
Abstract
Background:
Hyperkalemia is a potentially life-threatening electrolyte abnormality defined as a serum potassium above the lab reference range (usually >5.0-5.5 mEq/L). Polystyrene resins, including sodium polystyrene sulfonate (SPS) and calcium polystyrene sulfonate (CPS), have long been used to treat hyperkalemia. Sodium polystyrene sulfonate/calcium polystyrene sulfonate act by exchanging a cation for potassium within the intestinal lumen. While SPS and CPS have been available since the 1960s, there are rising concerns about the validity of the data supporting its use and about serious adverse gastrointestinal effects.
Objective:
The objective of this systematic review was to quantify the efficacy and safety of polystyrene sulfonate resins (SPS/CPS) in the treatment of adults with hyperkalemia. This review focuses on the randomized control trial (RCT), interventional non-RCT, and observational data available on SPS/CPS use.
Design:
Systematic review.
Setting:
Any country of origin. Both inpatient and outpatient settings.
Patients:
Adults with hyperkalemia treated with polystyrene sulfonate resins.
Measurements:
The primary outcome was change in serum potassium. The secondary outcomes included adverse effects of SPS/CPS and prevention of recurrent hyperkalemia.
Methods:
We conducted a systematic review using Cochrane Library, EMBASE (1947-2019), and Medline (1946-2019) databases. Literature reviews, systematic reviews, case studies, case series, and editorial pieces were excluded. Included studies were assessed for risk of bias.
Results:
Four RCTs, 21 observational studies, and 5 quasi-experimental trials were included. A total of 212 351 patients were included. Two thousand and fifty-eight patients were studied for the primary outcome and 210 293 patients were studied for the secondary outcomes. Study designs were heterogeneous and not amenable to meta-analysis. Most studies included nonhemodialysis outpatients older than 65 years. Of the included studies, 22/25 (88%) demonstrated a reduction of serum potassium >0.5 mEq/L over the study period. The magnitude of reduction in serum potassium of potassium resin compared with placebo or matched controls in the 3 low-risk studies identified was 0.14 to 1.04 mEq/L. However, each study used different dosing regimens. Ten of 22 studies reported the effects of polystyrene resins on serum potassium within 24 hours. A few high-quality observational studies suggest an increased risk of serious adverse gastrointestinal events with a relative risk of 2.10 and a hazard ratio of 1.25 to 1.94; however, the absolute risk remains low. The incidence of adverse gastrointestinal events is 16 to 23 events per 1000 person-years.
Limitations:
We acknowledge several limitations in this study. Case studies and case series were excluded from the search results. Large case series may have been excluded despite having comparable sample sizes to studies included due to lack of a comparator and calculated estimates. Due to the heterogeneity of the studies, the data were unable to be meta-analyzed and as such the potassium-lowering effect of polystyrene sulfonate resins remains founded on small studies with potential confounders.
Conclusions:
This systematic review demonstrates a continued lack of high-quality evidence for the use of SPS/CPS in hyperkalemia. Studies investigated highly variable timelines and the most robust evidence for SPS/CPS use is in chronic hyperkalemia. While the absence of high-quality evidence does not exclude the possibility of benefit, prescribers must understand that the use of SPS/CPS in acute hyperkalemia is not supported by high-quality evidence.
Trial registration:
The protocol for this systematic review was not registered.
Introduction
Hyperkalemia is a common and potentially life-threatening electrolyte abnormality defined as a serum potassium concentration above the upper limit of normal (5.0-5.5 mEq/L). The estimated prevalence of hyperkalemia in patients with chronic kidney disease (CKD) without renal replacement therapy is 9.6%. 1 Those requiring renal replacement therapy in the form of hemodialysis and continuous ambulatory peritoneal dialysis have a prevalence of 16.5% and 10.6%, respectively. 1 An increase in extracellular potassium lowers the cardiac membrane potential and predisposes the heart to fatal arrhythmias. 2 Observational data have demonstrated a U-shaped association between serum potassium and mortality.3 -6 A variety of management options are available including pharmacological (intracellular shifting and increasing excretion) and nonpharmacological (dietary restriction and renal replacement therapy).7 -9 One such pharmacological therapy for hyperkalemia is the use of potassium binding resins: sodium polystyrene sulfonate (SPS) and calcium polystyrene sulfonate (CPS). These resins are administered orally or rectally and exchange their respective cation for the potassium ion within the large intestine. While these agents have been considered one of the few pharmacological methods of potassium elimination, the literature supporting their use is inconsistent. In the United States, the approval of SPS was based largely on a study by Scherr et al published in 1961 conducted on 32 patients with hyperkalemia. 10 With a mean dose of 40 g of SPS in water per day, the study demonstrated a reduction of serum potassium of 1.8 mEq/L over the mean duration of 3 days and 1.0 mEq/L in the first 24 hours in the oral SPS group. However, the efficacy of SPS has recently been questioned.11 -13 The lack of placebo-controlled studies as well as the concomitant use of a low-potassium diet and dextrose in the Scherr study created a challenge in establishing the true effect of SPS. The lack of placebo-controlled trials may be in part due to the ethical implications of withholding a potentially efficacious treatment for which few alternatives exist.
In addition, there have been concerns for severe adverse events, primarily colonic necrosis. 14 Following the Scherr et al 1961 study, Flinn et al added the cathartic sorbitol to the preparation to improve delivery of the medication to the colon. 15 This study prompted the widespread use of sorbitol with SPS due to apparent increased efficacy. In the subsequent decades, case studies on intestinal ischemia were reported with SPS use. Initial case reports showed that postoperative patients, patients with uremia, and those exposed to SPS with sorbitol were the patients most at risk.16,17 In 2009, the U.S. Food and Drug Administration (FDA) subsequently published a black box warning highlighting the association with colonic necrosis and recommended against coadministration with sorbitol. 8 The role of sorbitol in generating intestinal injury remains unclear. Two studies using rat models, Ayoub et al and Lillemoe et al, provide conflicting conclusions on the culpability of SPS in the observed mortality and colonic necrosis.18,19 Despite a lack of a demonstrated causal relationship, there has been a shift to administering polystyrene sulfonate resins with water since the 2009 FDA recommendation. Previous systematic reviews studying the serious gastrointestinal (GI) adverse events associated with SPS use have assessed case report and case series data and therefore have been unable to provide data on incidence and prevalence of adverse GI events associated with polystyrene resin use. 14
Treatment of hyperkalemia can be divided into therapies for acute and chronic hyperkalemia.20,21 These terms are not well-defined in the literature. However, there is evidence that supports that the rate of hyperkalemia development is clinically relevant. 2 Treatment modalities can also be classified into acute and chronic treatments based on their time of onset and duration of effect. 21
Previously published reviews have predominantly examined the data from randomized control trials (RCTs).7,8 Both Batterink et al and Mahoney et al only identified one RCT by Gruy-Kapral et al from 1998 which demonstrated no difference 4 hours after resin administration. 22 In 2017, a systematic review published by Palaka et al was the first to include observational studies in the review. 23 Palaka et al identified 3 RCTs on SPS/CPS which included a total of 136 participants. While observational studies were included, they were not discussed or analyzed beyond a count of the number of available articles. The review primarily focused on a variety of management strategies for hyperkalemia beyond SPS/CPS.
Objective
The objective of this systematic review was to identify the literature investigating the efficacy and safety of polystyrene sulfonate resins (SPS/CPS) in the treatment adults with hyperkalemia. The questions we aimed to address were as follows: (1) What is the direction and magnitude of effect of polystyrene resins on serum potassium in adults with hyperkalemia? (2) What adverse events are associated with polystyrene resin use? This review focuses on the RCT, interventional non-RCT and observational data available on SPS/CPS use. Data from studies without controls, placebo controls, and active comparators were included in this review.
Methods/Search Strategy
A systematic review was conducted using the EMBASE (1947-2019), MEDLINE (1946-2019), and Cochrane Database of Systematic Reviews databases. The search was initially performed on July 13, 2018 and updated on October 6, 2019. Citations of previous reviews were also searched. Terms for hyperkalemia were combined with terms for cation exchange resins, SPS, CPS, and their brand names. The full search strategy can be found in the Supplemental Material. The protocol was not published or registered prior to completion of the systematic review. Two independent reviewers (S.W.S.W. and G.Z.) screened the titles, abstracts, and full papers against eligibility criteria.
Eligibility Criteria
We conducted a systematic review and meta-analysis of primary research literature that included full-text, English language, original RCTs, and observational studies. Our population of interest was adult patients above 18 years of age who received a polystyrene sulfonate resin for the treatment of hyperkalemia. Supplemental Table 1 summarizes the inclusion and exclusion criteria of our review. Studies were included that examined the management of hyperkalemia in adult patients with SPS or CPS with outcome data on reduction of serum potassium level and/or adverse events. Hyperkalemia was defined as a serum potassium >5.0 mEq/L. A lower threshold for defining hyperkalemia allows this review to capture a broader scope of literature including mild hyperkalemia. Studies without controls, with placebo controls and with active controls, were included. Literature reviews, systematic reviews, case studies, case series, and editorial pieces were excluded. For this study, nonrandomized interventional study designs were categorized as quasi-experimental studies and were included. Discrepancies were resolved by consensus.
Data Extraction and Outcome Measures
All included studies were assessed by 2 authors for data extraction. The primary outcome was the change serum potassium. The secondary outcomes were the incidence of adverse GI events associated with the use of polystyrene resins, hypokalemia, hypercalcemia, and rates of recurrent hyperkalemia. A broad definition of adverse GI events was used, including intestinal necrosis, ischemia, perforation, or ulceration. Additional post hoc secondary outcomes were added including hypernatremia, hypomagnesemia, weight gain, and funding sources.
Study characteristics were also collected including type of intervention, dose of resin, single dose or multidose, time to outcome, and number of included study participants.
Bias Assessment
Articles were independently assessed by each reviewer (S.W.S.W. and G.Z.) and dichotomized to low/high risk of bias based on standardized scoring systems. An RCT was considered low risk if it satisfied a score of 8 or more based on the Cochrane Risk of Bias Tool 2.0. 24 An observational study was considered low risk if it satisfied a score of 8 or more based on the Newcastle-Ottawa Criteria. 25 All nonrandomized interventional study designs (Quasi-experimental) were assessed using the Risk of Bias In Non-randomized Studies of Interventions (ROBINS-I) assessment tool. 26
Statistical Analysis
The data abstracted from this systematic review were not amenable to meta-analysis due to significant heterogeneity in populations, intervention, and measurement of effects. A sensitivity analysis could not be performed due to the low number of studies considered to be at low risk of bias. To determine the direction of effect, vote counting and a corresponding sign test were performed according to the Cochrane Handbook of Systematic Reviews of Interventions Version 6.0. 27 Studies considered in favor of intervention if a reduction of greater or equal to 0.5 mEq/L was achieved. There is no consensus on a clinically relevant reduction in serum potassium and so this value was set by the authors of this study. Qualitative analyses were performed on the study characteristics and secondary outcomes. A post hoc analysis was performed on the effect of potassium binding resins on weight gain, serum sodium, and magnesium.
Results
We identified 867 relevant articles (Figure 1). After applying the exclusion criteria and removal of duplicates, 30 articles were eligible for inclusion (Table 1).10,12,15,28-54 Of the included studies, 4 studies were RCTs, 21 were observational studies (Table 2), and 5 studies were nonrandomized interventional study designs (quasi-experimental study designs) (Table 3). Most of the literature was published since 2010: 4 articles were published before 1990, 1 between 1990 and 2000, 3 between 2000 and 2010, and 22 were published since 2010. A total of 212 351 patients were included in these studies with 208 patients within the RCTs, 1766 patients in observational studies investigating the primary outcome, 210 293 patients in observational studies investigating secondary outcomes, and 84 patients in quasi-experimental study designs. In total, 2058 patients were included in studies investigating the primary outcome and 210 293 patients in studies investigating the secondary outcomes.
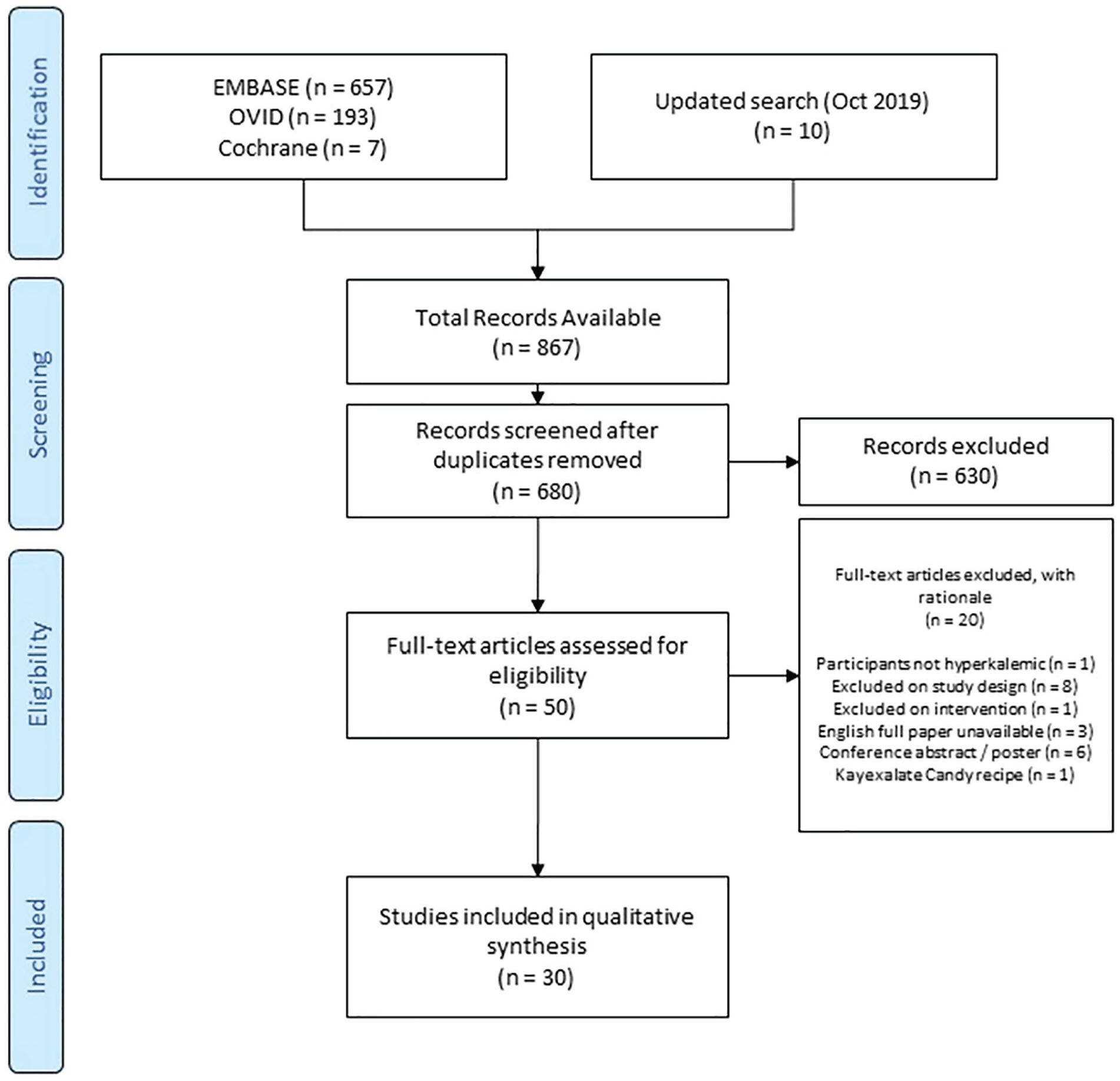
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram.
Study Characteristics of Randomized Control Trials on Polystyrene Exchange Resins.

Note. eGFR = estimated glomerular filtration rate; SPS = sodium polystyrene sulfonate; CKD = chronic kidney disease; CPS = calcium polystyrene sulfonate; SCr = serum creatinine.
Study Characteristics of Observational Studies on Polystyrene Exchange Resins.
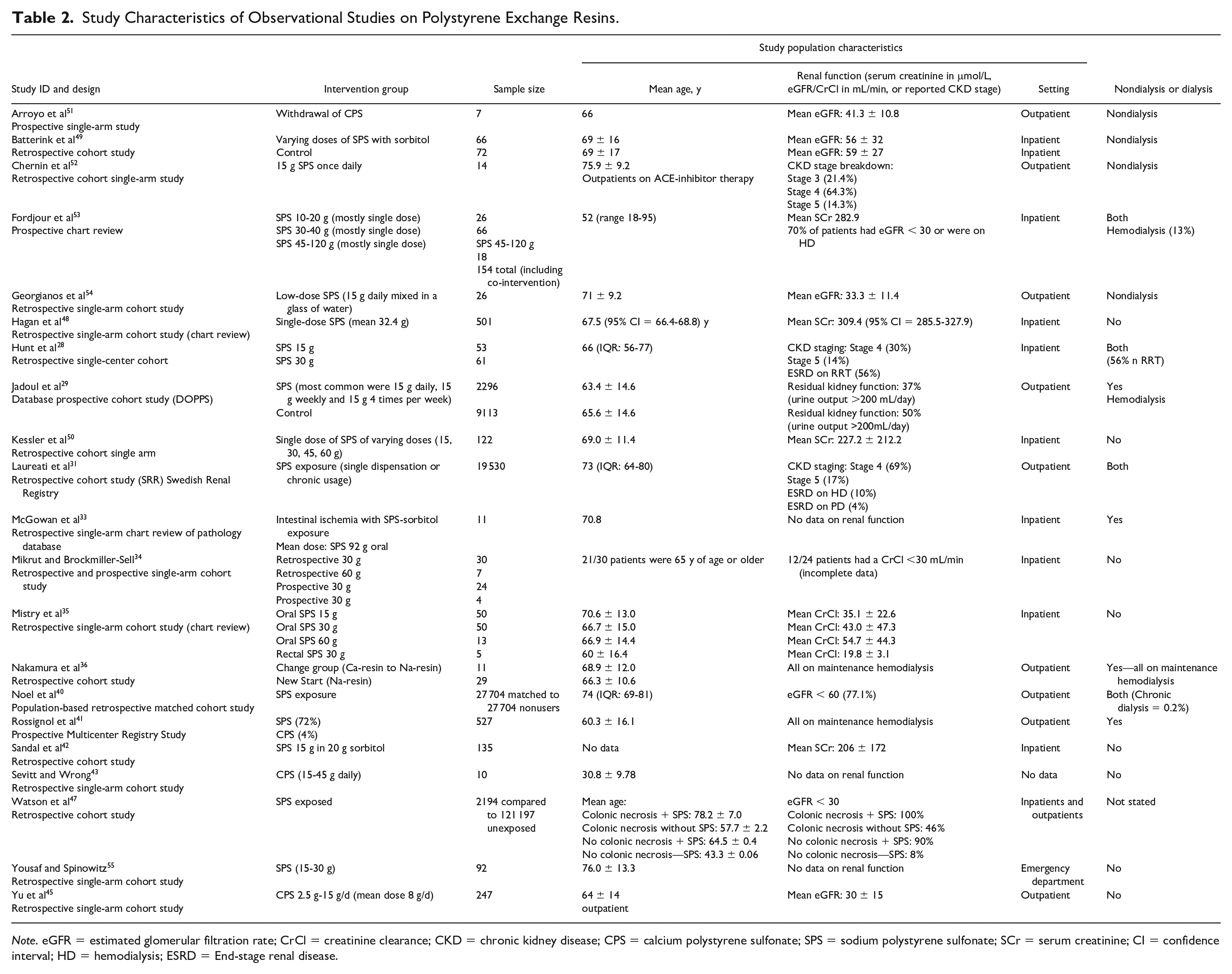
Note. eGFR = estimated glomerular filtration rate; CrCl = creatinine clearance; CKD = chronic kidney disease; CPS = calcium polystyrene sulfonate; SPS = sodium polystyrene sulfonate; SCr = serum creatinine; CI = confidence interval; HD = hemodialysis; ESRD = End-stage renal disease.
Study Characteristics of Quasi-Experimental Studies on Polystyrene Exchange Resins.
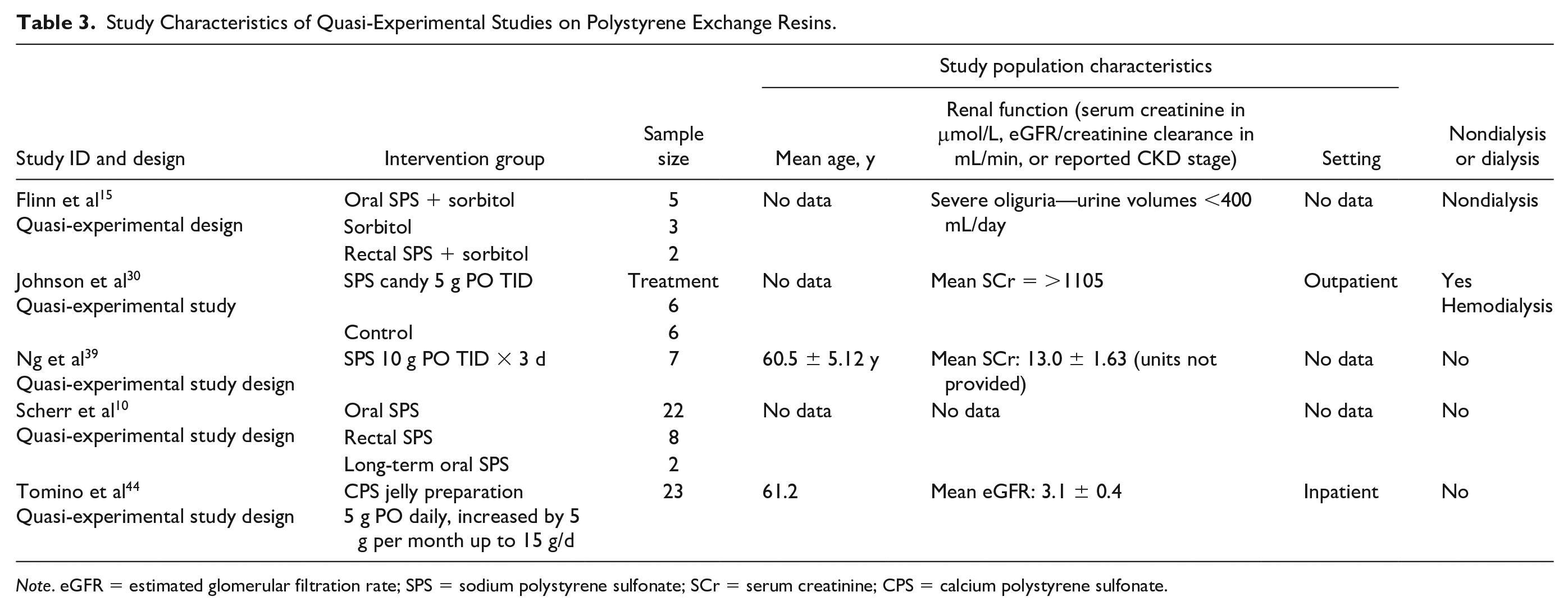
Note. eGFR = estimated glomerular filtration rate; SPS = sodium polystyrene sulfonate; SCr = serum creatinine; CPS = calcium polystyrene sulfonate.
Study Characteristics
Included Study Designs
This systematic review identified 4 RCTs investigating the use of polystyrene resins in the setting of hyperkalemia.32,37,38,46 Lepage et al and Wang et al studied the efficacy of polystyrene resins in placebo-controlled trials. Nakayama et al and Nasir and Ahmad compared SPS with an active comparator, CPS. These 2 trials were included as they provided valuable data on the magnitude of reduction in serum potassium with both CPS and SPS. However, it was felt to be of similar quality to the other data in this review and thus was included. The inclusion of such data does not change the overall conclusions of the review. All RCTs studied outpatients exclusively. Nasir and Ahmad specifically studied patients presenting to the emergency department. Only Wang et al conducted an RCT examining the effect of polystyrene exchange resins in patients treated with hemodialysis.
Setting
Of the included studies, 14 (46%) studied outpatients exclusively, 2 (6.7%) articles studied patients in the emergency department. Nine (30%) studies investigated inpatients exclusively. Only 1 (3.3%) study conducted by Watson et al included both inpatients and outpatients. Four (13%) studies provided no data on the setting.
Population Characteristics
Most studies provided data on elderly patients with documented renal dysfunction in the outpatient setting. However, there was significant heterogeneity. In studies investigating the primary outcome, the mean age of participants was 66.2 years. The mean age of participants in studies investigating secondary outcomes was 49.0 years; however, the mean age was significantly affected by the younger matched control group in the article by Watson et al. 47 The mean age of participants of articles investigating secondary outcomes excluding Watson et al is 70 years. Seventeen (57%) studies included patients with a mean age above 65 years, 4 (13%) studies included no information about the age of their study population.
Four (13%) studies included both patients on hemodialysis and those without. Six (20%) studies investigated the effect of polystyrene resins exclusively in patients on maintenance dialysis, 19 (63%) articles were included that studied nondialysis patients. The observational study by Watson et al did not specify the inclusion of patients on hemodialysis.
Of the 23 studies that included patients not on hemodialysis, 3 (13%) reported no data on renal function, 4 (17%) articles reported mean serum creatinine >200 μmol/L, 8 (35%) studies reported estimated glomerular filtrate rate (eGFR), creatinine clearance (CrCl), or CKD staging consistent with a mean CrCl less than 30 mL/min/1.73 m2. Six (26%) studies reported either eGFR or CrCl between 30 and 60 mL/min/1.73 m2. Flinn et al reported that patients were oliguric, with no further details on renal function. 15 Nasir and Ahmad 2014 reported that patients had a range of CKD stages from I to IV. 38 Overall, most articles that reported either renal function studied patients with a CrCl or eGFR of less than 60 mL/min/1.73 m2.
Interventions
Ten studies (45%) investigating the primary outcome utilized a single-dose resin. Seventeen (57%) of studies investigated the primary outcome using SPS and 3 (10%) using CPS. Both Nakayama et al and Nasir and Ahmad studied both SPS and CPS. Sodium polystyrene sulfonate dosing was studied between 15 g daily up to 60 g per day. Calcium polystyrene sulfonate was studied at lower doses ranging from starting doses of 5 to 15 g per day.
Time to Outcome
The reported time to effect of polystyrene sulfonate resins was variable between studies. Of the 22 included studies investigating the primary outcome, 5 (23%) reported outcomes in less than 12 hours, 5 (23%) reported outcomes within 12 to 24 hours, 5 (23%) reported outcomes within 1 to 7 days, and 7 (32%) reported outcomes assessed beyond 7 days.
Co-intervention
Hyperkalemia is often treated with multiple agents concomitantly including insulin, beta-agonists, and diuresis. These confounders may result in overestimation of the effect of cation resins. Of the 13 observational studies studying the primary outcome, 7 excluded co-intervention, 4 studies likely did not have co-intervention but did not explicitly exclude co-intervention (Chernin et al, Georgianos et al, Nakamura et al, Yu et al), and 2 studies (Hagan et al, Yousaf et al) included co-intervention. Of the quasi-experimental study designs, only Scherr et al documented co-intervention. The remaining 4 studies did not explicitly exclude co-intervention but were unlikely to co-administer other agents for hyperkalemia.
Risk of Bias
In the included RCTs, risk of bias overall was low as assessed by the Cochrane Risk of Bias Tool. Studies were largely well-designed albeit with small sample sizes. However, only the trials by Lepage et al and Wang et al were considered strictly to be at low risk of bias. Both Nakayama et al and Nasir and Ahmad compare SPS with an active comparator CPS. Therefore, its effect compared with placebo is not able to be elucidated. In addition, the open-label nature of trial by Nakayama et al could introduce bias. Furthermore, the randomization process was also not clearly outlined by Nasir and Ahmad. Despite these, the objective measure of serum potassium was protective in ensuring the validity of these findings.
Observational studies were assessed by the Newcastle-Ottawa Criteria and only 6 studies were low risk of bias. Only 2 observational studies examining the primary outcome, Batterink et al and Nakamura et al were at low risk of bias. The remaining 3 studies investigated secondary outcomes at a population level (Jadoul et al, Noel et al, Rossignol et al, Watson et al). The high-risk studies were designated as such largely due to the lack of comparator groups.
The quasi-experimental studies were assessed using the ROBINS-I tool. All studies were at serious or critical risk of bias. Overall, the studies included few participants, had missing demographic data, or lacked comparator groups.
Outcomes
Primary Outcome
Reduction in serum potassium
This systematic review demonstrates that the current evidence for polystyrene use in hyperkalemia is heterogeneous and has a paucity of high-quality placebo-controlled studies (Table 4). Current literature from observational studies largely support the use of SPS/CPS for lowering serum potassium. There is no consensus on a clinically significant reduction in serum potassium, we defined a clinically significant difference as a reduction in serum potassium of 0.5 mEq/L. In total, 88% of the 25 included studies favored intervention (P < .001). Notably, of the 23 studies that reported an outcome as a reduction in serum potassium 2 of 4 (50%) RCTs, all 13 observational studies and 4 of 5 (80%) quasi-experimental studies demonstrated a reduction of >0.5 mEq/L during the study period (Figure 2 and 3).
Primary Outcome Data on Polystyrene Exchange Resins.

Note. SPS = sodium polystyrene sulfonate; CI = confidence interval; CPS = calcium polystyrene sulfonate; HD = hemodialysis; ESRD = End-stage renal.

Change in serum potassium in intervention group of studies examining primary outcome within 72 hours.

Change in serum potassium in intervention group of studies examining primary outcome after 72 hours.
A dose-dependent reduction of serum potassium was also observed in 5 observational studies (Fordjour et al, Hunt et al, Kessler et al, Mistry et al, and Yu et al). Four studies investigated the effect of SPS/CPS over time. Sandal et al observed a progressive decline reaching a minimum serum potassium at 18 to 24 hours. Flinn et al and Ng et al reported a continued decline in serum potassium at 6 and 3 days, respectively. In contrast, Tomino et al demonstrated a continued decline in potassium 3 months after initiation of treatment; however, there were monthly increases in doses.
A sensitivity analysis including only low-risk studies revealed that only the study by Lepage et al demonstrated a reduction of greater than 0.5 mEq/L (1.04 mEq/L) when compared with placebo. Both other low-risk studies by Wang et al and Batterink et al demonstrated an additional reduction in serum potassium of 0.38 and 0.14 mEq/L compared with placebo or matched controls. While both differences were statistically significant, the clinical significance of small reductions in serum potassium is unclear. Notably, the Wang et al trial used a low dose of CPS, 5 g 3 times a day over the study period. Of the participants in the Batterink et al study, 47% received a single dose of 30 g of SPS dose and 48.5% received a single 15-g dose.
In summary, the data from the 2 low risk of bias studies suggest a serum potassium reduction of 0.14 mEq/L in 6 to 24 hours and 0.38 mEq/L in 3 weeks.8,46 Other data from observational data and RCTs with active comparators estimate a more generous effect on potassium reduction. The reduction in serum potassium ranges from 0.3 to 2.25 mEq/L with the effect varying with dose and duration of therapy.10,34 Several studies support a dose-dependent reduction in serum potassium with escalating resin doses.28,35,45,50,53 Overall, the current evidence supports a small reduction in serum potassium with the use of polystyrene sulfonate resins. Most of the current literature is observational and lacks appropriate controls. The results of this review do not change in the direction of effect after a sensitivity analysis excluding studies at high risk of bias.
Secondary Outcomes
GI adverse events
The risks of polystyrene resin use have been better elucidated in observational data in recent years (Table 5). In 2012, Watson et al published a retrospective cohort study providing the first estimations of relative risk and absolute risk of pathologically demonstrated colonic necrosis in SPS use. The reported 9-year cumulative incidence of colonic necrosis was 0.14% with a relative risk of 2.10 that was not considered significant. The number needed to harm was 1395 in the entire cohort and 631 in patients above the age of 65 years. The authors concluded that there was no increased risk associated with SPS use. Subsequent studies by Laureati et al and Noel et al expanded the scope to include other serious adverse GI events including ulcer, perforation, and ischemia. They reported an overall increase in serious adverse GI events associated with SPS use. The reported hazard ratios were 1.25 and 1.94 and incidence rates per 1000 person-years were 16 and 22.97 in Laureati et al and Noel et al, respectively. Current observational data from these 3 studies as well as data from a systematic review of case reports suggest that adverse GI events occur from days 2 to 14 after SPS administration. In addition, Noel et al noted no difference in event rate before and after the 2009 FDA recommendation to avoid coadministration with sorbitol. None of the participants in Laureati et al were exposed to sorbitol. While there are no studies specifically examining the risk of adverse events with CPS use, we expect the adverse event profile to be similar to SPS. All 3 studies had a follow-up period of 30 days following polystyrene resin exposure. Noel et al noted an increased risk in GI adverse events being detected afer 10 days and persisting during the entire follow-up period.
Secondary Outcome Data on Polystyrene Exchange Resins.

Note. GI = gastrointestinal; HD = hemodialysis; ESRD = End-stage renal disease; SPS = sodium polystyrene sulfonate; CPS = calcium polystyrene sulfonate.
These observational studies represent the best evidence to date for the effect of polystyrene resins on GI events and are the only studies that are adequately powered to study the rare adverse GI events. In summary, SPS use is associated with increased adverse GI events with an estimated hazard ratio of 1.25 to 1.94 and an incidence rate of 16 to 23 per 1000 person-years.31,40 This increased risk of rare but serious adverse GI events should be considered when prescribing polystyrene sulfonate resins.
Weight gain
Several studies have reported the effect of polystyrene resins on weight in both dialysis and nondialysis groups. Data from the DOPPS (Dialysis Outcomes and Practice Patterns Study) as analyzed by Jadoul et al suggest that there is a 250 mL increase in interdialytic weight gain in patients treated with maintenance dialysis prescribed a sodium-based potassium resin. In contrast, Nakamura et al demonstrated no change in weight in patients on hemodialysis in the SPS new start or resin change groups. Wang et al also demonstrated no change in weight with the use of CPS.
Three studies reported on the effect of resins on weight in patients not on hemodialysis (Chernin et al, Nakayama et al, and Nasir and Ahmad) report no statistically significant change in weight associated with polystyrene resin use. Nakayama et al did identify a nonstatistically significant trend to increased weight and a statistically significant association between weight and serum sodium.
Electrolyte abnormalities
Hypokalemia was reported in 7 studies. Both placebo-controlled RCTs reported hypokalemia; however, neither found that the rate was statistically different between treatment and placebo arms within the follow-up period of 6.9 days to 3 weeks.32,46 Two studies studied hypercalcemia while using CPS (Arroyo et al and Sevitt and Wrong). The follow-up time was 3 and 8.3 months, respectively. Neither reported patients who were symptomatic from hypercalcemia. The 7 patients in Arroyo et al showed an increase in serum calcium of 0.91 ± 0.46 mg/dL (0.22 ± 0.46 mmol/L) after starting CPS. The mean CPS dose was 8.93 g per day which conferred a total of 713 mg of elemental calcium daily. Of the 10 participants in the Sevitt and Wrong study, 5 patients became hypercalcemic with an average dose of elemental calcium being 1963 mg per day. However, the overall incidence of hypercalcemia has not been studied. Other studies (Tomino et al, Wang et al, Nasir and Ahmad) demonstrated no change in serum calcium with the use of CPS. Of the 6 studies that reported on serum calcium with SPS use, only Lepage et al reported a reduction in serum calcium. Three of 16 participants (18.8%) had hypocalcemia compared with placebo, which had no episodes of hypocalcemia.
Of the 9 studies that reported on serum sodium with SPS usage, 3 noted an increase in serum sodium ranging from 0.89 to 9 mEq/L (Flinn et al, 9 mEq/L; Georgianos et al, 0.89 mEq/L; Nakayama et al, 1.6 mEq/L). One case of hypernatremia was reported by Flinn et al with a serum sodium of 148 mEq/L from 143 pre-resin. Hagan et al reported 10 cases of new onset hypernatremia (2%) with a mean serum sodium of 148.5 mEq/L. A mean change in serum sodium was not provided. Out of the 3 studies that reported sodium with CPS use, there was no change in serum sodium.
Three studies (Lepage et al, Nakayama et al, and Tomino et al) reported serum magnesium levels. Lepage et al reported 5 of 16 participants (31.2%) had hypomagnesemia compared with one in the placebo group. The other 2 studies noted no change in rates of hypomagnesemia.
Electrolyte disturbances are common, and the attributability of these abnormalities to polystyrene resin use is unclear without control data. There is conflicting evidence on the association of CPS with hypercalcemia. Recent studies have identified no change or modest changes to serum calcium. Other than in the study by Lepage et al, SPS was not shown to have a statistically significant association with hypocalcemia and hypomagnesemia. Modest increases in serum sodium were observed with SPS use ranging from 0.89 to 9 mEq/L with more recent estimations being low.
Funding sources
Of the 30 included studies, 23 (77%) had no funding or conflict of interest to declare. Two studies investigating secondary outcomes disclosed funding support from pharmaceutical industry. Three studies had one author who received a research chair, an honoraria, and personal fees from pharmaceutical industry. Finally, Noel et al and Wang et al were both funded by nonindustry groups: Institute for Clinical Evaluative Sciences and Liaoning Province Translational Medicine Centre, respectively. Overall, the data included in this systematic review appear to be largely free of significant conflicts of interest. The results and conclusions do not change when studies with a funding source are excluded.
Discussion
The primary objective of this systematic review was to identify the currently available evidence for the efficacy and safety of polystyrene exchange resins in adults with hyperkalemia. To our knowledge, this study is the first systematic review to include and assess RCTs, observational data, and nonrandomized interventional studies. Previous systematic reviews investigating efficacy have previously only included RCTs, of which there are few studies.7,8,23 Previous reviews on the safety profile of polystyrene resins have focused on the adverse GI events and examined the case series and case report literature. This review builds on that knowledge by including data regarding the safety profile of polystyrene resins from large observational studies and by including additional safety endpoints.
This systematic review identified several themes as outlined in the following sections.
Key Point 1: Highly Variable Timeline Studied—Poor Evidence for Use in Acute Hyperkalemia
The majority and highest quality evidence for the use of polystyrene resins is for periods of time greater than 24 hours. Ten studies investigated the effects of single-dose polystyrene resins within 24 hours, none of which are RCTs. While all studies reported a reduction in serum potassium, these studies were subject to significant confounders. The variable timelines studied likely reflect the ongoing uncertainty of the role of SPS/CPS in acute and chronic hyperkalemia—terms that are not well-defined in the literature. In contrast, 12 studies investigated the role of polystyrene resins beyond 24 hours. Ten of 12 demonstrated a reduction of greater than 0.5 mEq/L. However, only 1 of 3 low-risk studies demonstrated this reduction when compared with a matched control or placebo group. This difference in serum potassium reduction may be a result of the comparatively high dose of resin used in the study conducted by Lepage et al when compared with Wang et al and Batterink et al. While the paucity of high-quality evidence does not exclude the possibility of benefit, it is important to note that the use of potassium resins in acute hyperkalemia is not robustly supported by the evidence. The use in chronic hyperkalemia is somewhat mixed and may depend on the dose of resin provided.
Key Point 2: Patient-Centered Outcomes Such as Recurrence of Hyperkalemia and Mortality are Under-Studied
This study reviews the data available for the potassium-lowering effects of polystyrene resins. This endpoint, however, does not necessarily represent patient-important outcomes. Several studies have demonstrated that chronic hyperkalemia is well tolerated in patients with CKD and that mortality from hyperkalemia is highest in those with normal or lower grade CKD.3-6 Furthermore, data from Rossignol et al suggest that the use of polystyrene resins does not prevent recurrence of hyperkalemia at a population level. 41 At the present time, it remains unclear whether the use of polystyrene resins produces an effect on patient-centered outcomes including hospitalization, morbidity, and mortality; this is especially relevant in the setting of chronic use.
Key Point 3: Safety Profile—Interdialytic Weight Gain and Electrolyte Disturbances Have Limited Data
Within the current body of literature, complications of polystyrene use included interdialytic weight gain in SPS, hypercalcemia in CPS, and adverse GI events. Recent literature has provided data on the adverse GI events; however, the other adverse effect profiles of these medications remain poorly studied. Specifically, interdialytic weight gain and electrolyte disturbances including hypercalcemia are potential adverse effects that have been minimally studied.
Strengths/Limitations
The present review is the first systematic review of the current literature on polystyrene sulfonate resins in hyperkalemia that closely examines RCT data, observational, and nonrandomized experimental study data. This study included both commonly available preparations of SPS and CPS. In contrast, a previous review included 18 studies on SPS and CPS and previous Cochrane reviews have only included at most one RCT.7,8,23
We acknowledge several limitations in this study. Case studies and case series were excluded from the search results. Large case series may have been excluded despite having comparable sample sizes to studies included due to lack of a comparator and calculated estimates. Due to the heterogeneity of the studies, the data were unable to be meta-analyzed and as such the potassium-lowering effect of polystyrene sulfonate resins remains founded on small studies with potential confounders. As with any review the validity of the results is limited by publication bias. We were not able to quantify this given study heterogeneity. However, there was adequate dispersion of sample sizes and estimates that we capture in our review that would minimize such bias.
Conclusions
The current literature suggests that polystyrene sulfonate resins may have a modest effect on lowering potassium in the setting of hyperkalemia. The magnitude of effect remains unclear as most of the available evidence is at high risk of bias. The best evidence for its use is for longer term treatment of hyperkalemia, typically greater than 72 hours and with multiple doses of resin. It remains unclear whether there is a role for polystyrene resins in the acute management of hyperkalemia. The most well-recognized complication of polystyrene sulfonate use are adverse GI events including ischemia with an estimated hazard ratio between 1.25 and 1.94 and incidence rates per 1000 person-years between 16 and 22.97. The adverse effect profile has not yet been clearly elucidated; however, current evidence suggests that hypercalcemia, hypernatremia, and hypomagnesemia may not be clinically relevant adverse outcomes with polystyrene resin use. There also remains little evidence on the effect of polystyrene sulfonate resins on patient-important outcomes such as hospitalization, morbidity, and mortality. Future research should be directed at determining the magnitude of effect of polystyrene resin use compared with placebo in both acute and chronic hyperkalemia with a focus on patient-important outcomes.
Supplemental Material
CJK-Supplemental_material – Supplemental material for Polysulfonate Resins in Hyperkalemia: A Systematic Review
Supplemental material, CJK-Supplemental_material for Polysulfonate Resins in Hyperkalemia: A Systematic Review by Sheung Wing Sherwin Wong, Grace Zhang, Patrick Norman, Hasitha Welihinda and Don Thiwanka Wijeratne in Canadian Journal of Kidney Health and Disease
Footnotes
List of Abbreviations
SPS, sodium polystyrene sulfonate; CPS, calcium polystyrene sulfonate; RCT, randomized control trial; CKD, chronic kidney disease; CrCl, creatinine clearance; eGFR, estimated glomerular filtration rate; GI, gastrointestinal.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
All authors consented to the publication of this manuscript.
Availability of Data and Materials
All data is presented in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.