
Abstract
Background:
In North America, most people start hemodialysis via a central venous catheter (“catheter”). These patients are counseled to undergo arteriovenous fistula (“fistula”) creation within weeks of starting hemodialysis because fistulas are associated with improved survival.
Objectives:
To determine whether attempting to create a fistula in patients who start hemodialysis via a catheter is associated with improved mortality. We also sought to determine whether differences in baseline patient characteristics, vascular procedures for access-related complications, or days in hospital may confound or mediate the relationship between attempted fistula creation and mortality.
Design:
Multicenter, retrospective cohort study.
Setting:
Six dialysis programs located in Ontario, Alberta, and Manitoba.
Patients:
Patients aged ≥18 years who initiated hemodialysis via a catheter between January 1, 2004, and May 31, 2012, who had not had a previous attempt at fistula creation. We excluded those who had a life expectancy less than 1 year, who transitioned to peritoneal dialysis within 6 months of starting dialysis, and people who started hemodialysis via a graft.
Measurements:
Attempted fistula creation, all-cause mortality, patient characteristics and comorbidities, vascular procedures for access-related complications, and days spent in hospital.
Methods:
We used survival methods, including marginal structural models, to account for immortal time bias and time-varying confounding.
Results:
In total, 1832 patients initiated hemodialysis via a catheter during the study period and met inclusion criteria. Of these patients, 565 (31%) underwent an attempt at fistula creation following hemodialysis start. As compared to those who did not receive a fistula attempt, these people were younger, had fewer comorbidities, and were more likely to have started dialysis as an outpatient and to have received pre-dialysis care. In a marginal structural model controlling for baseline characteristics and comorbidities, attempted fistula creation was associated with a significantly lower mortality (hazard ratio [HR] = 0.53; 95% confidence interval [CI] = 0.43-0.66). This effect did not appear to be confounded or mediated by differences in the number of days spent in hospital or vascular procedures for access-related complications. It also remained similar in analyses restricted to patients who survived at least 6 months (HR = 0.60; 95% CI = 0.47-0.77) and to patients who started hemodialysis as an outpatient (HR = 0.48; 95% CI = 0.33-0.68).
Limitations:
There is likely residual confounding and treatment selection bias.
Conclusions:
In this multicenter cohort study, attempting fistula creation in people who started hemodialysis via a catheter was associated with significantly reduced mortality. This reduction in mortality could not be explained by differences in patient characteristics or comorbidities, days spent in hospital, or vascular procedures for access-related complications. Residual confounding or selection bias may explain the observed benefits of fistulas for hemodialysis access.
Trial Registration:
Not applicable (cohort study).
Introduction
The majority (~70%) of people with end-stage kidney failure (~300 000 000 globally) are treated with hemodialysis,1,2 a treatment which requires reliable vascular access. This may be accomplished using a central venous catheter (“catheter”), an arteriovenous fistula (“fistula”), or an arteriovenous graft (“graft”). In North America, approximately 80% of people start hemodialysis via a catheter; these patients are counseled to consider an attempt at fistula creation within weeks of starting hemodialysis.3-6 Although guidelines are moving toward more patient-centered approaches, clinical practice guidelines, national initiatives, and patient advocacy groups still recommend use of fistulas and discourage catheters for long-term hemodialysis access.3-7 These recommendations are largely based on observational data associating receipt of hemodialysis via a usable fistula with a lower risk of mortality, with access-related morbidity being considered a mediator of increased mortality among catheter users. 8
However, no randomized controlled trial has compared the effects of different hemodialysis access strategies on patient outcomes and existing observational evidence is at high risk of bias. 8 Studies that assessed the impact of creating a fistula for hemodialysis access compared outcomes of people who achieved a usable fistula to those that used a catheter, including those who were not eligible for a fistula or whose fistula had previously failed.8,9 As a consequence, existing studies have not assessed the impact of attempting to create a fistula (the intervention being prescribed), but rather that of achieving a functional fistula (an outcome that cannot be prescribed).10-12 This is important because 23% to 60% of fistula creation attempts fail.13,14 They have also not controlled for the confounding or mediating effects of variables that change over time such as days spent in hospital and procedures used to maintain access patency or address access-related complications. 15 Existing studies have proposed that access-related morbidity mediates the increased risk of death among catheter users, 16 but evidence in support of these claims is lacking. Instead, studies have shown that the vast majority of catheter-related deaths are not due to access complications,16,17 suggesting that the increased need for access-related procedures or days spent in hospital occur more often among catheter users who are “sicker” than fistula users.9,16,17
We performed a multicenter, Canadian, retrospective cohort study to determine whether attempting to create a fistula in patients who start hemodialysis via a catheter is associated with improved mortality. We also sought to determine whether differences in baseline patient characteristics, vascular procedures for access-related complications, or days spent in hospital may confound or mediate the relationship between attempted fistula creation and mortality. We tested the hypothesis that patient characteristics, days spent in hospital, or vascular access–related procedures may explain or mediate the association between attempted fistula creation and mortality in patients who started hemodialysis via a catheter.
Methods
Design and Reporting
We conducted a multicenter, retrospective cohort study. Reporting followed recommended guidelines.18,19
Ethical Considerations
Research ethics approval and waiver of patient consent were obtained from each of the 5 participating Canadian dialysis programs.
Data Sources and Participants
We identified patients aged 18 years old or older who initiated hemodialysis via a catheter between January 1, 2004, and May 31, 2012, and who had not received a previous attempt at fistula creation (including radiocephalic, brachiocephalic, and other inflow-outflow configurations). We excluded those who had a life expectancy less than 1 year due to metastatic cancer or other terminal illnesses, who transitioned to peritoneal dialysis within 6 months of starting dialysis, and people who started hemodialysis via a graft.
Setting and Data
We collected data from the Dialysis Measurement Analysis and Reporting (DMAR) system. The DMAR system was a centrally hosted, web-based quality improvement system that prospectively collected data on incident hemodialysis patients treated at 1 of 6 participating Canadian dialysis programs located in Ontario (The Ottawa Hospital, Sunnybrook Health Sciences Center, and London Health Sciences Center), Alberta (Northern and Southern Alberta Renal Programs), and Manitoba (Manitoba Renal Program). Patients were included in DMAR if they had chronic kidney failure and started dialysis or had acute kidney injury and received at least 28 days of dialysis.
Trained staff entered data into DMAR using a standardized coding schema. These data were then centrally reviewed for coding consistency, accuracy, and completeness. Data contained in DMAR included baseline demographic, comorbidity, and laboratory information; any changes in dialysis modality; hospitalizations; kidney transplantations; losses to follow-up; transfers out of the program; and deaths. All vascular access procedures, before and after initiation of dialysis therapy, were also captured, along with the location, date, description, and indication for each procedure.
Exposure Variable
The exposure of interest was attempted fistula creation after starting hemodialysis with a catheter, determined longitudinally by DMAR procedure records. Using an intention-to-treat analysis, patients were unexposed if they did not receive a fistula attempt for any time before they received one. Following receipt of a fistula creation attempt, they remained exposed regardless of whether or not the fistula became suitable for use.
Outcome
The primary outcome was all-cause mortality during the study follow-up period.
Follow-up
We followed participants from hemodialysis initiation until recovery of kidney function, kidney transplant, transfer out of the dialysis program, transfer to peritoneal dialysis (after 6 months), the end of the follow-up period, or death.
Covariates
We controlled for a number of covariates that a published international survey of nephrologists 20 and multidisciplinary hemodialysis access teams 21 identified as potential confounders of the relationship between attempted fistula creation and mortality. These covariates included age, gender, duration of pre-dialysis care, and history of diabetes or cardiovascular disease (CVD) (defined as coronary, cerebrovascular, or peripheral artery disease or heart failure).
Study Size
Based on previous studies, 16 we estimated that approximately 1500 patients would start hemodialysis using a catheter at the 5 participating dialysis centers. Assuming that approximately 30% of people would receive a fistula attempt and about 30% of all people (with/without attempt) would die during the study period, we estimated that this sample size would have a power of at least 85% to detect a significant difference in mortality with a hazard ratio (HR) of ≤0.7 (or ≥1.4) and a 2-sided P-value of .01.
Statistical Analyses
We summarized categorical and continuous patient characteristics using counts (percentages) and medians (with interquartile ranges [IQRs]), stratified by whether patients underwent an attempt at fistula creation. We compared these statistics using chi-square and Mann-Whitney U tests, respectively.
As standard methods for analyzing cohort studies with time-updated exposure and covariate variables can produce biased estimates, 22 we used a marginal structural model to determine the effect of attempted fistula creation on the hazard of death after starting hemodialysis via a catheter. Marginal structural models account for immortal time bias and control for confounding variables that change over time. Immortal time is the time during which death cannot occur among the exposed. Bias is the result of selecting participants who survive until they become exposed (survivorship bias), which extends their survival time by a period preceding the exposure (immortal time). A common way to address this bias is to treat the exposed as “unexposed” until the date they become exposed and are then “exposed” thereafter. To control time-varying confounding, marginal structural models use patient weights based on their probability of receiving treatment (ie, attempted fistula creation) and of being censored. 15 We determined stabilized inverse probability of treatment weights using age, sex, history of CVD, diabetes, pre-dialysis care, and inpatient initiation of hemodialysis as baseline covariates. We also accounted for the possible time-varying confounding effect of time-varying covariates including days spent in hospital following hemodialysis start and procedures required to maintain access patency or address other access complications, using the same approach. 22
Statistical analyses were conducted using STATA 15 (STATA Corp., College Station, TX, USA). We did not use methods for missing data as information was complete for all of the variables included in the database.
Mediation, Sensitivity, and Post Hoc Analyses
We conducted a series of pre-specified mediation and sensitivity analyses. To assess whether days spent in hospital or vascular procedures for access-related complications were on the causal pathway between a fistula creation attempt and mortality, we compared the mortality estimates obtained from a time-varying Cox models with or without these potential mediators included in the model (time-varying covariates). We also compared the mortality estimate obtained from the above marginal structural model with that estimated using a time-varying Cox proportional hazards model that treats attempted fistula creation as a time-varying exposure (accounting for immortal time bias), but does not address time-varying confounding. This standard Cox model included the same baseline covariates as the marginal structural model (age, sex, history of CVD, diabetes, pre-dialysis care, and inpatient initiation of hemodialysis). We also used a marginal structural model to determine the effect of attempted fistula creation on the risk of death using only those patients with 6 months or longer follow-up to determine whether this association was robust to varying durations of follow-up.
In a post hoc analysis, we excluded patients who had an inpatient dialysis start from the marginal structural model to determine the effect of attempted fistula creation on the hazard of death after starting hemodialysis as an outpatient via a catheter. This model included the same baseline and time-varying covariates as our principal marginal structural model.
Results
Cohort and Follow-Up
We identified 3145 patients who initiated dialysis therapy at 1 of the 5 participating Canadian centers. Of these patients, 1928 (61%) initiated hemodialysis via a catheter and 1832 (95%) of these patients did not have a previous attempt at fistula creation (Figure 1). During a median follow-up of 11 (IQR = 4-25) months, 520 (28%) patients died, 74 (4%) received a kidney transplant, 234 (13%) recovered kidney function, 141 (8%) transferred to another dialysis program, 2 (0.1%) were lost to follow-up, and 66 (4%) transferred to peritoneal dialysis.

Details of cohort creation.
Attempted Fistula Creation in Those That Initiated Hemodialysis via a Catheter
Of these 1832 included patients who did not have a previous attempt at fistula creation, 565 (31%) had an attempt after starting hemodialysis. Table 1 shows baseline characteristics of the patients, stratified by whether or not they had an attempted fistula creation. Patients who had an attempted fistula creation were younger, had fewer comorbidities and a lower estimated glomerular filtration rate (eGFR) at initiation of dialysis, and were more likely to have started dialysis as an outpatient and to have received pre-dialysis care. Patients who had an attempted fistula creation were also significantly less likely to recover kidney function (Table 2). The median length of follow-up was 24.7 (IQR = 13.1-43.7) months in those who underwent an attempted fistula creation and 6.3 (IQR = 2.4-15.7) months in those who did not (P < .001). The median time from dialysis start to fistula attempt was 3.3 (IQR = 1.8-6.2) months while the median follow-up time without a fistula for the whole cohort was 4.9 (IQR = 2.1-11.6) months.
Characteristics of the 1832 Patients Included in the Study.

Note. IQR = interquartile range; BMI = body mass index; eGFR = estimated glomerular filtration rate.
Participant Follow-up and Outcomes.
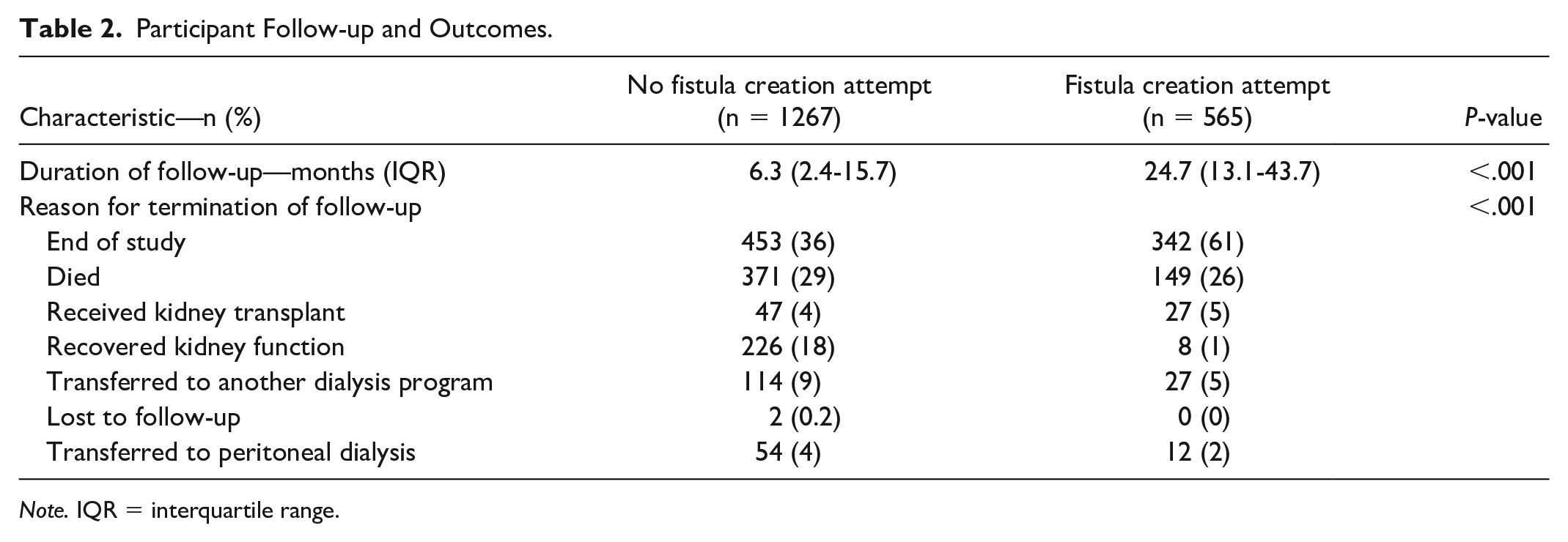
Note. IQR = interquartile range.
Association Between Attempted Fistula Creation and Mortality
In a marginal structural model controlling for baseline and time-varying covariates, attempted fistula creation was associated with a significantly lower hazard of mortality (HR = 0.53; 95% confidence interval [CI] = 0.43-0.66) (Figure 2). Figure 3 provides a comparison of the estimated association between attempted fistula creation and mortality in people starting hemodialysis via a catheter using different modeling strategies. We observed similar results using marginal structural models without time-varying confounding (ie, without treatment and censoring weights) (HR = 0.51; 95% CI = 0.40-0.63). A similar relationship was also observed between attempted fistula creation and reduced mortality using a time-varying Cox proportional hazards model (HR = 0.55; 95% CI = 0.44-0.69), which adjusted for the same covariates, but treated the time-varying covariates (procedures and days in hospital) as mediators (on the causal pathway toward death) rather than confounders (that influence the probability of treatment/censoring) (see Supplemental Table 1 for the full models obtained using each different modeling strategy).

Hazard of death after attempted arteriovenous fistula creation estimated using a marginal structural model.
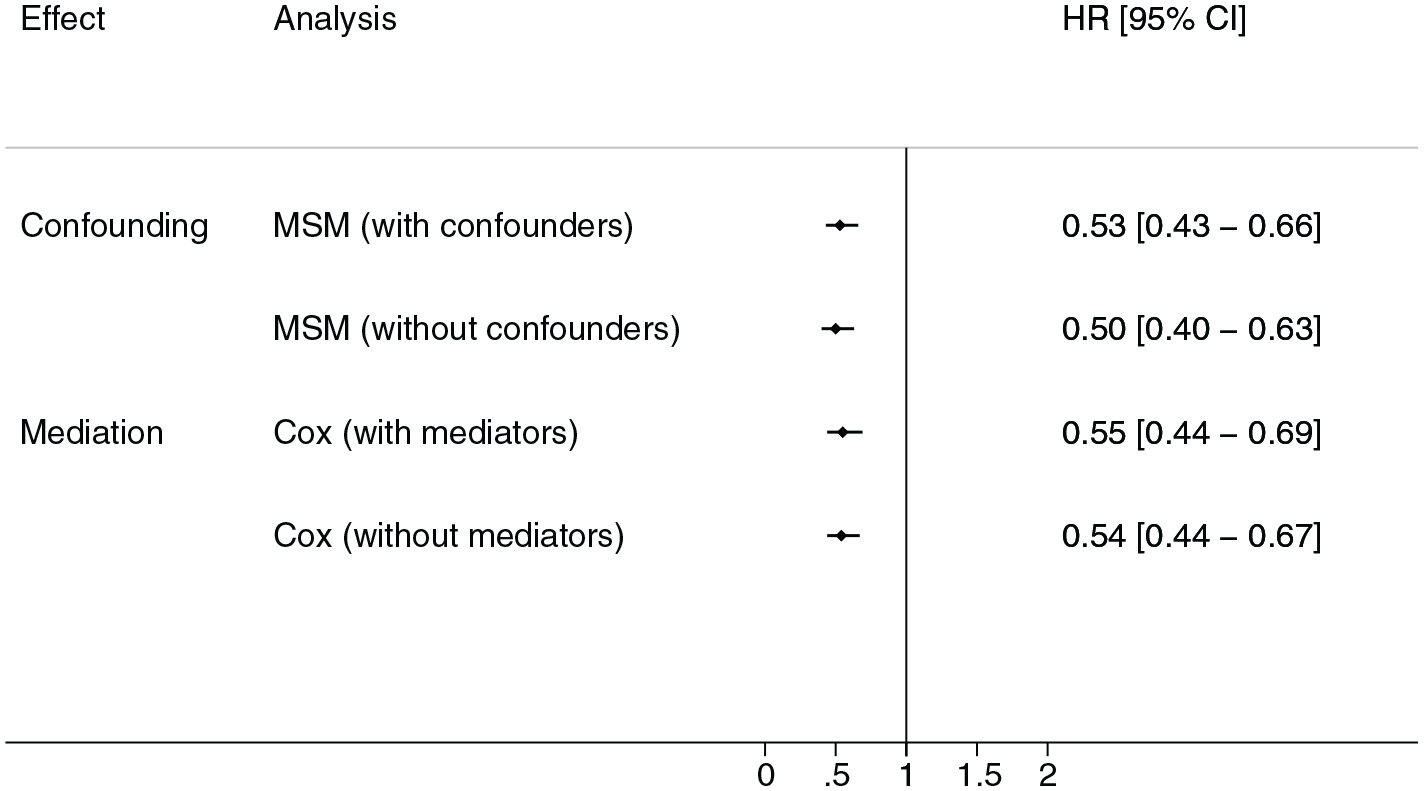
Hazard of death after attempted arteriovenous fistula creation estimated using marginal structural or Cox proportional hazards models.
Mediation, Sensitivity, and Post Hoc Analyses
Using a Cox proportional hazards model, we found no evidence that differences in procedures required to address access complications or days spent in hospital mediated the relationship between attempted fistula creation and mortality. Introducing or removing these variables from the models showed a 2% mediation effect of procedures and 4% mediation effect of days spent in hospital. Overall, removing both these variables from the model altered the HR by less than 0.02. Furthermore, our finding of a reduced mortality with attempted fistula creation was materially unchanged in analyses restricted to patients who survived at least 6 months (HR = 0.60; 95% CI = 0.47-0.77) and to patients who started hemodialysis as an outpatient (HR = 0.48; 95% CI = 0.33-0.68).
Discussion
In this multicenter, Canadian, retrospective cohort study, we found that attempting fistula creation in patients who started hemodialysis via a catheter was associated with a significantly lower mortality. These findings extend those of previous studies from our group by formally testing whether the superiority of fistulas is the result of measured confounding or is mediated by access-related morbidity. We found no evidence of confounding due to differences in baseline characteristics or comorbidities, days spent in hospital or vascular procedures for access-related complications, or mediation effects due to the occurrence of these events over time following a fistula attempt. These findings are consistent with those from a related cohort study, which found no evidence to support that catheter-related deaths were directly related to access complications.16,17 Our finding of reduced mortality in people who underwent an attempted fistula creation remained robust to analyses restricted to 6-month survivors and those who started hemodialysis as an outpatient. Collectively, unless we assume that receiving an attempt at fistula creation somehow alters patient physiology and impacts outcome, much of the excess mortality observed in patients treated with catheters may be due to residual (unmeasured) confounding or treatment selection bias.16,17 Access-related morbidity may be the result of patient health status rather than the type of access used for hemodialysis. This finding has important implications for patient care, developing future clinical practice guideline and policy recommendations, and designing future research.
Designing an observational study that provides a valid comparison between the outcomes of patients who receive hemodialysis via a fistula or catheter is challenging.9,16 First, people receiving hemodialysis via fistulas differ systematically in many important ways from those receiving it via catheters. 9 For example, in this study, patients who had an attempted fistula creation were younger, had fewer comorbidities, less often started dialysis as an inpatient, and more often received pre-dialysis care. People who do and do not receive an attempt at fistula creation may also differ with respect to unmeasured indicators of health that even nephrologists 20 and multidisciplinary hemodialysis access teams 21 have yet to identify as potential confounders. This includes indicators of disease severity (as opposed to comorbid condition present or absent), health status, or functional independence. Second, studies comparing fistulas to catheters have typically included those who were ineligible for a fistula and compared outcomes of people who achieved a usable fistula to everyone who used a catheter, including those in whom a fistula was not possible or failed. 9 To address this problem in this study, we excluded people commonly felt to be ineligible for a fistula (ie, those with a life expectancy less than 1 year, who transitioned to peritoneal dialysis within 6 months of starting dialysis, and who started hemodialysis with a graft). We also compared the effects of attempting to create a fistula instead of achieving a usable fistula, which is what matters to patients and clinicians when making intervention decisions.
We found that just attempting to create a fistula in people who initiated hemodialysis via a catheter was associated with a similarly improved mortality to that previously reported in cohort studies comparing outcomes between those with a usable fistula and a catheter. 8 A related study from our group also reported that hemodialysis patients who undergo a pre-dialysis attempt at creating a fistula had a lower risk of death. 16 Furthermore, while higher rates of access-related complications in those receiving hemodialysis via catheters instead of fistulas (eg, infections) are considered the causal link between access type and mortality,3-6 we previously reported that access-related complications were a relatively rare cause of death among patients receiving hemodialysis, regardless of the type of vascular access. 16 Almost all of the causes of death were more common in the group that did not undergo an attempt at fistula creation, even those that would not be expected to increase because of an exposure to a catheter. 16 This may suggest that the excess mortality observed in patients who receive hemodialysis via a catheter is not due to the catheter, but rather because their demographics and baseline health are different from those who undergo an attempted fistula creation. 16 In this study, lack of confounding effects of indicators of access-related morbidity further supports this interpretation.
Our study is novel. Contrary to current beliefs, we found no evidence to support that access-related morbidity may mediate the relationship between attempted fistula creation (the intervention) and death (the outcome). This is because the apparent benefits of fistula creation remain the same with or without considering the contribution of these explanatory variables. If access-related morbidity mediated the effects of fistulas on mortality, we would have seen the benefits of fistula creation disappear (partly or completely) after accounting for these potential mediators. These findings suggest that treatment selection bias cannot be overcome in observational research comparing the outcomes of people who receive hemodialysis via different vascular access types. Healthier patients are more likely to receive a fistula for hemodialysis and sicker patients a catheter. Residual confounding may persist after adjustment of measured confounding (including time-varying confounding), making the observed outcomes more likely to be the result of the characteristics or health of the included patients than their vascular access type. 9 Because catheters are used predominantly in patients who need to start dialysis urgently (eg, because of an acute illness), those with limited life expectancy or who would not tolerate a fistula, and in those with poor vessels, the risk of confounding by indication and treatment selection bias in nonrandomized studies remains high.9,16,17
This study’s findings should be considered in the context of its strengths and limitations. Although our study addressed many of the limitations of previous cohort studies, we lacked data on cause of death. There is also likely residual confounding and treatment selection bias given that those who underwent an attempted fistula creation were healthier than those who continued to receive hemodialysis via a catheter. Furthermore, less patients in the fistula attempt compared to the no fistula attempt group (1% vs 18%) recovered kidney function, suggesting possible unbalanced distribution of reversible acute kidney injury between groups. The relatively low probability of receiving a fistula for permanent access (31%) supports this interpretation. Finally, data were collected between 2004 and 2012. Although the association between receipt of a fistula and mortality may have not changed over the last decade, the probability of receiving a fistula may have increased in more recent years. Ultimately, a randomized controlled trial is needed to estimate the efficacy and safety of attempting to create a fistula in people who initiate hemodialysis via a catheter. Until recently, however, it was unclear whether clinicians would be willing to participate in such a trial. 20 In a survey of physicians and trainees involved in the care of patients with end-stage renal disease, 76% of respondents from Canada, Europe, and Australasia reported that they would be willing to participate in a trial comparing fistulas and catheters, suggesting that equipoise exists regarding the optimal vascular access strategy. 20 We therefore recently initiated an open-label, pilot randomized controlled trial to test the feasibility and safety of randomizing people 55 years old or older who start hemodialysis with a catheter, and are eligible to receive a fistula, to a catheter- or a fistula-based strategy (ClinicalTrials.gov identifier: NCT02675569). 23
This study has important implications for patient care, developing future clinical practice guideline and policy recommendations, and designing future research. Guidelines, national initiatives, and patient advocacy groups have until recently uniformly recommended fistulas as the best form of hemodialysis access.3-7 Many jurisdictions dedicate significant resources to promoting use of fistulas for hemodialysis access. The proportion of people using a fistula has also traditionally been considered a proxy for the quality of care in hemodialysis access programs. As this study and others suggest that the evidence to support these recommendations and initiatives is at high risk of bias, there is an immediate need for appropriately designed randomized controlled trials to confirm that these efforts to promote fistulas are appropriate and cost-effective. Qualitative studies are also needed to evaluate how vascular access type recommendations can be more responsive to patient and clinician preferences and needs. Until results of these studies are available, they may also imply that choices regarding vascular access type for people who are candidates for a fistula or catheter can be individualized and based on their different benefits and limitations. This is supported by the National Kidney Foundation Kidney Disease Outcomes Quality Initiative (NKF-KDOQI) 2019 guideline update, which has shifted from fistula first to “life plans,” which focus on patient-centered, shared decision-making when deciding about the best vascular access strategy for individual patients. 24
Conclusions
In this multicenter, Canadian, retrospective cohort study, people who started hemodialysis via a catheter and underwent an attempt at fistula creation after starting hemodialysis had a significantly reduced mortality. The reduced mortality in these people could not be explained by differences in baseline characteristics, days spent in hospital, or vascular access–related procedures. Therefore, much of the excess mortality observed in patients treated with catheters may be due to residual confounding or treatment selection bias. This finding has important implications for patient care, developing future clinical practice guideline and policy recommendations, and designing future research.
Supplemental Material
sj-pdf-1-cjk-10.1177_20543581211032846 – Supplemental material for Association Between Attempted Arteriovenous Fistula Creation and Mortality in People Starting Hemodialysis via a Catheter: A Multicenter, Retrospective Cohort Study
Supplemental material, sj-pdf-1-cjk-10.1177_20543581211032846 for Association Between Attempted Arteriovenous Fistula Creation and Mortality in People Starting Hemodialysis via a Catheter: A Multicenter, Retrospective Cohort Study by Derek J. Roberts, Alix Clarke, Meghan Elliott, Kathryn King-Shier, Swapnil Hiremath, Matthew Oliver, Robert R. Quinn and Pietro Ravani in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-pdf-2-cjk-10.1177_20543581211032846 – Supplemental material for Association Between Attempted Arteriovenous Fistula Creation and Mortality in People Starting Hemodialysis via a Catheter: A Multicenter, Retrospective Cohort Study
Supplemental material, sj-pdf-2-cjk-10.1177_20543581211032846 for Association Between Attempted Arteriovenous Fistula Creation and Mortality in People Starting Hemodialysis via a Catheter: A Multicenter, Retrospective Cohort Study by Derek J. Roberts, Alix Clarke, Meghan Elliott, Kathryn King-Shier, Swapnil Hiremath, Matthew Oliver, Robert R. Quinn and Pietro Ravani in Canadian Journal of Kidney Health and Disease
Footnotes
Ethics Approval and Consent to Participate
Ethics approval was obtained separately at all participating sites.
Consent for Publication
All authors have consented to publication.
Availability of Data and Materials
Data and materials cannot be made publicly available due to restrictions on its disclosure and use.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Oliver and Quinn disclose they are co-inventors of the Dialysis Measurement Analysis and Reporting system.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Roberts’ research is supported by funding from the Department of Surgery at the University of Ottawa. Dr Ravani holds Canadian Institutes for Health Research funding to support studies on hemodialysis access-related decision needs of patients, caregivers, and health care providers (FRN 162369). Dr Ravani is supported by the Baay Chair in Kidney Research at the University of Calgary.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.