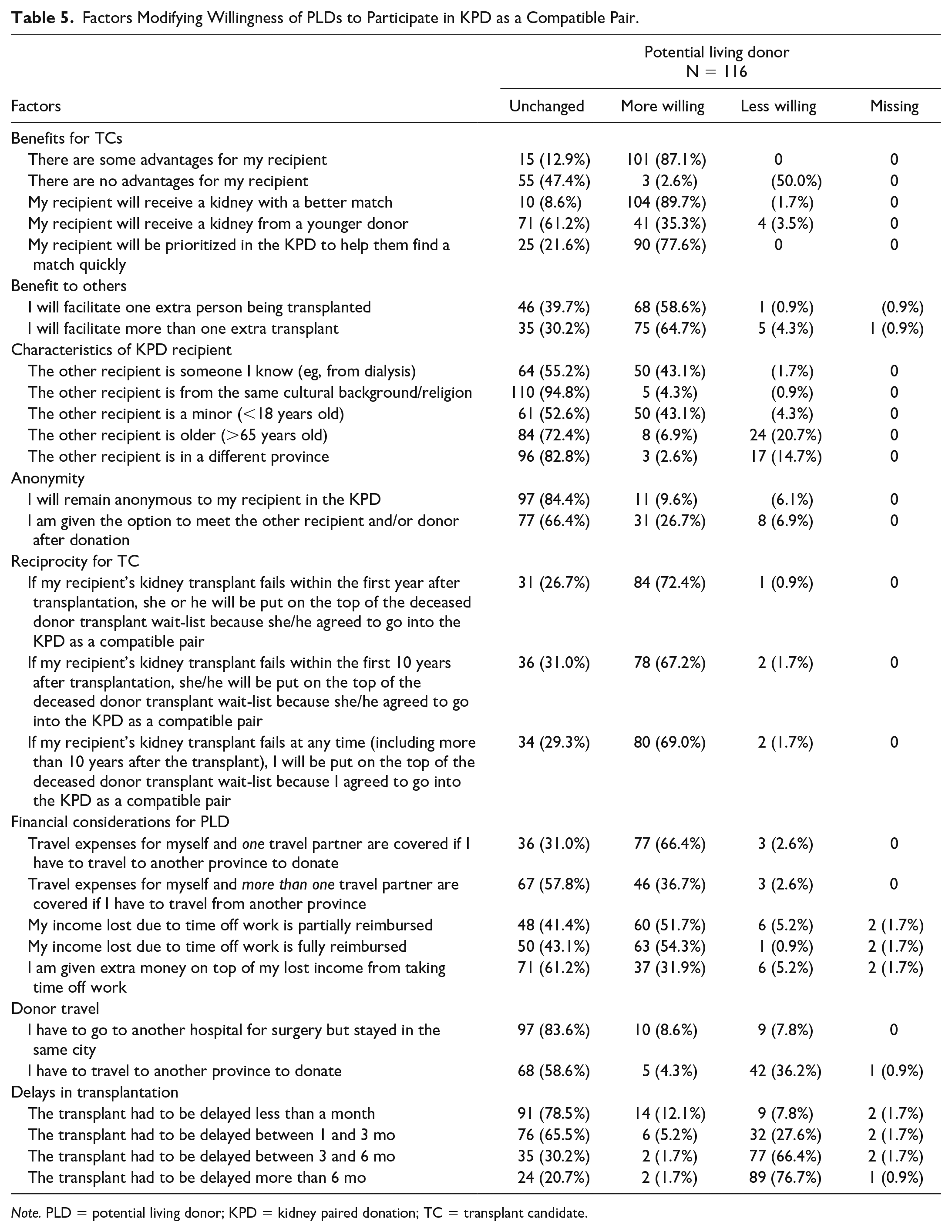
Note. PLD = potential living donor; KPD = kidney paired donation; TC = transplant candidate.
Factors Modifying Willingness of TCs to Participate in KPD as a Compatible Pair.

Note. TC = transplant candidate; KPD = kidney paired donation; PLD = potential living donor.

Most important factor that would influence decision to participate in kidney paired donation as compatible pair.

Most important factor that would hinder decision to participate in kidney paired donation as compatible pair.
Importantly, 47.4% of PLDs and 61.3% of TCs reported no change to their willingness to consider KPD if there was no clear medical benefit for the intended compatible TC. Furthermore, 58.6% of PLDs and 54.1% of TCs reported an increased willingness if they could facilitate one additional transplant for a stranger and an even greater proportion reported an increased willingness if transplantation facilitated more than one extra transplant. Facilitating transplantation for a minor or for someone else they knew also increased willingness to participate in KPD. Similarly, having the option to meet the individual that compatible KPD benefited increased willingness to participate in both PLDs and TCs, although most (84.4%) of PLDs stated their willingness to participate was unchanged even if they were to remain anonymous.
Prioritization of the compatible TC for repeat transplantation in the event that the KPD transplant fails significantly increased the willingness of compatible PLDs and TCs to participate in KPD, with 72.4% of PLDs and 80.2% of TCs reporting an increased willingness to enroll in KPD if there were a policy of reciprocity, whereby if the TC’s transplant from KPD were to fail within the first year, they would be moved to the top of the wait list for a deceased-donor transplant. Interestingly, extending this benefit to a KPD transplant that fails beyond the first year after transplantation did not substantially increase willingness further.
Reimbursement of the donor’s and a companion’s travel expenses increased willingness among 66.4% of PLDs and 76.6% of TCs. Similarly, reimbursing lost wages increased willingness in 51.7% of PLDs and 77.5% of TCs. The promise of overt cash incentives for the PLD increased the willingness among 55.9% of TCs, but only increased willingness among 31.9% of PLDs.
Delays in transplantation reduced willingness among both PLDs and TCs, with a delay of 3 to 6 months reducing willingness among 66.4% of PLDs and 39.6% of TCs, and a delay of 6 months reducing willingness among 76.7% of PLDs and 65.8% of TCs. Twenty-one percent of PLDs and 19% of TCs reported delays in transplantation as the most important factor that would hinder their willingness to enroll in KPD as a compatible pair (Figure 2). Also, the need for donors to travel to another province reduced willingness among 36.2% of PLDs and 28.3% of TCs.
Qualitative interviews
During the interviews, most of the PLDs and TCs felt that the decision to participate in KPD belongs primarily to the PLD, as it is the donor who is making a sacrifice and has the most to lose by participating in KPD. A participant mentioned that the PLD should be given the option of participating in KPD before knowing whether or not they are compatible with their TC. Some TCs also mentioned that PLDs have chosen their intended recipient and that this decision should be respected. Other participants mentioned that the decision to participate as a compatible pair should be made jointly by the PLD and TC. Table 7 summarizes the themes and presents interview excerpts.
Responsibility for Deciding to Participate in KPD as a Compatible Pair.

Note. KPD = kidney paired donation; TC = transplant candidate; PLD = potential living donor.
Offering priority points for future kidney transplants to recipients who choose to participate in KPD with a compatible donor in the event that a graft fails was identified as a facilitating factor. Either priority points for a deceased-donor kidney transplant or for an organ from a donor at the end of the chain in KPD would make participants reconsider their stance on participating in KPD as a compatible pair. Financial incentives such as reimbursing travel expenses for a companion for a donor who has to travel to another transplant center, to have support during organ recovery and offset lost income, were cited as factors that would facilitate participation. The PLDs and TCs also suggested that knowing an incompatible pair registered in KPD would make them more inclined to participate in KPD, indicating that it would be easier to donate or accept a kidney from someone they know and whose lifestyle habits they are familiar with. For one PLD, advanced donation was mentioned as a facilitating factor.
Delaying transplantation as a result of participating in KPD was the major concern expressed by PLDs and TCs. The PLDs are concerned about putting the TC’s health at risk if the transplantation is delayed. The other major concern or obstacle regarding participation in KPD is the risk of chain breaks. Donors having to travel to the recipient center and the costs associated with doing so are further obstacles to participating in KPD. Moreover, participants are reluctant to travel to the TC’s center because they want to stay close to their family for support and do not want to deal with a medical team with which they are unfamiliar and have not yet established trust. Finally, the quality of the kidney obtained through KPD compared with the kidney from a directed donor is also a major concern and could represent an obstacle to participation. Box 1 summarizes facilitating factors and obstacles and presents interview excerpts.
Facilitating Factors and Obstacles to Participation as a Compatible Pair in KPD.

Note. KBD = kidney paired donation; TC = transplant candidate; PLD = potential living donor.
Symbolic Nature of Living Kidney Donation
This topic was only addressed during interviews. Many TCs and PLDs mentioned that there was a difference between directed living kidney donation and donating to a stranger. One PLD who is donating to his or her partner mentioned that there was something special in giving that person something another person could not, whereas another participant mentioned that there is a special connection between donors and their intended recipients, and that the connection is not there if you donate to a stranger. For TCs who participated in this study, it is important to know the lifestyle habits of the PLD who will ultimately donate a kidney, to be sure that the kidney is of good quality. Another difference between directed LDKT and participation as a compatible pair in KPD is that, in KPD, the PLDs know the TCs and can be sure that the medical condition is not self-inflicted.
Some participants, mostly TCs and some PLDs, indicated that it would make no difference if they received a kidney from a stranger rather than their intended donor. One PLD claimed that if the TC receives a kidney, it does not matter to whom the donor donates, whereas another PLD said that what matters is that the TC receives the best kidney, no matter who it comes from. Box 2 summarizes the theme and presents interview excerpts.
Symbolic Nature of Living Kidney Donation.

Note. TC = transplant candidate; PLD = potential living donor; ESRD = end-stage renal disease.
Discussion
Participation of compatible donor and recipient pairs in KPD continues to be rare, with compatible pairs comprising only 2.3% of transplants performed in the National Kidney Registry in the United States. 8 In Canada, since the inception of KPD, only 36 compatible pairs have registered in KPD programs out of a total of 1484 pairs, representing 2.4% of all pairs (Canadian Blood Services, personal communication). In this study, we prospectively examined PLDs’ and TCs’ perspectives on participation in KPD as a compatible pair, with a cohort of individuals who are actively being evaluated for living kidney donation or transplantation. When surveyed, 61.2% of PLDs and 76.6% of TCs reported a willingness to enroll in KPD as a compatible pair, which is consistent with prior Canadian retrospective survey studies on this issue, 12 but contradicts studies conducted in the United States and the Netherlands that reported a higher degree of ambivalence or lack of interest in participating in KPD among compatible pairs.6,22 Interestingly, only 11.1% of PLDs and 47.1% of TCs who consented to the in-depth interviews were willing to enroll in KPD. The decreased willingness to participate in KPD reported by individuals who took part in interviews may be attributed to the inherent difference in methodology. The smaller cohort of individuals who consented to interviews may represent a selected subset of individuals who were more concerned about KPD, but it is also possible that TCs and PLDs may have felt more comfortable voicing their concerns in an interview.
Another important consideration is that individuals who completed the surveys were at an earlier phase in their donation and transplantation evaluation process compared with those who completed the interviews. Surveys were all completed among individuals for whom a final decision regarding candidacy had not yet been made, whereas the in-depth interviews were conducted among individuals who were at a later point in their evaluation process where their candidacy had often been finalized and plans were being made in the context of a direct compatible transplant. These results may indicate that compatible pairs of PLDs and TCs may be more inclined to consider KPD at an earlier stage in their evaluation rather than at a later point where plans for directed donation are more firmly established. Therefore, the timing of discussions about KPD for compatible pairs may be a key factor, suggesting that earlier introduction of this option may be preferable, to make TCs and PLDs more comfortable considering this as a viable option and allow them sufficient time to do so.
An important finding in this study is that the prospect of facilitating transplantation among additional patients in and of itself appears to be a strong motivator for TCs to consider KPD, and, in both surveys and interviews, was cited as the most important factor driving their desire to participate as a compatible pair. As in prior studies,6,8,22,23 finding a “better match” or medical advantage for the intended TC was also cited by both PLDs and TCs as an important motivator for participating in KPD and has the potential to further increase willingness to participate as a compatible pair.
The PLDs who participated in our study also wanted to ensure that no harm comes to their intended TCs through the decision to pursue KPD as a compatible pair. In particular, avoiding delays in transplantation that may result in prolonged dialysis exposure and associated harm for the TC was viewed as a key condition for considering participation in KPD. In the Canadian KPD program, there are only 3 match cycles per year to maximize matches, resulting in a median wait time of 182 days from the time of enrollment to transplantation. 1 Consequently, the anticipated delays in large KPD programs like this may limit the opportunities for compatible KPD. Conversely, KPD programs with an increased frequency of match runs are likely to be more suitable for enrollment of compatible pairs in KPD.
Both PLDs and TCs were highly supportive of policies that would ensure rapid access to repeat transplantation for TCs that enroll in KPD with a compatible donor. More than 72% of PLDs and 80.2% of TCs reported an increased willingness to participate in KPD as a compatible pair if there were a guarantee of prioritization for repeat transplantation through either a deceased donor or a nondirected living donor (through KPD) if the transplant recipient suffered allograft loss within the first year following transplantation. Importantly, providing a similar guarantee for recipients’ whose graft failed after the first year post-transplant did not further increase willingness to participate in KPD. Therefore, a policy of reciprocity whereby TCs who enroll in KPD as part of a compatible pair would be prioritized for repeat transplantation in the event of early graft loss may provide additional assurance for compatible pairs considering KPD and significantly increase the likelihood of enrollment in the program. While such a policy would need to consider the views of all patients waiting for a deceased-donor kidney, the impact of such a policy on wait times has been examined and is likely to be minimal due to the low likelihood of early graft loss following LDKT.16,24
The anonymity of KPD is a major barrier for some compatible pairs to overcome, as it minimizes the perceived connection between donors and recipients. The PLDs interviewed who were unwilling to enroll in KPD felt a sense of “loyalty” and an emotional bond in donating directly to their intended recipient. This sentiment was also noted among PLDs who completed the survey, who reported that they would be more willing to participate in KPD if their kidney were allocated to a minor or someone they knew. Similar findings were reported by Kranenburg et al, 22 who reported that, in the Netherlands, the emotional relationship between compatible donors and recipients was the most frequently cited reason for not wanting to participate in KPD as a compatible pair. Anonymity of donor/recipient pairs is a key component of many KPD programs, including the Canadian KPD program. Examining strategies whereby an emotional link may be established between compatible KPD donors and their recipient while maintaining anonymity may increase willingness of compatible pairs to enroll in KPD programs.
While our work represents the only large-scale prospective mixed-methods study examining the enrollment of compatible pairs in KPD, there are important limitations to consider. The study was conducted in 3 transplant programs in 2 Canadian provinces and therefore may only represent the views of PLDs and TCs in these programs and regions. Although the surveys were anonymous, social desirability bias may still be an important limitation, particularly during the in-depth in-person interviews. The surveys and interviews were conducted in English and French and excluded individuals with other primary languages. Moreover, participants in the survey were primarily white and highly educated. Also, the interviews and surveys revealed that most donors were either the spouse or a family member of the recipient. As a consequence, these data may not be reflective of the views of individuals in other groups, including ethnic minority populations.
Conclusion
The participation of compatible pairs in KPD has the potential to improve access to kidney transplantation for incompatible recipients and further optimize outcomes for compatible TCs. A high proportion of PLDs and TCs in our study were willing to consider KPD as part of a compatible pair, even in the absence of a direct benefit to the recipient. Approaching PLDs and TCs early in their evaluation process, ensuring timely transplantation and a more optimally matched kidney for TCs, and offering a policy of reciprocity to ensure timely repeat transplantation for compatible recipients should their allograft fail post KPD transplant may further increase participation of compatible pairs in KPD.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581211058932 – Supplemental material for Compatible Donor and Recipient Pairs’ Perspectives on Participation in Kidney Paired Donation Programs: A Mixed-Methods Study
Supplemental material, sj-docx-1-cjk-10.1177_20543581211058932 for Compatible Donor and Recipient Pairs’ Perspectives on Participation in Kidney Paired Donation Programs: A Mixed-Methods Study by Marie-Chantal Fortin, John Gill, Julie Allard, Fabián Ballesteros Gallego and Jagbir Gill in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-docx-2-cjk-10.1177_20543581211058932 – Supplemental material for Compatible Donor and Recipient Pairs’ Perspectives on Participation in Kidney Paired Donation Programs: A Mixed-Methods Study
Supplemental material, sj-docx-2-cjk-10.1177_20543581211058932 for Compatible Donor and Recipient Pairs’ Perspectives on Participation in Kidney Paired Donation Programs: A Mixed-Methods Study by Marie-Chantal Fortin, John Gill, Julie Allard, Fabián Ballesteros Gallego and Jagbir Gill in Canadian Journal of Kidney Health and Disease
Footnotes
List of Abbreviations
BC, British Columbia; ESRD, end-stage renal disease; HLA, human leukocyte antigen; KPD, kidney paired donation; LDKT, living-donor kidney transplantation; PLD, potential living donor; TC, transplant candidate.
Authorship
1. Marie-Chantal Fortin participated in research design, in the performance of the research, in data analysis, and in the writing of the manuscript.
2. John Gill participated in research design and the writing of the manuscript.
3. Julie Allard participated in data analysis and the writing of the manuscript.
4. Fabián Ballesteros participated in the performance of the research, in data analysis, and in the writing of the manuscript.
5. Jagbir Gill participated in research design, in the performance of the research and in the writing of the manuscript.
Ethics Approval and Consent to Participate
The Centre hospitalier de l’Université de Montréal (ethics certificate 15.206) and UBC Providence Health (ethics certificate H15- 03361) research ethics board approved the study. All participants provided informed consent.
Consent for Publication
All authors consent to publication.
Availability of Data and Materials
The data are available from corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was funded by a Biomedical Research Grant from the Kidney Foundation of Canada.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.