
Abstract
Background:
Approximately 10% of emergency department (ED) visits among dialysis patients are for conditions that could potentially be managed in outpatient settings, such as hyperkalemia.
Objective:
Using population-based data, we derived and internally validated a risk score to identify hemodialysis patients at increased risk of hyperkalemia-related ED events.
Design:
Retrospective cohort study.
Setting:
Ten in-center hemodialysis sites in southern Alberta, Canada.
Patients:
All maintenance hemodialysis patients (≥18 years) between March 2009 and March 2017.
Measurements:
Predictors of hyperkalemia-related ED events included patient demographics, comorbidities, health-system use, laboratory measurements, and dialysis information. The outcome of interest (hyperkalemia-related ED events) was defined by International Classification of Diseases (10th Revision; ICD-10) codes and/or serum potassium [K+] ≥6 mmol/L.
Methods:
Bootstrapped logistic regression was used to derive and internally validate a model of important predictors of hyperkalemia-related ED events. A point system was created based on regression coefficients. Model discrimination was assessed by an optimism-adjusted C-statistic and calibration by deciles of risk and calibration slope.
Results:
Of the 1533 maintenance hemodialysis patients in our cohort, 331 (21.6%) presented to the ED with 615 hyperkalemia-related ED events. A 9-point scale for risk of a hyperkalemia-related ED event was created with points assigned to 5 strong predictors based on their regression coefficients: ≥1 laboratory measurement of serum K+ ≥6 mmol/L in the prior 6 months (3 points); ≥1 Hemoglobin A1C [HbA1C] measurement ≥8% in the prior 12 months (1 point); mean ultrafiltration of ≥10 mL/kg/h over the preceding 2 weeks (2 points); ≥25 hours of cumulative time dialyzing over the preceding 2 weeks (1 point); and dialysis vintage of ≥2 years (2 points). Model discrimination (C-statistic: 0.75) and calibration were good.
Limitations:
Measures related to health behaviors, social determinants of health, and residual kidney function were not available for inclusion as potential predictors.
Conclusions:
While this tool requires external validation, it may help identify high-risk patients and allow for preventative strategies to avoid unnecessary ED visits and improve patient quality of life.
Trial registration:
Not applicable—observational study design.
What was known before
Emergency department (ED) use is high among hemodialysis patients.
Approximately 10% of ED encounters among hemodialysis patients are for conditions that could potentially be managed in outpatient settings, such as hyperkalemia.
What this adds
We derived and validated a clinical risk prediction tool to identify hemodialysis patients at increased risk of hyperkalemia-related ED events.
This prediction tool has good discrimination and calibration and includes 5 strong predictors of hyperkalemia-related ED events: ≥1 laboratory measurement of serum K+ ≥6 mmol/L in the prior 6 months; ≥1 Hemoglobin A1C [HbA1C] measurement ≥8% in the prior 12 months; Mean ultrafiltration of ≥10 mL/kg/h over the preceding 2 weeks; ≥25 hours of cumulative time dialyzing over the preceding 2 weeks; Dialysis vintage of ≥2 years.
Introduction
Health care use is high among patients with chronic kidney disease (CKD), often related to their medical complexity.1-7 Multi-morbidity is common, and as a result, the use of acute care services is high—particularly among dialysis-dependent patients.8-13 On average, dialysis-dependent patients are hospitalized at least once per year, and 1 in 3 will be readmitted to hospital within 30 days. 6 Emergency department (ED) use is also high among this patient population.3,7 Recent work by our team found that dialysis-dependent patients present to the ED upward of 2 to 3 times per year. 7
Dialysis patients frequently present to the ED with access-related infections, dyspnea (as a result of fluid overload or other pathologies), chest and abdominal pain, acid/base and electrolyte imbalances, and hypotension.12,14,15 In a population-based analysis of ED use among dialysis patients, we found that approximately 10% of all ED encounters were for conditions that could have been managed or cared for in an outpatient setting—and were thus potentially preventable. 7 One of the most common ambulatory care–sensitive conditions16,17 with which dialysis-dependent patients present to the ED is hyperkalemia, a potentially life-threatening condition associated with increased risk of arrhythmia and cardiac mortality. 18
While the ED is essential for providing urgent care in a timely manner, identifying ways to improve efficiency and decrease ED use has been recognized as a national research priority.19-21 Given the patient and health-system burden associated with dialysis, and the high rate of potentially preventable ED encounters (such as hyperkalemia), tools that highlight patients at risk of ED visits could allow for appropriate preemptive interventions. Currently, there is no standardized system to identify patients at high risk of adverse events who may require additional clinical attention and care. With this in mind, we used population-based data from Alberta, Canada to derive and internally validate a clinically useful prediction tool to identify hemodialysis patients at increased risk of hyperkalemia-related ED events.
Methods
This study complies with the reporting standards outlined in the Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) statement 22 (Supplementary Table S1) and was approved by the University of Calgary Conjoint Health Research Ethics Board.
Study Cohort
We identified all maintenance hemodialysis patients (≥18 years) from March 2009 to March 2017 in southern Alberta, Canada. Individuals were eligible for inclusion in the cohort based on availability of electronic dialysis session-level data, recorded in the Patient-based Renal Information System (PARIS) which was implemented across 10 in-center hemodialysis sites in the Southern Alberta Renal Program (SARP) between March 2009 and November 2016. 23 Within this database, detailed records of each dialysis session (electronic run sheets) for an individual were available (described below). To ensure maintenance dialysis status, we excluded patients with less than 90 days of dialysis information as well as dialysis sessions during and 4 weeks after an inpatient admission. Outcome status and potential candidate variables for the prediction tool were established by linking this cohort (via provincial health care number) to the administrative and clinical data holdings of the Alberta Kidney Disease Network, which include demographic, laboratory, comorbidity information, and records of health-system use, 24 as well as dialysis vintage and modality history in the PARIS database.
Study Design and Outcome Ascertainment
Within our cohort of patients, we identified differences between patients with and without hyperkalemia-related ED events. The study outcome was a hyperkalemia-related ED encounter, as defined by either an International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Canada (ICD-10-CA) code (E87.5) or a serum potassium (K+) measurement ≥6.0 mmol/L on the day before or day of presentation to the ED. To allow for a sufficient period to establish predictors of the outcome, the earliest eligible outcome date was 28 days after dialysis initiation or electronic run sheet data availability. For all individuals without an outcome, we assigned a random date within each persons’ period on hemodialysis to serve as an equivalent to an outcome date. Therefore, time preceding hyperkalemia-related ED events could be compared to equivalent time periods that did not end with an ED event. This aided the identification of differences between patients with and without hyperkalemia-related ED events. We predicted 2-week risk of the outcome to allow sufficient time for nephrologists to alter treatment in an effort to avoid subsequent outcome events.
Selection of Candidate Predictor Variables
Available health-system data including hospital discharge abstracts, physician claims, and ambulatory care records were used to derive measures of health-system use and comorbidity. We obtained demographic information from population health registry files linked with neighborhood-level Canadian Census data. Provincial laboratory data provided measures of serum K+, serum phosphate, and hemoglobin A1C (HbA1C). Dialysis session information included date and location of each session, dialysis access type, pre-run intentions (eg, ultrafiltration rate goal, target weight, K+ dialysate concentration), in-session information including duration, reporting of various symptoms (diarrhea, edema, fever, nausea, etc), intradialytic hypotension events (a drop of ≥20 mmHg from baseline), as well as summary measures of online urea clearance and ultrafiltration rate. Pre- and post-session physical measurements (weight, blood pressure, heart rate, mobility) provided evidence of state change due to dialysis. From the list of all available variables, we selected candidate predictor variables for further analysis based on clinical expertise and likelihood of being readily accessible within hemodialysis units. Dialysis predictors were defined at, or up to, an ascertainment date 14 days prior to the outcome date (eg, a predictor recorded in “the prior 2 weeks” was measured 14-28 days prior to the outcome), while laboratory values were defined at clinically relevant intervals, based on nephrologist consultation and standard test ordering schedules. If a measurement was not available during the ascertainment window, it was treated as missing for modeling purposes.
Model Development
We described and compared potential predictors by outcome status using Chi-square, t tests, or Kruskal-Wallis tests as appropriate. Univariate logistic regression was also used to further refine the list of potential predictors that could reasonably be implicated in the outcome. We then developed a multivariable model using these predictors. We used the full cohort for model derivation and internal validation, using the bootstrapping sample use-reuse method to estimate and adjust for overfitting and optimism inherent to this approach. 25 Variables were removed from the model via backwards elimination, based on a strategy of sequentially eliminating the weakest predictor as specified by the Wald test P value, while ensuring that each deleted variable also lowered the Akaike Information Criterion (AIC) of the model. A parsimonious model with minimized AIC was considered the final model. We used robust standard errors to account for potential clustering of hyperkalemia events per patient.
Model performance was assessed using measures of discrimination and calibration. Discrimination was assessed numerically using the C-statistic (also referred to as area under the receiver operating characteristic [ROC] curve). Initially, the apparent discrimination of the final multivariable model was calculated. The model derivation process was repeated with 1000 bootstrapped samples, and the bootstrapped model coefficients were averaged and compared to coefficients from the original dataset to obtain estimates of optimism. These were then used to adjust model performance measures, as described by Harrell et al. 25 An ROC curve was plotted for graphical assessment of discrimination. Model calibration was assessed statistically using the Hosmer-Lemeshow goodness-of-fit test and graphically by plotting observed versus predicted deciles of risk, in addition to a calibration slope to visually represent the overfitting/underfitting of the model.
Generation of a Point System
We created a point system based on the method described for the Framingham Score. 26 To assign point scores, the lowest coefficient value within the final regression model was assigned one point, and the ratio of every other coefficient in the model to that coefficient was rounded to the nearest integer to obtain an equivalent point score for that coefficient. Summing the points assigned to categories of each predictor (when present within a patient) allowed for the calculation of a total point score, which was approximately linearly related to the risk of the outcome predicted by the model. All described analyses were completed using Stata version 14 (StataCorp LP), and P values <.05 were considered to be statistically significant.
Results
Patient Characteristics
Our study included 1533 maintenance hemodialysis patients, each of whom had a period of dialysis treatment spanning at least 90 days, as recorded in the PARIS database (Figure 1). Of these, 331 (21.6%) had 615 hyperkalemia-related ED events (197 defined by both ICD-10-CA code and serum K+ measure, 65 by ICD-10-CA code alone, and 353 by serum K+ measure alone). The 331 individuals had a median follow-up time of 2.1 years (interquartile range [IQR]: 1.3-3.4 years), and a rate of 1.83 hyperkalemia events per 1000 patient days. Table 1 shows the demographic and clinical characteristics of the overall study cohort, stratified by outcome status. Mean age of the cohort was 64.0 years (standard deviation [SD]: 15.5), with no significant difference between those with and without the outcome of interest. Those with hyperkalemia-related ED events had more comorbidity than those without (median [IQR]: 5 conditions [4, 7] vs 4 conditions [3, 6], P < .001). Those with hyperkalemia were also more likely to have at least one HbA1C measure ≥8% in the previous 12 months (29.6% vs 21.6%, P = .01) and to have at least one serum K+ measure ≥6 mmol/L in the 6 months prior to the ED event, not including measures recorded during the event itself (46.8% vs 21.1%, P < .001). The dialysis delivered to the patients with an ED encounter for hyperkalemia in the month prior to the outcome event differed from those who did not have the outcome, with a lower dialysate K+ concentration (26.3% ≤2.0 mmol/L vs 18.4%, P = .002), higher average ultrafiltration rate (47.9% ≥10 mL/kg/h vs 30.4%, P < .001), and more dialysis time (39.0% ≥25 hours in 2 weeks vs 22.1%, P < .001) among those with a hyperkalemia ED event.

Study cohort formation.
Demographic, Clinical, and Dialysis Characteristics of Study Cohort.

Note. All P values calculated are by Chi-square test except †t test and ‡Kruskal-Wallis. COPD = chronic obstructive pulmonary disease; PCP = primary care provider.
2-year primary care provider attachment refers to the percentage of all primary care encounters that were made to the most visited primary care provider, among those with at least 3 visits.
Predictors of a Hyperkalemia-Related ED Event
The univariate analysis for candidate predictors is reported in Supplementary Table S2. The final multivariable model for hyperkalemia-related ED events included 5 predictors totaling 9 points: ≥1 HbA1C measurement ≥8% in the prior 12 months (1 point); ≥25 hours of cumulative time dialyzing over the preceding 2 weeks (1 point); a mean ultrafiltration rate of ≥10 mL/kg/h over the preceding 2 weeks (2 points); dialysis vintage of ≥2 years (2 points) and ≥1 laboratory measurement of serum K+ ≥6 mmol/L in the prior 6 months (3 points) (Figure 2).
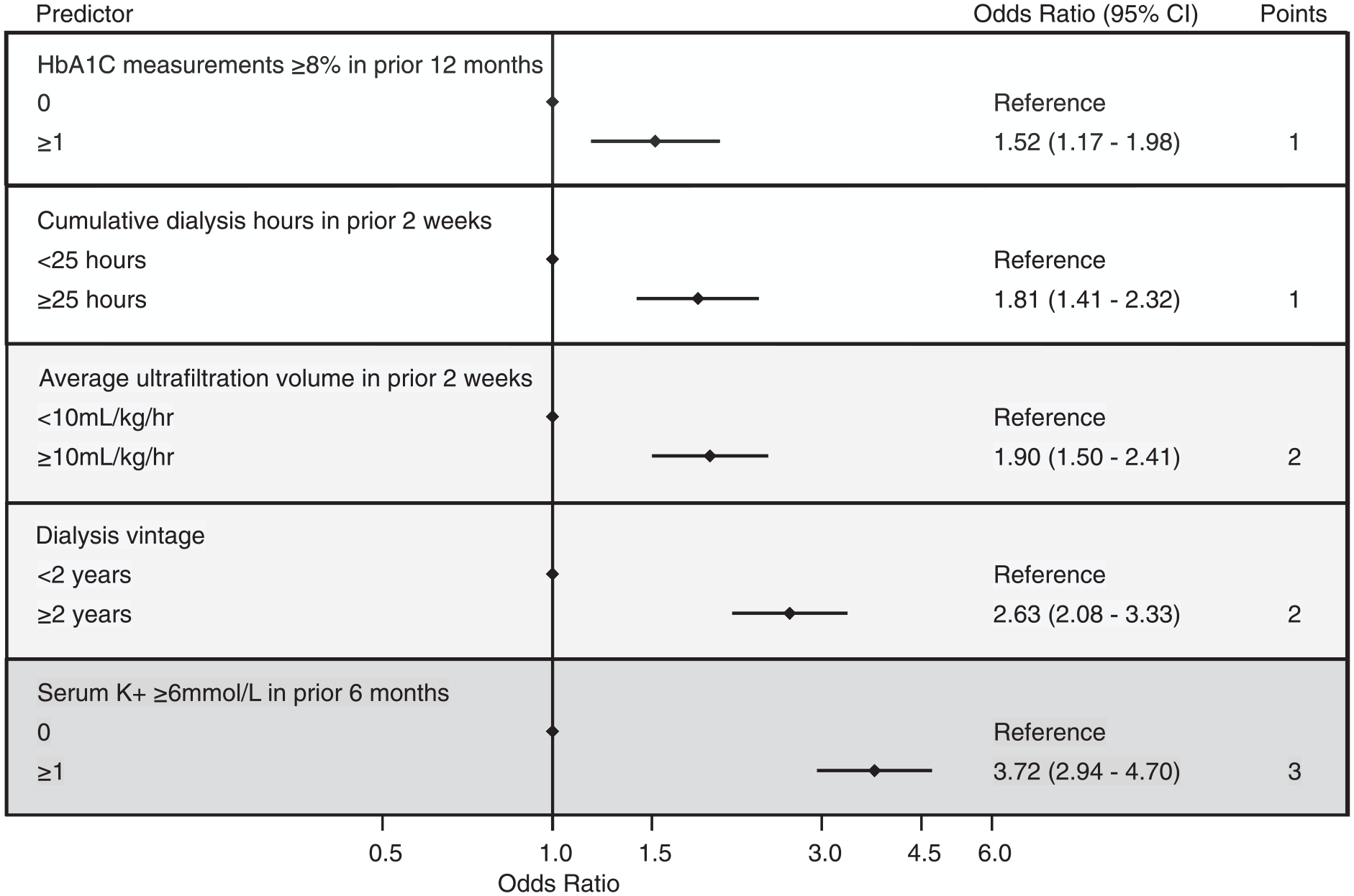
Forest plot of independent predictors of an emergency department encounter for hyperkalemia with corresponding point scores.
The apparent C-statistic in the full cohort was 0.76. Following bootstrapping to estimate model overfitting and optimism, the optimism-adjusted C-statistic was 0.75, representing reasonable model discrimination (Figure 3). Graphical presentation of the observed versus expected risk of hyperkalemia-related ED events for each decile of risk (Figure 4) showed near-equivalence for all deciles (Hosmer-Lemeshow P = .097), indicating good calibration. This was corroborated by the calibration slope that closely mirrors the 45° identity line, with intercept 0.00 (95% confidence interval [CI]: −0.04 to 0.04) and slope 0.99 (95% CI: 0.89 to 1.10), each indicating no significant deviation (Supplementary Figure S1).
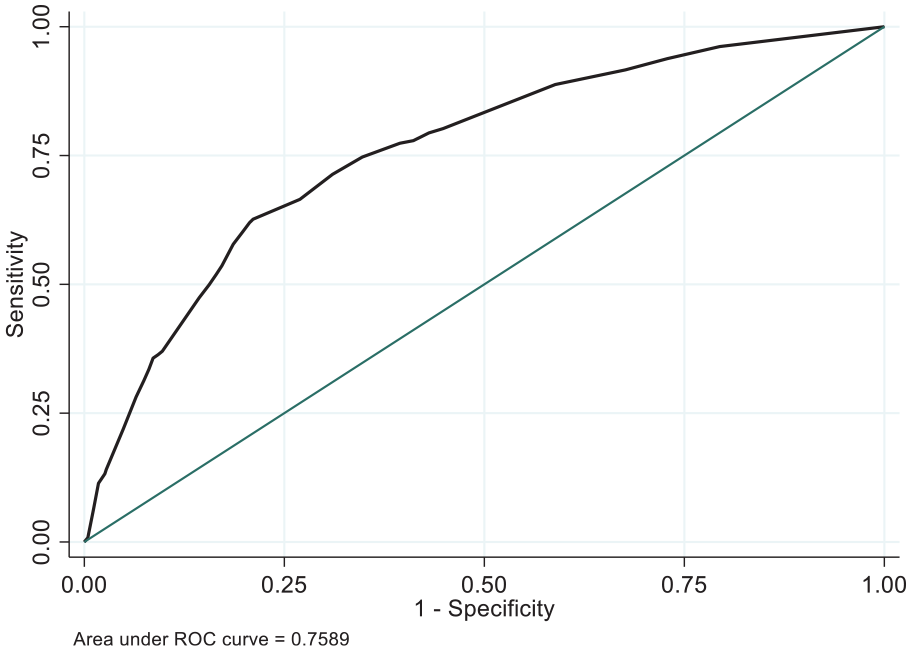
ROC curve for the multivariable model estimating the risk of an emergency department encounter for hyperkalemia.
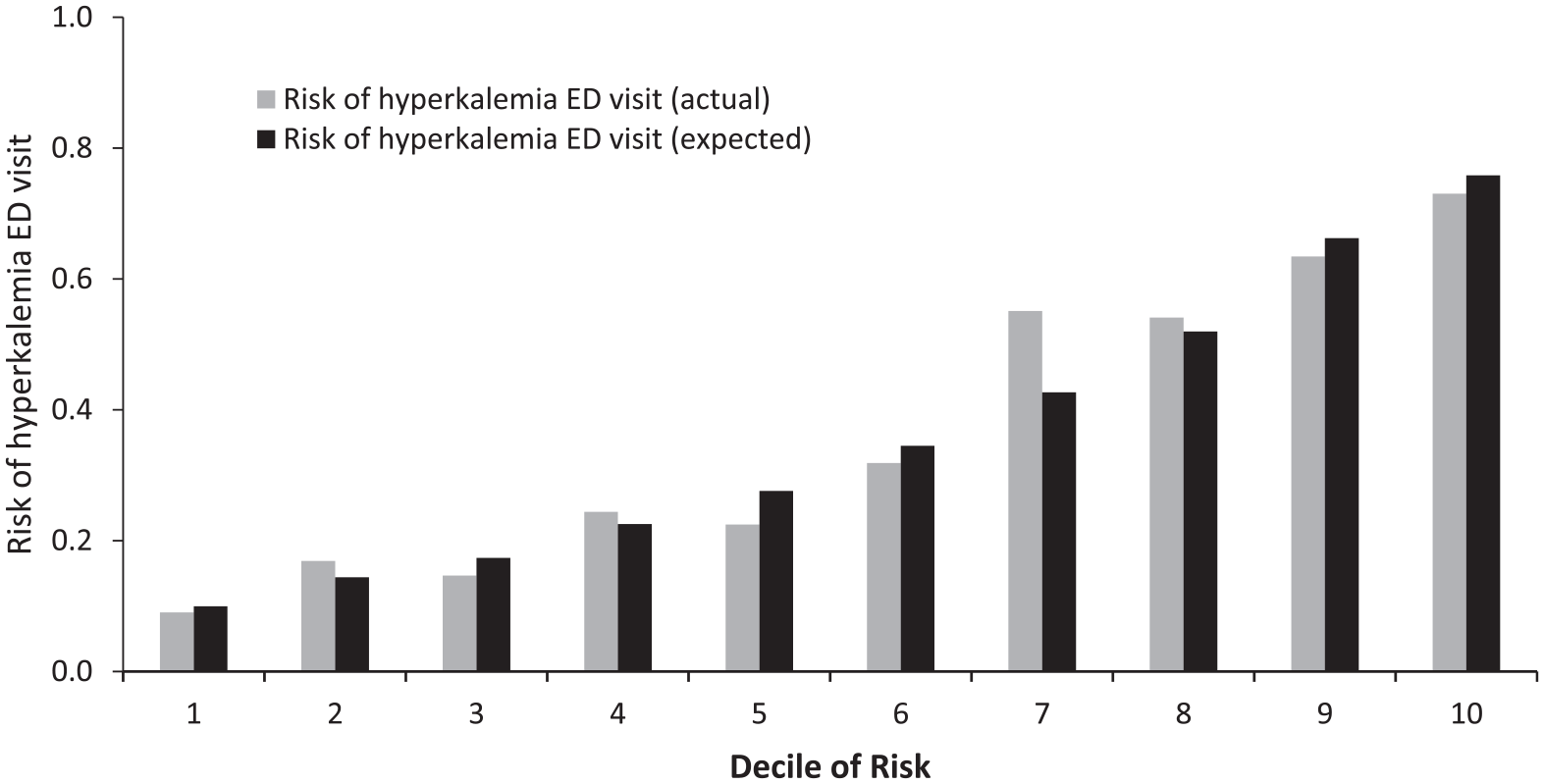
Deciles of actual versus expected risk for the multivariable model estimating the risk of an ED encounter for hyperkalemia (Hosmer-Lemeshow P value = .097).
Using the coefficient for ≥1 HbA1C measurement ≥8% in the prior 12 months as the basis of 1 point, the remaining coefficients were converted to an integer based on relative magnitude, creating a 9-point scale. A score of ≤2 equated to approximately 20% of individuals experiencing a hyperkalemia-related ED event in the following 2 weeks, while a score ≥6 represented at least 60% of individuals having an event (Figure 5). As scores increased, the percentage of individuals at each point total who experienced the outcome, and who were predicted to experience the outcome, also increased.
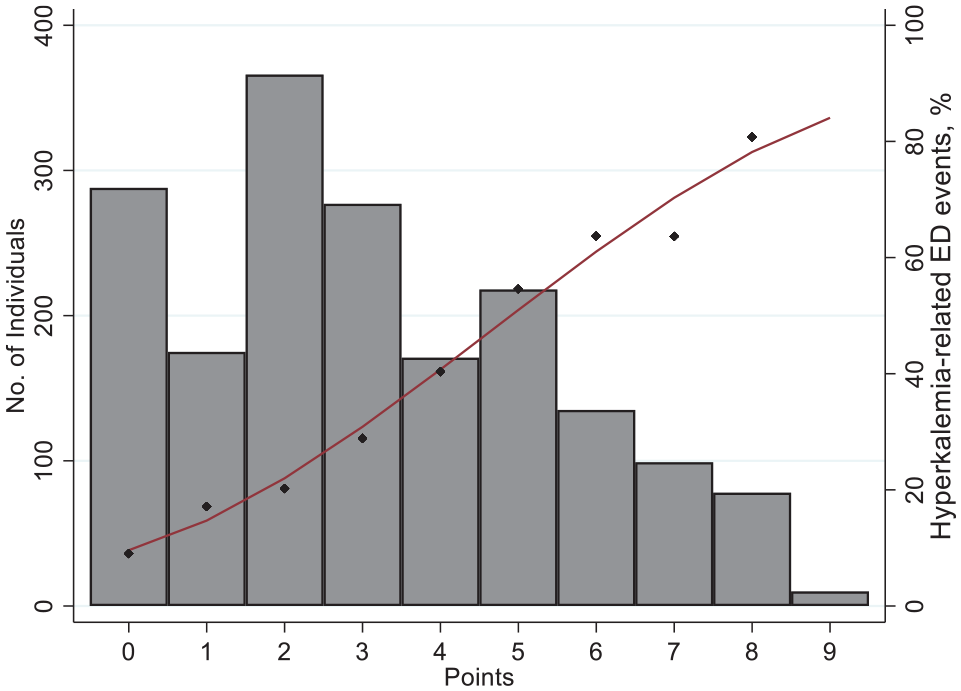
Number of individuals associated with each point score (primary axis, presented as bars) and percentage of individuals who had the outcome (diamonds) or were predicted to have the outcome (logistic function line) at each point score (secondary axis).
Discussion
Using a large population–based cohort of maintenance hemodialysis patients, we developed and internally validated a risk score to identify patients at greatest risk for a hyperkalemia-related ED encounter. The final model contained 5 predictors readily available from hemodialysis care and had good discrimination and calibration. To facilitate clinical use, a scoring system was created with each of the 5 predictors assigned a point value proportional to its level of risk. Following external validation, our tool has the potential to identify hemodialysis patients at highest risk of presenting to the ED for a condition that is potentially preventable. Combining this tool with preventive strategies may improve patient quality of life and reduce the strain currently placed on EDs by hemodialysis patients.
Prior studies have explored clinical and demographic factors associated with health care encounters for hyperkalemia,27-29 while others have examined the health outcomes (particularly mortality) among hemodialysis patients with elevated serum potassium levels.30-32 To our knowledge, this is the first multivariable prediction model that has been derived and internally validated to identify maintenance hemodialysis patients at increased risk for hyperkalemia-related ED encounters.
The predictors included in our prediction model have face validity and most are commonly cited characteristics associated with adverse outcomes (including hyperkalemia) among hemodialysis patients. Prior research has shown that patients with diabetes are at an increased risk for hyperkalemia for numerous reasons.33,34 For example, hyporeninemic hypoaldosteronism in the setting of diabetic kidney disease can contribute to hyperkalemia, and these patients are also more likely to receive angiotensin blockade for hypertension and proteinuria. 35 Furthermore, diabetics with HbA1C values ≥8% in the prior year could be correlated with poor adherence both with diabetic control and with dietary choice. While the accuracy of HbA1C measurements among end-stage kidney disease patients may be variable due to changes in hemoglobin characteristics and red blood cell turnover in the setting of erythropoietin therapy, any misclassification that is likely to occur would be non-differential and thus would not impact our overall study results. 36 In previous literature, prior laboratory values for elevated serum potassium (K+ ≥6 mmol/L) have also been shown to be a strong predictor of recurrent ED encounters for hyperkalemia. 27
Cumulative hours of dialysis in the prior 2 weeks and an average ultrafiltration rate ≥10 mL/kg/h were also significant predictors of ED encounters for hyperkalemia. Longer dialysis hours may be capturing an appropriate clinical response to treat patients with persistently elevated potassium, chronic volume overload, or uremic complications. Prior research has shown that non-adherence with dialysis and fluids accounts for a substantial proportion of hyperkalemia-related hospitalizations,18,37 and thus, it is not surprising to see that a high ultrafiltration rate is associated with hyperkalemia. The potential non-adherence to fluid restrictions, as suggested by the high ultrafiltration rate, may be correlated with adherence to dietary potassium restrictions as well.
An independent predictor that was of particular interest within our multivariable model was dialysis vintage. With prolonged exposure to dialysis, there is potential for loss of residual kidney function and urine output. This may eliminate the observed survival and fluid management benefits associated with residual kidney function in dialysis patients and contribute to reduced potassium excretion and thus increase a patients’ risk for hyperkalemia. 38 However, further work is required to determine if vintage is truly an independent risk factor for hyperkalemia or a proxy measure for loss of residual kidney function.
There are a number of strengths of this study including its methodological rigor and adherence to TRIPOD guidelines to ensure accuracy, consistency, and transparency of the reported results. Our study was also conducted using population-based data which minimize selection bias and would lead to greater external validity. Furthermore, the 5 predictors included in the model all had fairly large effect sizes and represent clinical variables that are routinely collected or evaluated by multidisciplinary dialysis teams in dialysis units (eg, laboratory values, dialysis prescription, and vintage). The point score version (out of 9) is also very simple to use and unlike many prediction tools, does not require additional expensive or time-consuming tests. Once externally validated, the risk prediction score or the risk prediction model itself could be implemented into existing electronic medical records/clinical information systems and automated to dynamically generate an individual’s probability of attending the ED for a hyperkalemia-related event when new laboratory values are received or changes to a dialysis prescription are made. Those at greatest risk could prompt consultation with a dietician, evaluation of the current dialysis prescription, or other strategies to prevent future ED presentation.
However, these findings should be interpreted in light of the study limitations. First, this tool was derived using retrospective secondary data. As such, predictor variables were selected based on the available data from administrative data sources rather than selection of predictors most desirable to develop the prediction model. For example, we were unable to include variables related to health behaviors or social determinants of health that may affect a patient’s adherence to recommended care plans. Contribution of residual kidney function could also not be directly measured and may confound the observed relationships between our identified predictors and outcome. Furthermore, we did not assess prescription medications that are associated with an increased risk for hyperkalemia (namely angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, potassium-sparing diuretics [spironolactone or eplerenone], or potassium supplements). While inclusion of these additional variables may improve model discrimination, we believe our linked data sources contained an array of important clinical, demographic, and dialysis-specific variables to consider in the modeling process. It is therefore unlikely that we have missed a strong predictor of the outcome that would have resulted in an appreciable increase in model performance. Second, it is possible that variation in clinical practice and laboratory measurements in other settings could influence model performance. However, the use of population-level data combined with analytical adjustment to address optimism increases the likelihood that this tool will be externally valid. Despite this, we recognize the need for external validation of this prediction tool in other jurisdictions and a greater understanding of how this tool would be used in a clinical setting prior to implementation.
Conclusions
In summary, we derived and internally validated a clinical risk prediction tool to identify maintenance hemodialysis patients at greatest risk of an ED encounter for hyperkalemia. The 5 variables that were identified in our multivariable model are routinely collected laboratory and dialysis-specific information suggesting this model could easily be implemented in other clinical settings. While the measures of model performance and internal validation are promising, there is a need for external validation and testing prior to its clinical application. Combined with preventive care strategies, this tool has the potential to avoid unnecessary use of acute care services while improving patient quality of life.
Supplemental Material
CJKHD_Supplemental_Material_-_Appendix_1-3_Revised_Clean_Copy_-_June_29_2020_1 – Supplemental material for Derivation and Internal Validation of a Clinical Risk Prediction Tool for Hyperkalemia-Related Emergency Department Encounters Among Hemodialysis Patients
Supplemental material, CJKHD_Supplemental_Material_-_Appendix_1-3_Revised_Clean_Copy_-_June_29_2020_1 for Derivation and Internal Validation of a Clinical Risk Prediction Tool for Hyperkalemia-Related Emergency Department Encounters Among Hemodialysis Patients by Paul E. Ronksley, James P. Wick, Meghan J. Elliott, Robert G. Weaver, Brenda R. Hemmelgarn, Andrew McRae, Matthew T. James, Tyrone G. Harrison and Jennifer M. MacRae in Canadian Journal of Kidney Health and Disease
Footnotes
Ethics Approval and Consent to Participate
This study was approved by the University of Calgary Conjoint Health Research Ethics Board and granted a waiver of participant consent.
Consent for Publication
All authors consented to the publication of this manuscript.
Availability of Data and Material
This study is in part on the basis of data provided by Alberta Health and Alberta Health Services. The interpretation and conclusions are those of the researchers and do not represent the views of the Government of Alberta. Neither the Government of Alberta nor Alberta Health express any opinion in relation to this study. Dr. Paul Ronksley had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. We are not able to make our data set available to other researchers due to our contractual arrangements with the provincial health ministry (Alberta Health), who is the data custodian. Researchers may make requests to obtain a similar data set at ![]() .
.
Author Contributions
P.E.R. was involved in the conception and design of the study. He was also responsible for drafting the manuscript and interpreting the data. J.P.W. and R.G.W. contributed to the study design and conducted the analysis. M.J.E., B.R.H., M.J.E., T.G.H., A.M., and J.M.M. contributed to the conception and interpretation of study findings. All authors were responsible for revising the manuscript critically for important intellectual content, approved the final version, and agreed to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by a Biomedical Research Grant from the Kidney Foundation of Canada (KFOC). M.J.E. is supported by a Kidney Research Scientist Core Education and National Training (KRESCENT) New Investigator Award. B.R.H. is supported by the Roy and Vi Baay Chair in Kidney Research. M.T.J. is supported by a Foundation Award from the Canadian Institutes of Health Research (CIHR). The Interdisciplinary Chronic Disease Collaboration is funded by the AIHS-Collaborative Research and Innovation Team Grant Program. T.G.H. is supported by a KRESCENT postdoctoral fellowship (co-sponsored by the KFOC and CIHR) and the Clinician Investigator Program at the University of Calgary.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.