
Abstract
Background:
Literature on the outcome of acute kidney injury (AKI) in Sjogren’s syndrome (SJS) is quite scanty. Acute kidney injury has emerged as a significant cause of morbidity and mortality in patients with autoimmune diseases such as systemic lupus erythematosus.
Objective:
To examine the outcome of AKI with and without SJS. To achieve this, we examined the prevalence, mortality, outcomes, length of stay (LOS), and hospital charges in patients with AKI with SJS compared with patients without SJS from a National Inpatient Sample (NIS) database in the period 2010 to 2013.
Design:
A retrospective cohort study using NIS.
Setting:
United States.
Sample:
Cohort of 977 055 weighted patient discharges with AKI from the NIS.
Measurements:
Not applicable.
Methods:
Data were retrieved from the NIS for adult patients admitted with a principal diagnosis of AKI between 2010 and 2013, using the respective International Classification of Diseases, Ninth Revision (ICD-9) codes. The study population divided into 2 groups, with and without Sjogren’s disease. Multivariate and linear regression analysis conducted to adjust for covariates. We omitted patients with systemic sclerosis and rheumatoid arthritis from the analysis to avoid any discrepancy as they were not meant to be a primary outcome in our study.
Results:
The study population represented 977 055 weighted patient discharges with AKI. Analysis revealed AKI patients with Sjogren’s compared with patients without Sjogren’s had statistically significant lower hyperkalemia rates (adjusted odds ratio: 0.65, confidence interval: 0.46-0.92; P = .017. There was no statistically significant difference in mortality, LOS, hospital charges, and other outcomes.
Limitations:
Study is not up to date as data are from ICD-9 which are testing data from 2010 to 2013, and data were obtained through SJS codes, which have their limitations. Also, limitations included lack of data on metabolic acidosis, hypokalemia, and not including all causes of AKI.
Conclusions:
At present, our study is unique as it has examined prevalence, mortality, and outcomes of Sjogren’s in patients with AKI. Patients with Sjogren’s had significantly lower hyperkalemia during the hospitalization. Further research is needed to identify the underlying protective mechanisms associated with Sjogren’s that resulted in lower hyperkalemia.
Trial registration:
Not applicable.
Introduction
Sjogren’s syndrome (SJS) is a chronic progressive autoimmune disease that was first described by Henrik Sjögren in 1933. 1 Sjogren’s syndrome affects the exocrine glands, including salivary and lacrimal glands, which results in dryness of the mouth and eyes in more than 90% of the patients. Nearly one-quarter of patients may present with systemic manifestations, including peripheral neuropathy, interstitial lung disease, and cutaneous vasculitis.1-3 Sjogren’s syndrome is a relatively common disease with a prevalence of 0.23%.2,4 It usually affects middle-aged women with reported renal involvement up to 5% of patients with SJS through different mechanisms including lymphocytic infiltration causing tubulointerstitial nephritis (TIN), rarely associated with uveitis (Tinu syndrome) and immune complex–mediated process causing glomerulonephritis. 2 Moreover, TIN, both acute and chronic, is considered as the most common cause of renal disease in SJS and predisposes to both types 1 and 2 renal tubular acidosis (RTA).1,3
On the contrary, acute kidney injury (AKI), which is associated with a sudden drop in glomerular filtration rate, leads to a wide array of complications with significant morbidity and mortality. Several studies have concluded that AKI is associated with prolonged length of hospital stay, mortality, and higher resource utilization.5-7 Acute kidney injury is well known to be the primary cause of death in 3% of cases. 8 The average cost of a single hospital stay due to AKI might cost up to US$9200 (CAD $12 084), and a cost as high as US$4.6 (CAD $6) billion per year. 5 Acute kidney injury–associated mortality rate has decreased over the past 2 to 3 decades and is inversely correlated with the income of countries and the percentage of gross national product spent on total health care. 9
Methodology
Data Source
We used the 2010-2013 National Inpatient Sample (NIS) for this study as our database. The NIS is the largest all-payer database of inpatient hospital stays in the United States developed by the Agency for Healthcare Research and Quality (AHRQ) as part of its Healthcare Cost and Utilization Project (HCUP). The NIS contains more than 7 million unweighted hospitalizations per year. Discharge weights which is automatically generated and provided within the NIS database was applied. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) coding used to provide 25 discharge to 30, depending on the year and 15 procedures on each admission. The NIS discharge records include diagnoses, demographics, procedures, insurance, length of stay, hospital characteristics, and hospital charges. As the data collected from NIS, no institutional review board approval was required.
Variables and Outcomes
The NIS discharge date from 2010 to 2013 was analyzed in a retrospective cohort method. We used validated ICD-9 codes to include adults (≥18 years) hospitalized with principal diagnosis of AKI. Chronic kidney disease was identified with estimated glomerular filtration rate of less than 60 mL/min/1.73 m2. We also omitted patients with systemic sclerosis and rheumatoid arthritis all together from the analysis to avoid any discrepancy as they were not meant to be a primary outcome in our study. The appendix depicts the ICD-9 codes used. Patients’ baseline characteristics are outlined in Table 1. Charlson comorbidity index was calculated for comorbidities. Patients with AKI Sjogren’s were compared with patients without Sjogren’s in characteristics, length of stay (LOS), hospital charges, pulmonary edema, deep vein thrombosis, thrombophlebitis, pulmonary embolism, septic shock, and hyperkalemia. The primary outcome is in hospital mortality.
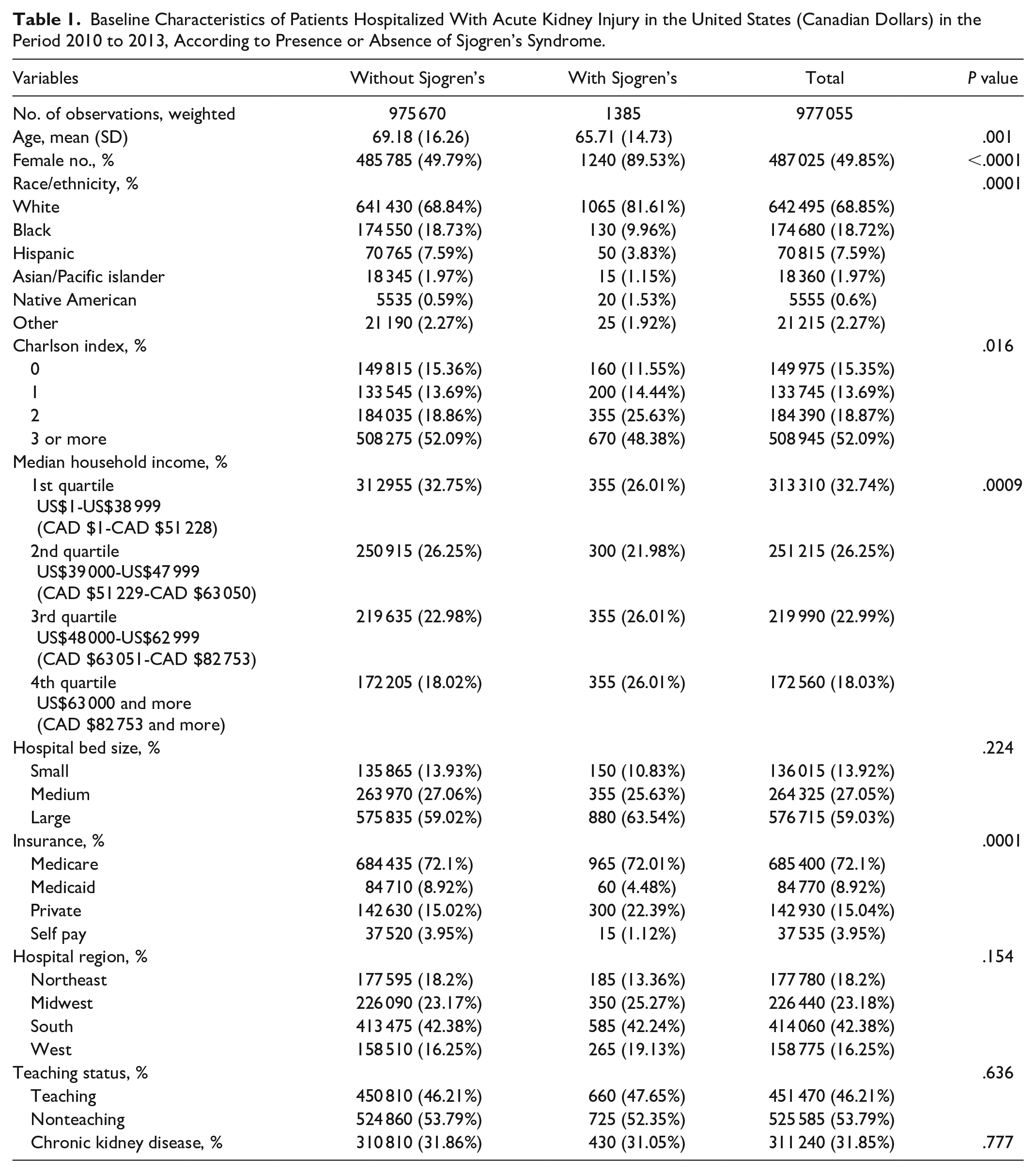
Baseline Characteristics of Patients Hospitalized With Acute Kidney Injury in the United States (Canadian Dollars) in the Period 2010 to 2013, According to Presence or Absence of Sjogren’s Syndrome.
Statistical Analysis
Statistical analyses in our study were performed using STATA 15 (Stata Corp, College Station, Texas). Categorical variables were stated in percentages, and continuous outcomes were stated in mean ± SD. Chi-square test and Student t test were used for categorical and continuous variables, respectively. To compare groups, we conducted logistic regression model for categorical outcomes and linear regression for continuous outcomes. Statistical significance was determined based on the P value of <.05. For outcomes, numeric results reported as mean and binary outcomes reported as an odds ratio (OR).
Results
Our study sample included 977 055 patients from the NIS database. Patients were all hospitalized with AKI with and without SJS diagnosis in the period from 2010 to 2013. As shown in Table 1, we found Sjogren’s cohort to be relatively younger with a mean age of 65.71 ± 14.73 years compared with 69.18 ±16.26 years for the group without Sjogren’s. In the AKI and Sjogren’s arms, females were the predominant gender accounting for 89.53% versus 49.79% in AKI without Sjogren’s arm. Regarding ethnicity, white patients constituted the majority, followed by blacks and then Hispanics with (68.85%, 18.72%, and 7.59%, respectively). Moreover, secondary in-hospital outcomes analysis reported lower rates of hyperkalemia complicating AKI admissions with Sjogren’s as compared with the AKI without Sjogren’s (OR: 0.65; 95% confidence interval [CI]: 0.46-0.92, P = .017; Table 2). We also found that nearly three-quarters had Medicare, followed by privately insured patients with the least number being on Medicaid. More than half of the population have received their treatment in a tertiary center hospital. Charlson index reported more than two-thirds of study subjects to have 2 or more comorbidities. After adjusting for patient-level characteristics, the crude and adjusted OR by logistic regression has shown (Table 3) that in-hospital mortality was not statistically significant between the AKI group with Sjogren’s versus AKI without Sjogren’s (OR: 1.22; 95% CI: 0.16-9.01, P = .844). Although statistically insignificant, higher rates of deep venous thrombosis (DVT), septic shock, and pulmonary edema were reported in patients with AKI and SJS. The charges of hospitalization and LOS were found to be statistically insignificant by the adjusted linear regression model shown in Table 3.
Crude and Adjusted Odds Ratio of In-Hospital Mortality and Clinical Outcomes of Patients Hospitalized With Acute Kidney Injury in the United States in the Period 2010 to 2013, According to Presence of Sjogren’s Syndrome by Logistic Regression Model.

Note. OR = odds ratio; CI = confidence interval; PE = pulmonary embolism.
Adjusted Linear Regression Model of Length of Stay and Hospital Charges (in US$) of Patients Hospitalized With Acute Kidney Injury in the United States in the Period 2010 to 2013, According to Presence or Absence of Sjogren’s Syndrome.

Discussion
Although previous literature has extensively addressed the association of AKI with cost and LOS, we are not aware of a single study with a special emphasis on the outcome of AKI and SJS. The annual number of inpatient deaths associated with AKI probably exceeds 40 000. 6 There were 497 observation unweighted patients with AKI and SJS in this study, and a prevalence rate of 0.14% (1385/977 055), which is much lower than the previously reported data. Regarding chronic renal involvement in SJS, a Chinese study has demonstrated renal tubular abnormalities prevalence as high as 33.5% (192/573) in patients with primary SJS. 10 In contrast, a study by Goules has found a lower prevalence of renal involvement in SJS of only 5%. 11 This wide discrepancy might be ascribed to the higher number of patients in the Chinese study. Also, we found that hospitalizations complicated by AKI-associated SJS were more costly US$38 867 (CAD $51 054) as compared with general AKI hospitalizations without SJS. This indicates that SJS, as a confounding factor in patients with AKI, is associated with an increasing burden on annual health care expenditure. This might be explained by their need for complicated immunosuppressive regimens.
Furthermore, this is clearly shown by studies of Silver and Zeng which demonstrated that AKI was associated with an increase in hospitalization costs of US$7933 (CAD $10 420) (95% CI: US$7608-US$8258) (CAD $9993-CAD $10 847) as well as an increase in LOS of 3.2 (95% CI: 3.2-3.3).7,12 This is also in keeping with a study published by Chertow et al 13 who has reported the mean cost of hospitalization to range between US$4900 (CAD $6436) (adjusted) and US$8900 (CAD $11 690) (unadjusted). In this particular study, serum creatinine was used as a parameter to diagnose AKI. 13 These higher adjusted estimates may reflect application of multivariable models, which did not adjust for several significant determinants of cost, including several procedures and hospital-level variables. Moreover, another study at the same academic center in 2010, and after adjusting for several procedures, has found AKI to be associated with a rise in cost US$7082 (CAD $9302) and 2.8-day increase in LOS. 7 However, this study was unable to adjust for hospital-level variables because of its limitation as a single-center design. Fischer et al 14 was able to adjust for hospital teaching as well as the inclusion of 23 community hospitals, with demonstration of more AKI in patients with SJS when hospitalized in community hospitals compared with university centers, 52.35%, and 47.65%, respectively. Also, patients with AKI were more prone to more extended intensive care units as well as overall hospital stay. 15
Moreover, the explanation of increased reporting of septic shock, DVT, and pulmonary edema is most likely multifactorial, and it is beyond the scope of this article to go into details. Although hyperkalemia is a common finding with severe AKI, our study has found less prevalence of hyperkalemia in AKI with SJS, and this is quite fascinating. This might be explained by the previous predisposition of a patient with SJS to chronic proximal and distal RTA. In contrast, hyperkalemia is uncommon in SJS, with RTA type 4 being quite an unusual finding. 16
At present, our study is unique as it has examined outcomes, LOS, and hospitalization in AKI and SJS. However, it has a few limitations as a case-control study, which could be summarized as follows:
Data were obtained through SJS codes, which have their limitations. The SJS diagnosis might be flawed with errors and inaccuracy of information available on admission as well as details missed by health care providers. Study is not up to date as data are from ICD-9 which are testing data from 2010 to 2013. Also, not all causes of AKI are included.
A particular risk factor or situation when retrieved by SJS codes cannot be substantiated independently. In addition, unbundling and upcoding can lead to a significant potential source of error. 17
Conclusions
Even with these limitations, database studies are still useful to study uncommon diseases like SJS. Prospective studies are urgently needed to unravel the relationship between AKI and SJS, which might have a direct impact on health care expenditure. In-hospital mortality, charges of hospitalization, and LOS were not statistically significant between the AKI groups with Sjogren’s versus AKI without Sjogren’s. Lower rates of hyperkalemia were a significant finding in patients with Sjogren’s, which needs to be examined in further studies.
Footnotes
Appendix
ICD-9 Codes Used to Identify Diagnoses.

| Diagnosis or procedure | |
|---|---|
| Acute kidney injury | 584.9 |
| Sjogren’s syndrome | 710.2 |
| End-stage renal disease | 585.6 |
| Chronic kidney disease | 585.3, 585.4, 585.5 |
| Scleroderma | 701.0 |
| Systemic sclerosis | 701.1 |
| Rheumatoid arthritis | 714.0, 714.3 |
| Pulmonary edema | 518.4 |
| Deep venous thrombosis/thrombophlebitis | 451.1, 451.11, 451.19, 451.2, 451.8, 451.81, 451.83, 451.84, 451.89, 451.9, 453.2, 453.8, 453.9 |
| Septic shock | 785.52 |
| Hyperkalemia | 276.7 |
| Pulmonary embolism | 415.1, 415.19 |
Note. ICD-9 = International Classification of Diseases, Ninth Revision.
Ethics Approval and Consent to Participate
This study was obtained from national inpatient sample which is public.
Consent for Publication
All authors reviewed and approved the final version of this manuscript.
Availability of Data and Materials
All relevant data and materials are contained in the appendices.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.