
Abstract
Background:
Most studies addressing hemodialysis initiation with a dialysis catheter focus on patients entering maintenance dialysis programs and exclude other patients, such as those with acute kidney injury (AKI), making interpretation and application of the results difficult for clinicians managing patients at the time of dialysis commencement.
Objective:
To compare the survival of all patients requiring a catheter for hemodialysis access according to the nature of clinical presentation.
Design:
Prospective observational.
Setting:
An Australian tertiary renal unit.
Patients:
All patients requiring a central venous catheter (CVC) for hemodialysis access between 2005 and 2015.
Measurements:
Baseline comorbidities, demographics, and nature of clinical presentation. Data regarding each episode of dialysis access insufficiency and each CVC were collected. The primary outcome was all-cause mortality.
Methods:
Patients were classified into 1 of 3 groups based on physician assessment at the time of presentation: patients believed to have AKI with expected renal recovery (AKI), patients considered to be entering the maintenance dialysis program without a functioning dialysis access (Maintenance Dialysis), patients unable to perform peritoneal dialysis, or use their existing hemodialysis access (Access Failure). Time-split multivariable Cox regression analyses were used to compare survival between groups.
Results:
A total of 557 eligible patients had complete prospective data regarding CVC use and were included in the analyses. The majority of patients were in the AKI (246/557, 44%) and Maintenance Dialysis groups (182/557, 33%) compared with the Access Failure group (129/557, 23%). During a median follow-up of 3 years, 302 (54%) of the 557 patients died. Following adjustment, risk of all-cause mortality was higher in the AKI group (hazard ratio [HR]: 2.01, 95% confidence interval [CI]: 1.31-3.60, P = .001) during the first 2 years after catheter insertion and lower in years 2 to 4 (HR: 0.42, 95% CI: 0.20-0.88, P = .02) than in the reference Maintenance Dialysis group. No difference in mortality risk between the Access Failure and reference group was found.
Limitations:
Single-center study. Possible residual confounding owing to the observational study design.
Conclusions:
Patients requiring acute or unplanned hemodialysis experience high mortality, and the nature of clinical presentation does influence outcomes. Most notable is the greater early mortality experienced by patients with AKI compared to other patient groups. Prospective definition of the nature of unplanned dialysis initiation is important to accurately measure and improve outcomes in this high-risk patient population.
Human Research Ethics Committee Approval Number
CH62/6/2017-042.
Introduction
The requirement to initiate dialysis in an acute or unplanned fashion is common, and outcomes for these patients are worse than those starting in a planned manner.1-4 This need arises for a variety of reasons, including acute kidney injury (AKI), with clinicians often uncertain of the underlying diagnosis and the prospects for renal recovery in such patients. Prospective data to inform clinicians regarding prognosis and the factors that influence outcomes is sparse and mainly focusses on those entering maintenance dialysis programs. 5
Whilst the definition of “unplanned dialysis” remains variable, it is generally regarded as dialysis commencement in life-threatening or unscheduled circumstances, or the commencement of maintenance dialysis without a permanent access in place.6,7 Despite this, most studies addressing unplanned dialysis initiation exclude patients with AKI, usually based on the post hoc recovery of renal function allowing dialysis independence.1,5,8-10 Similarly, most reports of outcomes in patients with AKI requiring dialysis define AKI retrospectively when renal recovery is known,3,4 and thus do not capture the clinical uncertainty at the time of presentation, nor allow comparison of the relative risks of adverse outcomes in patients with different baseline diagnoses.
More recent prospective, observational studies11,12 and extended follow-up of randomized controlled trials 13 have described the high long-term mortality experienced by patients with AKI requiring dialysis but have largely focused on patients in intensive care units (ICU). Outside of an ICU setting, prospective studies of long-term outcomes following AKI have mostly examined patients not requiring dialysis. 14 As such, the current literature is not representative of the bulk of patients with AKI who require dialysis outside of an ICU setting and are predominantly managed by renal services worldwide. 15
We collected prospective data on all patients managed in a tertiary renal unit who required a central venous catheter (CVC) for dialysis access over a 10-year period and sought to compare patient survival by the clinical setting of dialysis requirement.
Methods
Study Design and Population
This prospective cohort study was conducted in the Renal Unit at Concord Repatriation & General Hospital (CRGH), a 750-bed adult tertiary teaching hospital in Sydney, Australia. The cohort consisted of all patients managed by the CRGH Renal Unit who required a CVC for hemodialysis (HD) access between May 1, 2005 and December 31, 2015. Eligible patients were defined as any inpatient or outpatient over 18 years of age who received a temporary or tunneled CVC for dialysis access regardless of etiology or expected chronicity of kidney replacement therapy (KRT). This included patients who commenced dialysis in the ICU and were discharged from ICU requiring ongoing dialysis treatment, but not patients initiated on KRT in ICU who died or achieved dialysis independence prior to ICU discharge. Patients with a failing transplant as the reason for dialysis initiation were excluded from the study due to the very small numbers of such patients, but a history of previous renal transplantation was not an exclusion criterion. Ethical approval for analysis and retrospective data linkage was granted by the Sydney Local Health District Human Research Ethics Committee (CH62/6/2017-042).
Nature of the Clinical Presentation
Consistent with other studies of dialysis CVC use, 16 eligible patients were identified at the time of CVC insertion and classified by the treating renal physician into 1 of 3 groups based on the reason for initial CVC insertion: (a) patients believed to have AKI, with expected recovery of renal function, were classified as AKI; (b) patients who were considered to be initiating maintenance dialysis without a usable existing permanent dialysis access in place were classified as Maintenance Dialysis; (c) patients requiring an interim CVC due to failure of their ability to perform peritoneal dialysis (PD) or failure of their existing HD access, were classified as Access Failure.
CVC Use
Patients may have had more than one CVC during any single episode and could have had multiple episodes during the 10-year study period. Each episode had its own classification, so patients could have had an episode that necessitated CVC insertion for new onset of Maintenance Dialysis followed by a later episode of Access Failure. Patients were analyzed based on the reason for CVC requirement at their first presentation only, such that in the example above, a patient presenting with Maintenance Dialysis followed by Access Failure would be analyzed as per the Maintenance Dialysis classification. Data regarding each episode and each CVC were collected for each patient in real time and entered into a database by a dialysis nurse. Each episode of dialysis access insufficiency was defined as from the time of initial CVC insertion to the first of; recovery of renal function to dialysis independence; establishment of a permanent functioning KRT access and removal of the CVC; a decision was made to continue with a long-term CVC and not pursue a non-CVC dialysis access; and dialysis withdrawal or death.
Data Collection and Covariates
Primary prospective data collection
Prospective data collection commenced at the date of first CVC insertion for each patient and included patient demographics and the details of each episode and CVC (including start date, duration, and reason for removal).
Retrospective data linkage
Following completion of prospective data collection, all eligible patients were linked to the CRGH inpatient data collection and the Australia and New Zealand Dialysis and Transplant Registry (ANZDATA). The CRGH inpatient data collection allowed derivation of private health insurance use, comorbidities, and mortality status. Comorbidities including: hypertension (HTN), diabetes (DM), ischaemic heart disease (IHD), peripheral vascular disease (PVD), and cerebrovascular disease (CBVD) were determined by the presence of relevant International Statistical Classification of Diseases, Tenth Revision, Australian Modification (ICD10 AM) codes in hospital admission records at the time of initial CVC insertion or within the preceding 12 months. ANZDATA records permitted the derivation of dialysis vintage, calculated as duration of PD and HD exposure prior to initial CVC insertion, and history of renal transplantation. Time with a functioning transplant was excluded from dialysis vintage duration.
Over the 10 years of prospective data collection, the nature of the episodes as well as CVC exposure were reviewed routinely within the CRGH Renal Unit with the purpose of reducing CVC exposure. Changes in practice during this time included appointment of a vascular access nurse specialist at commencement of the study and regular multidisciplinary team meetings between renal physicians, vascular surgeons, and dialysis nurses.
Outcomes
The primary outcome of this analysis was patient survival following initial CVC insertion, compared across the different reasons for initial CVC insertion. Survival analysis commenced at initial CVC insertion date for each patient and was censored at; date of transplantation in patients who received a kidney transplant, date of transfer in patients where care was transferred to another hospital who had unknown survival status, or at December 31, 2016, for all other patients, allowing at least 12 months of follow-up.
Statistical Analysis
Results are reported as counts and percentages for categorical variables, mean ± standard deviation for normally distributed continuous variables and median with interquartile ranges (IQRs) for non-normally distributed continuous variables. Unadjusted survival was illustrated using Kaplan-Meier curves. Multivariable adjusted hazard ratios and 95% confidence intervals were calculated using multivariable Cox regression models. The assumption of proportional hazards was not met, due to the changing effect of variables over time, so a time split approach was used where analyses were conducted at 2 yearly intervals following entry point. Variables selected for inclusion in multivariable models were based on clinical judgment and univariate assessment. Interactions were examined for variables within the models. The final model included the following: reason for CVC insertion (Maintenance Dialysis defined as the reference group), age, sex, dialysis vintage, year of admission, and comorbid information (DM, IHD, and PVD). To reflect real-world practice, only information known at the time of presentation were incorporated, and therefore, subsequent episodes of CVC requirement and recovery of renal function were not included in any model. For the same reason, we did not adjust for time-dependent covariates at the beginning of each time interval. Given the time-split approach used, the direct effect of year of admission could not be interpreted and has therefore not been reported; however, its inclusion was necessary to provide adjustment for changes in practice which occurred within the renal unit over the data collection period. Analyses were also performed using an additional multivariable model, which included the total number of comorbidities as a variable rather than the presence or absence of individual comorbidities. Sensitivity analyses were performed using multiple imputations by chained equations to impute 30 data sets for missing demographic, comorbid, and dialysis vintage data, which were assumed to be missing at random. A 2-sided p value of <.05 was considered statistically significant. All analyses were performed using Stata software (release 15.1, StataCorp, College Station, TX, USA). Patients with missing prospective data or no linkable record within the CRGH inpatient data collection were excluded.
Results
Participants
Between May 1, 2005 and December 31, 2015, 575 patients required a CVC for dialysis access. Of these, 18 were ineligible for inclusion due to incomplete data or the reason for CVC insertion being renal transplant failure. The remaining 557 eligible patients had complete prospective data regarding CVC use, which consisted of 751 separate episodes and 1067 CVC insertions.
Linkage of patients to the inpatient data collection excluded a further 88 patients due to incomplete data. Complete case survival analysis was therefore performed using 469 patients with complete primary and secondary data available (Figure 1).

Flow diagram describing study cohort derivation.
Cohort Characteristics
The baseline characteristics of the study cohort are presented in Table 1. The majority of patients were in the AKI (246/557, 44%) and Maintenance Dialysis groups (182/557, 33%) compared with the Access Failure group (129/557, 23%). Age differed between groups, with patients in the Maintenance Dialysis group (70 [53-78] years) younger than those in the AKI (72 [62-80] years) and Access Failure (72 [60-77] years) groups. Diabetes (46%) and HTN (77%) were more common in the Maintenance Dialysis group than the other groups (overall prevalence of 39% and 62%, respectively), but the use of private health insurance was less common in the Maintenance Dialysis group (18%). Despite the expectation of recovery to dialysis independence for patients in the AKI group, at the end of the episode of dialysis access insufficiency, only 54% (132/246) of patients in the AKI group were alive and not requiring KRT. Long-term survival without the need for KRT in the AKI group is presented in Figure S1. Renal recovery in the Maintenance Dialysis group was rare (3%).
Baseline Characteristics by Reason for CVC Insertion Group.

Note. The number of patients in each group is presented as absolute n and (percentage of patients) in each reason for CVC insertion group. Age and Dialysis Vintage are presented in years as median values with (interquartile ranges). CVC = central venous catheter; AKI = acute kidney injury (expected renal recovery); Maintenance Dialysis = patients considered to be entering the maintenance dialysis program; Access Failure = patients requiring an interim CVC due to failure of their ability to perform peritoneal dialysis or failure of their existing hemodialysis access; Comorbidities: Diabetes = diabetes mellitus; IHD = ischaemic heart disease; PVD = peripheral vascular disease; HTN = hypertension; CBVD = cerebrovascular disease; IQR = interquartile range.
529 patients with medical record data available.
476 patients with comorbidity data available from admission records within 12 months of CVC insertion date.
550 patients with dialysis vintage data available.
Table S1 shows the changing rate of new admissions to the cohort over time, with declining numbers of new presentations in the Maintenance Dialysis and Access Failure groups over the data collection period. As a result, the proportion of initial CVC insertions attributed to AKI within the cohort increased from 27% in 2005 to 59% in 2015.
Unadjusted Outcomes
The median follow-up duration was 3 [1-6] years, and 54% (302/557) of patients died. The unadjusted mortality rates for each group are presented in Table 2 and Figure 2, and show the high early mortality in all groups, especially the AKI group, and the relative moderation of mortality in the AKI group beyond 2-years of follow-up.
Unadjusted Mortality at Different Time Points of Follow-Up.

Note. The number of deaths is presented as absolute n/total number of patients and (percentage of patients) in each reason for CVC insertion group during the presenting episode, at 1-year and 3-year follow-up. The presenting episode is defined as from the time of initial CVC insertion to the first of; recovery of renal function to dialysis independence; establishment of a permanent functioning KRT access and removal of the CVC; a decision was made to continue with a long-term CVC and not pursue a non-CVC dialysis access; and dialysis withdrawal or death. CVC = central venous catheter; AKI = acute kidney injury (expected renal recovery); Maintenance Dialysis = patients considered to be entering the maintenance dialysis program; Access Failure = patients requiring an interim CVC due to failure of their ability to perform peritoneal dialysis or failure of their existing hemodialysis access; KRT = kidney replacement therapy.

Kaplan-Meier survival curves displayed for each reason for CVC insertion group.
Adjusted Outcomes
Results of the time-split multivariable Cox regression analyses are presented in forest plots in Figure 3. In the first 2 years following initial CVC insertion, the adjusted HRs for all-cause mortality were significantly higher for the AKI group (2.01, 95% CI: 1.31-3.06, P = .001) when compared to the reference Maintenance Dialysis group, but there was no difference seen between the Access Failure and reference group (Figure 3). During the period from 2 to 4 years following initial CVC insertion, the adjusted HR for all-cause mortality decreased to 0.42 (95% CI: 0.20-0.88, P = .02) in the AKI group when compared to the reference group, with no difference between the Access Failure and reference group. During years 4 to 6 following initial CVC, adjusted HRs for all-cause mortality were similar across all groups. Throughout the analysis, age was found to exert a significant effect on mortality with effect sizes between 1.03 and 1.05 per additional year of age, across the follow-up periods. Dialysis vintage, HR 1.10 per yearly increment (95% CI: 1.02-1.19, P = .01), and the baseline presence of IHD, HR 1.56 (95% CI: 1.09-2.23, P = .02), were also associated with significantly increased risk of all-cause mortality during the first 2 years after initial CVC insertion.
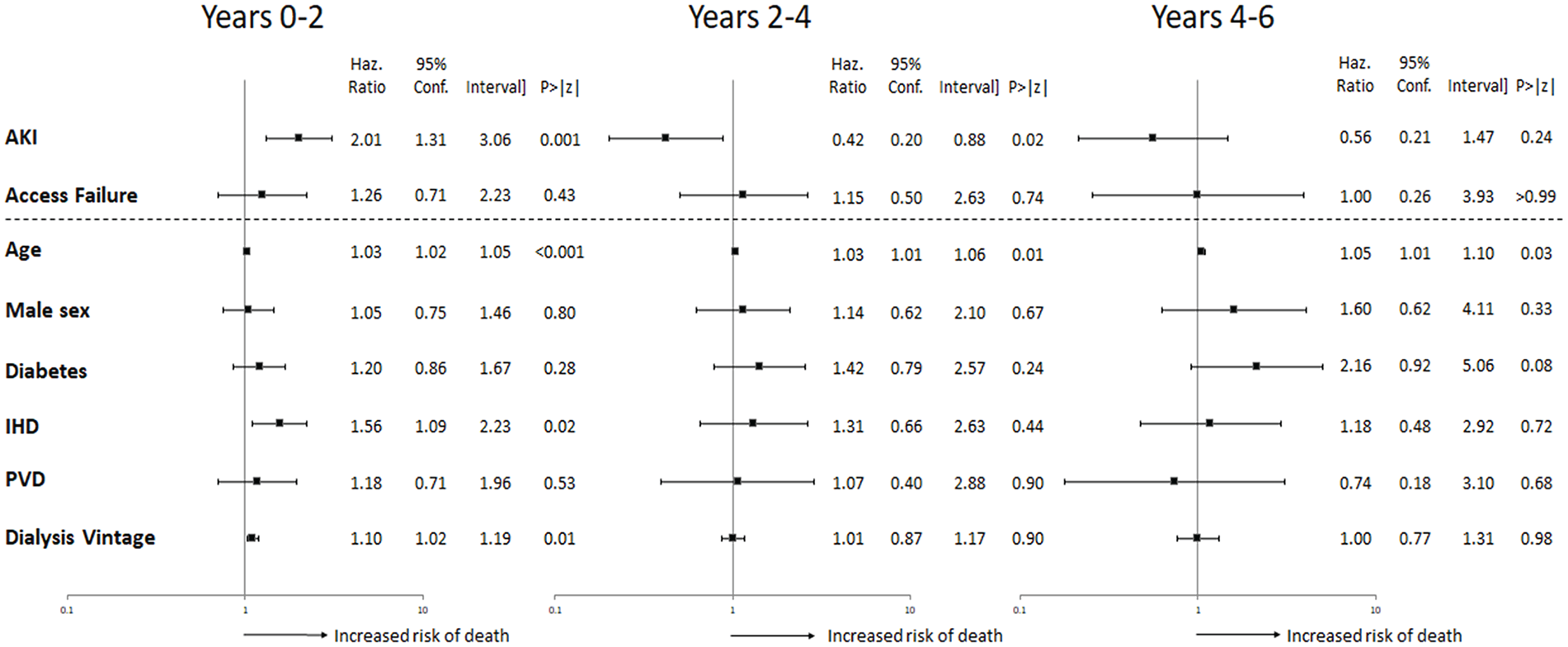
Time-split multivariate Cox regression analyses investigating the effect of reason for CVC insertion group on all-cause mortality.
Time-split multivariable Cox regression models using the total number rather than individual comorbidities demonstrated similar effects with regards to the risk for all-cause mortality due to the reason for CVC requirement over time; however, the number of incremental baseline comorbidities did not have a statistically significant affect at any time point (Figure S3). The effects of age and dialysis vintage were similar to the original models (Figure S3). Sensitivity analyses using multiple imputation for missing variables showed similar effects with regards to the risk for all-cause mortality due to the reason for CVC requirement and all other baseline variables over time (Table S2-S4).
Discussion
This long-term, prospective analysis of patients requiring unplanned HD with a CVC for dialysis access demonstrates the high mortality in all clinical settings, with less than 50% of patients surviving beyond 5 years. It also highlights the fact that the nature of the initial presentation does influence the survival of such patients, most notably seen in the higher early mortality rate of those with AKI, that diminishes with time, along with the fact that less than 50% of these patients are alive and KRT-free at 1 year. The prospective nature of case definition and the use of baseline characteristics for risk adjustment enhance the applicability of these findings to clinical practice and future study design.
Prospective studies of patients with AKI requiring dialysis managed within ICUs have demonstrated high 90-day, 12 1-year, 11 and long-term 13 mortality; however, prospective studies of patients with AKI requiring dialysis managed outside of ICUs are sparse. Eskola et al 17 compared 1- and 3-year outcomes in a prospective, multicenter study of such patients managed across both ICU and non-ICU settings. Of the 73 non-ICU patients, the mortality rate was 37% and 45% at 1- and 3-years, respectively, which is comparable to patients with AKI in our study. Importantly, in our cohort of patients, despite 81% of patients in the AKI group surviving their initial episode and 66% of those who survived recovering dialysis independence, only 52% were alive at the end of the study. This highlights the ongoing mortality risk of such patients beyond the initial admission.
Panocchia et al 18 reported high mortality (31%) in a prospective study of patients with chronic kidney disease (CKD) commencing unplanned dialysis between 2003 to 2009, despite follow-up being limited to hospital discharge and excluding patients with a prior history of dialysis requirement. This is higher than the mortality rates for patients commencing unplanned dialysis (AKI and Maintenance Dialysis groups combined) in our study, either during the presenting episode (16%) or at 1-year (24%). A possible explanation is that they excluded patients with normal baseline kidney function, which may highlight the impact of underlying CKD on outcomes in patients requiring unplanned dialysis. In both our study and the Panocchia study, 18 approximately two-thirds of patients (66% and 64%, respectively) classified as AKI who survived the episode recovered dialysis independence, which demonstrates the difficulty clinicians often face in predicting renal prognosis at dialysis commencement. Importantly, our results show a changing risk profile over time for patients with AKI requiring dialysis, such that the exclusion of patients who subsequently recover to dialysis independence from many studies addressing unplanned dialysis initiation may confound their findings. Our results also suggest that dialysis vintage and a history of IHD, but not the number of incremental comorbidities, at presentation significantly increase the risk of mortality in the first 2 years after CVC insertion.
The strengths of our study include prospective data collection and high rates of data completeness. We have extended follow-up of patients well beyond the index hospital admission and have collected data on all patients requiring a CVC for dialysis access including patients with previously normal and abnormal kidney function and those judged likely to recover dialysis independence. We have used only data available at the time of CVC requirement in our analyses with the purpose of making our results more relevant to clinicians treating patients at the time of unplanned dialysis commencement, when variables such as renal recovery, number of catheter days, measures of effective dialysis therapy or future development of comorbidities are not known.
The main limitation of our analysis is the reduced generalizability of our findings derived from a single Australian renal unit. We would expect our results to be consistent with comparable healthcare systems; however, the applicability of our findings to different populations is unknown. The exclusion of patients due to missing data is also a limitation; however, sensitivity analyses using multiple imputations for missing data show no significant differences in the effects reported. While there were only a handful of nephrologists responsible for classifying patients by the nature of their clinical presentation, it is possible that differing practice patterns between nephrologists could have influenced classification. The exclusion of patients with AKI in the ICU, as the care of such patients is not determined by the renal service, means our findings are only applicable to those patients who remain dialysis dependent at ICU discharge and are managed by a renal service. We have censored our analyses for kidney transplantation but were not able to adjust for other competing risks occurring after dialysis initiation. A reduction in the proportion of CVCs required for patients in the Maintenance Dialysis and Access Failure groups occurred over the course of the study as a result of changes in unit practice aimed at reducing catheter burden which could have influenced other clinical outcomes not recorded. We have tried to mitigate for this with adjustment for numerous covariates, including the year of presentation, but it is possible that residual confounding may still exist. Factors such as pre-existing CKD and the presence or absence of pre-dialysis care will likely have contributed to the nephrologist’s classification of reason for CVC insertion group in each case, but adjustment for these variables was not possible in this data set. It is possible that the effect of a CVC upon outcomes differs between patient groups and contributes to our findings; however, as the need for a CVC was common to all patients in this study, differentiating this further is beyond the capability of the study data set.
Conclusions
In conclusion, this large prospective study illustrates the poor long-term survival for all patients requiring a CVC for unplanned dialysis initiation in a tertiary renal unit. The nature of the data collection and analysis make these results relevant to clinicians in renal units treating patients at the time of dialysis commencement. Our findings support the evidence that AKI requiring dialysis is associated with higher early mortality rates and that renal recovery is seen in only around half of patients suspected to have recoverable AKI. The prospective definition of the cause for unplanned dialysis initiation is important in accurately measuring outcomes, appropriately informing clinicians and patients, and in designing future clinical studies in this high-risk population.
Supplemental Material
sj-pdf-1-cjk-10.1177_20543581211009986 – Supplemental material for The Impact of Clinical Presentation on Survival in Patients Requiring Hemodialysis Catheters for Acute and Unplanned Dialysis: A Prospective Observational Study
Supplemental material, sj-pdf-1-cjk-10.1177_20543581211009986 for The Impact of Clinical Presentation on Survival in Patients Requiring Hemodialysis Catheters for Acute and Unplanned Dialysis: A Prospective Observational Study by Benjamin Talbot, Ray Lin, Qiang Li, Min Jun, Sradha Kotwal, Shaundeep Sen and Martin Gallagher in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
All authors have provided consent for publication of this manuscript.
Ethics Approval and Consent to Participate
Ethical approval for analysis and retrospective data linkage was granted by the Sydney Local Health District Human Research Ethics Committee (CH62/6/2017-042).
Consent for Publication
All authors have provided consent for publication of this manuscript.
Availability of Data and Materials
The data underlying this article will be shared on reasonable request to the corresponding author and subject to approval from Sydney Local Health District Human Research Ethics Committee.
Author Contributions
Research idea and study design: B.T. and M.G.; statistical analysis: B.T., Q.L., M.J., and M.G.; supervision or mentorship: M.G. All authors contributed to data analysis/interpretation. Each author contributed important intellectual content during manuscript drafting or revision, accepts personal accountability for their own contributions, and agrees to ensure that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.T. is a clinical advisor for Ellen Medical Devices developing the Affordable Dialysis Project. M.G. is a lead for the REDUCCTION project that examines hemodialysis catheter complications. These are not seen as conflicts of interest but have been declared under Financial Disclosures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.