
Abstract
Purpose:
To collate best practice recommendations on the management of patients receiving in-center hemodialysis during the COVID-19 pandemic, based on published reports and current public health advice, while considering ethical principles and the unique circumstances of Canadian hemodialysis units across the country.
Sources of information:
The workgroup members used Internet search engines to retrieve documents from provincial and local hemodialysis programs; provincial public health agencies; the Centers for Disease Control and Prevention; webinars and slides from other kidney agencies; and nonreviewed preprints. PubMed was used to search for peer-reviewed published articles. Informal input was sought from knowledge users during a webinar.
Methods:
Challenges in the care of hemodialysis patients during the COVID-19 pandemic were highlighted within the Canadian Senior Renal Leaders Forum discussion group. The Canadian Society of Nephrology (CSN) developed the COVID-19 rapid response team (RRT) to address these challenges. They identified a pan-Canadian team of clinicians and administrators with expertise in hemodialysis to form the workgroup. One lead was chosen who drafted the initial document. Members of the workgroup reviewed and discussed all recommendations in detail during 2 virtual meetings on April 7 and April 9. Disagreements were resolved by consensus. The document was reviewed by the CSN COVID-19 RRT, an ethicist, an infection control expert, a community nephrologist, and a patient partner. Content was presented during an interactive webinar on April 11, 2020 attended by 269 kidney health professionals, and the webinar and first draft of the document were posted online. Final revisions were made based on feedback received until April 13, 2020. CJKHD editors reviewed the parallel process peer review and edited the manuscript for clarity.
Key findings:
Recommendations were made under the following themes: (1) Identification of patients with COVID-19 in the dialysis unit, (2) hemodialysis of patients with confirmed COVID-19, (3) hemodialysis of patients not yet known to have COVID-19, (4) visitors; (5) testing for COVID-19 in the dialysis unit; (6) resuscitation, (6) routine hemodialysis care, (7) hemodialysis care under fixed dialysis resources.
Limitations:
Because of limitations of time and resources, and the large number of questions, formal systematic review was not undertaken. The recommendations are based on expert opinion and subject to bias. The parallel review process that was created may not be as robust as the standard peer review process.
Implications:
We hope that these recommendations provide guidance for dialysis unit directors, clinicians, and administrators on how to limit risk from infection and adverse outcomes, while providing necessary dialysis care in a setting of finite resources. We also identify a number of resource allocation priorities, which we hope will inform decisions at provincial funding agencies.
Purpose
Patients receiving in-center hemodialysis are a unique and vulnerable population during a pandemic. The necessity for treatment at the dialysis center 3 times weekly means they cannot remain isolated in their homes. They must interact regularly with drivers, nurses, and members of the health care team. Most Canadian hemodialysis units are built with limited (if any) isolation rooms, and many units are too small to strictly observe the minimum 2 m distance between patients at all times in the waiting room and treatment areas. These circumstances pose the perfect environment for the rapid spread of COVID-19 infection. If infected, patients managed with maintenance dialysis have high risk of death because of their high burden of comorbid disease or advanced age. 1 Adequate implementation of measures to prevent the spread of COVID-19 in center hemodialysis units is therefore of paramount importance.
While provincial and federal public health agencies provide recommendations with respect to infection control practices on a daily basis, most of these recommendations, including those from the Centers of Disease Control, 2 provide minimal concrete and specific guidance on how to manage in-center hemodialysis units during the pandemic. Furthermore, advice from other countries is not necessarily applicable to the Canadian landscape.3-7
We convened a national workgroup of dialysis leaders to discuss key issues in the management of patients receiving in-center hemodialysis during the COVID-19 pandemic, 8 to collate concrete recommendations that can be easily translated into practice within the resource constraints of individual programs in Canada. We also sought to identify gaps in processes in care that were of high priority and common throughout the country so that these can be prioritized for resource allocation by provincial funding agencies.
Information Sources
The workgroup members used Internet search engines to retrieve documents from provincial and local hemodialysis programs,9-13 provincial public health agencies,14-19 the Centers for Disease Control and Prevention, 2 other kidney agencies, 20 as well as nonreviewed preprints. Finally, we searched PubMed for relevant peer-reviewed published articles using the search terms “COVID-19” AND “(dialysis OR chronic kidney disease).”
Methods
In the context of the pandemic, regional hemodialysis programs rapidly developed policy. Challenges in care were highlighted in the discussion group of the Canadian Senior Renal Leaders Forum, a group of medical and administrative leaders of kidney programs. The Canadian Society of Nephrology (CSN) developed the COVID-19 rapid response team (RRT) to address these challenges by recruiting volunteers within the CSN board who then identified other experts within the kidney community to form the workgroup. Available COVID-19 documents from programs across the country were collected. Other national and international kidney agency literature and webinars were viewed for recommendations that could be applied to the Canadian environment. In select circumstances, a review of the published literature was also undertaken. One lead was chosen who drafted the initial document. Members of the workgroup reviewed and discussed all recommendations in detail during 2 virtual meetings on April 7, 2020 and April 9, 2020. Disagreements were resolved by consensus. Recommendations were developed based on consideration of several principles based on ethical underpinnings. We use “we recommend” when we thought the evidence was strongest and the likelihood of benefit high. We use “we suggest” when we reached consensus but the evidence did not reach this standard. Once the document was thought to be complete, it was reviewed by an ethicist, an infection control expert, a community nephrologist, a patient partner, and the entire CSN COVID-19 RRT. Content was presented during an interactive webinar on April 11, 2020, attended by 269 kidney health professionals, after which the document was further revised. The webinar and revised document were posted online. 21 Final revisions were made based on feedback received until April 13, 2020. CJKHD editors reviewed the parallel process peer review and edited the manuscript for clarity.
Basis of These Recommendations
They aligned with most provincial public health recommendations.
They consdidered the different prevalence of COVID-19 within each community at different times (periods of low prevalence before and toward resolution of the pandemic).
They consdidered that hemodialysis centers throughout the country are of varying size and have different access to resources.
They were based on the best judgment of the workgroup after consideration of: known published peer-reviewed and non-peer-reviewed preprints, guidelines from other jurisdictions, input from infection control experts, and comments from knowledge users.
They attempted to uphold ethical principles that balance the needs and rights of the individual patient against the public good in the setting of finite resources.
Ethical Principles
Each recommendation considered several principles of care and its underlying ethical tenets.
Fairness—ensure that patients continue to receive appropriate treatments regardless of their COVID-19 status and avoid adverse outcomes that disproportionately impact those who are most vulnerable (eg, lower socioeconomic status).
Minimize net harm: limit the spread of disease and disruption to the health care system.
Reciprocity
Macro-allocation: optimize use of resources to maximize health outcomes for the greatest number, realizing that previous standards may need to be temporarily adjusted.
V. Maintain patient-centered care with respect to privacy, treatment location, rights to visit loved ones, and the provision of optimal medical and preventative care:
Respect for autonomy: Maintain patient-centered care as much as possible for all patients with respect to their preferences, granting that choices may be limited in a pandemic.
Fidelity: Maintain commitment to patients to provide necessary and optimal medical care, even through challenging times and when there is a degree of risk to providers.
Proportionality: Keep restrictions on staff and patients commensurate with level of risk to public health.
Scope of This Document
This document pertains to the practice of outpatient hemodialysis. Inpatient hemodialysis, home dialysis, chronic kidney disease care, access considerations, and acute kidney injury are not in the scope of this document.
This document pertains to infection control aspects related to the unique circumstances of in-center hemodialysis patient care. Other general infection control practices should follow the most current provincial public health recommendations and are referred to where appropriate throughout the document.
Key Findings
Items That Should Be Prioritized For Resource Allocation by Provinces

Recommendations
A. Identification of Patients With COVID-19 in the Dialysis Unit.



Rationale
Dialysis patients have a high risk of infection because they are unable to remain isolated in their homes. Many also reside in community living settings, such as long-term care facilities, where the prevalence of COVID-19 may be high due to outbreaks. Therefore, a rigorous screening process at entry to the dialysis unit is needed to identify potentially infected patients and inform precautionary measures to prevent transmission and protect health care workers.
The presentation of COVID-19 may be atypical in dialysis patients, especially if they are elderly or immunocompromised. Security personnel–led screening at a hospital/facility entrance is rapid and standardized. These individuals may not be trained to identify probable cases as accurately as health care workers who know the patients and can detect changes in general status and symptoms.
Temperature may aid in the identification of infected patients who do not present with typical symptoms.
Patients may feel more confident and comfortable to report symptoms to health care workers if the patients are well informed about possible COVID-19 symptoms and the patients receive assurances that dialysis care will continue.
Patients who present with severe symptoms may decompensate quickly and should be directed to the emergency department or other suitable location for further assessment.
Allowing patients to call ahead allows the dialysis unit staff to best plan their treatment to minimize the spread of infection and ensure patient safety. It also ensures that patients who have severe symptoms or are unstable are identified and treated as soon as possible.
Categorizing patients according to probability of infection will inform precautionary measures to safely treat patients in the most appropriate location and in the most appropriate manner, to minimize transmission to other patients, and to protect health care workers.
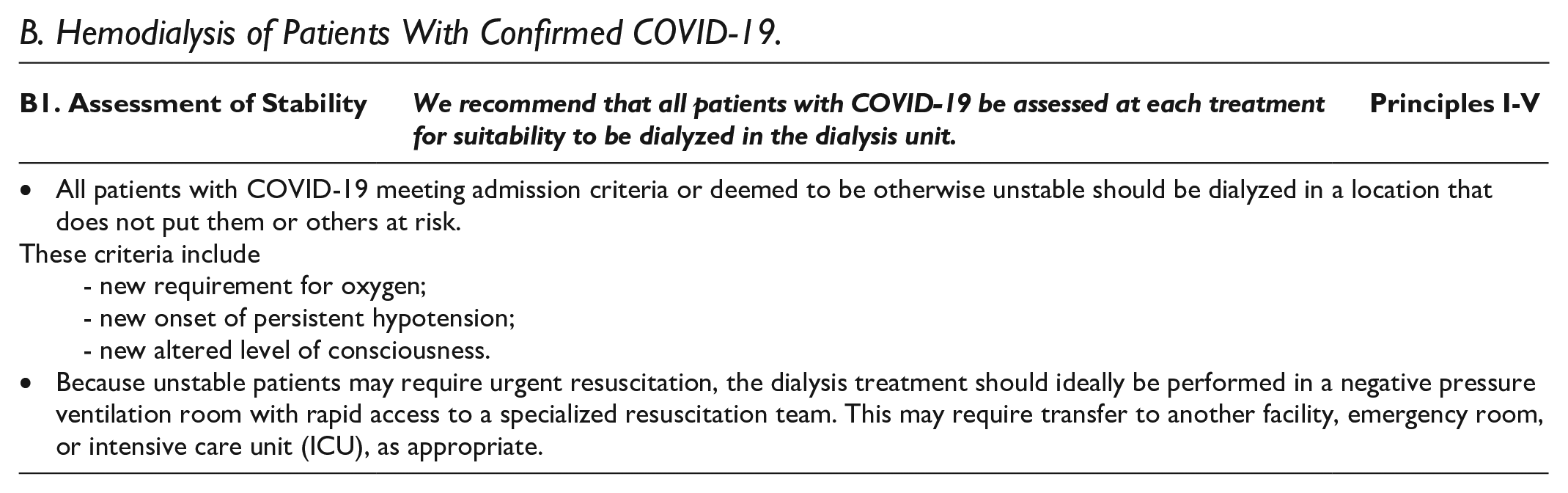
B. Hemodialysis of Patients With Confirmed COVID-19.








Rationale
Patients with severe symptomatic COVID-19 infection requiring high-flow oxygen have a very high risk of transmitting infection to others and therefore should be admitted, and dialyzed in an isolation room with airborne/droplet/contact precautions to minimize risk to nursing staff and other patients. Furthermore, such unstable patients usually require intensive nursing care which is difficult to provide in a busy outpatient unit, as every time the nurse enters the isolation room, PPE with N95 must be donned. Finally, unstable patients are at high risk of needing advanced resuscitation efforts (eg, CPR), which require expeditious access to an expert resuscitation team (see section F). For these reasons, such unstable patients should ideally not be dialyzed in the main outpatient dialysis unit.
Stable patients with COVID-19 should not be admitted to hospital as this is not likely to improve outcomes and allows inpatient resources to be reserved for those who are likely to benefit.
Isolation of stable confirmed COVID-19 patients using droplet/contact precautions while they are in hospital or treatment facility follows recommendations of provincial public health agencies. It is recognized that not all dialysis facilities have this capability. In this case, COVID-19-positive patients may be cohorted together on a single dialysis shift, accepting the small risk of cross-infection with a different COVID-19 strain. Finally, it is recognized that some dialysis units already at capacity may not have the ability to reserve an entire shift for just a few patients with confirmed COVID-19. For such units, a protocol of dialysis under fixed dialysis resources would need to be considered (section H).
Airborne precautions (N95 masks) are only required for patients who are undergoing aerosol-generating medical procedures (AGMP); these should NOT be done in the dialysis unit (including high-flow oxygen). Please see provincial health agency website for latest recommendations on what is classified as an AGMP.
In keeping with public health recommendations, confirmed COVID-19 patients should not circulate freely in public spaces. An escort will help adherence to this recommendation, especially for those who have cognitive deficits or misunderstand the recommendations.
It is not safe for visitors to be at the bedside of a patient infected with COVID-19 during dialysis treatment. Preventing infection transmission (principle II) supersedes patient-centered care and autonomy (principle V) in this case.
C. Hemodialysis of Patients Not Yet Known To Have COVID-19.



Rationale
This guidance varies according to prevalence. At times of low prevalence, before and after the peak(s) of the pandemic, principle V (patient-centered care) can be respected over principles II and III. As prevalence increases, the index of suspicion for COVID-19 infection increases in symptomatic patients, even in the absence of identifiable exposure. The rationale for the care pathways for P1 and P2 is therefore the same as that for confirmed COVID-19. Those who are symptomatic (P1/P2) should be treated with droplet/contact precautions in keeping with provincial public health guidelines. The care pathway for P3 is based on the risk of transmission of infection by asymptomatic or presymptomatic individuals. Asymptomatic identifiably exposed patients (P3) may transmit infection to vulnerable populations and should wear masks and undergo dialysis with droplet and contact precautions accordingly. As prevalence increases in the community, all people should be considered exposed irrespective of identifiable exposure, and wear a mask during dialysis, and health care personnel should wear mask and visor when within 2 m of patients.
Care Pathway for
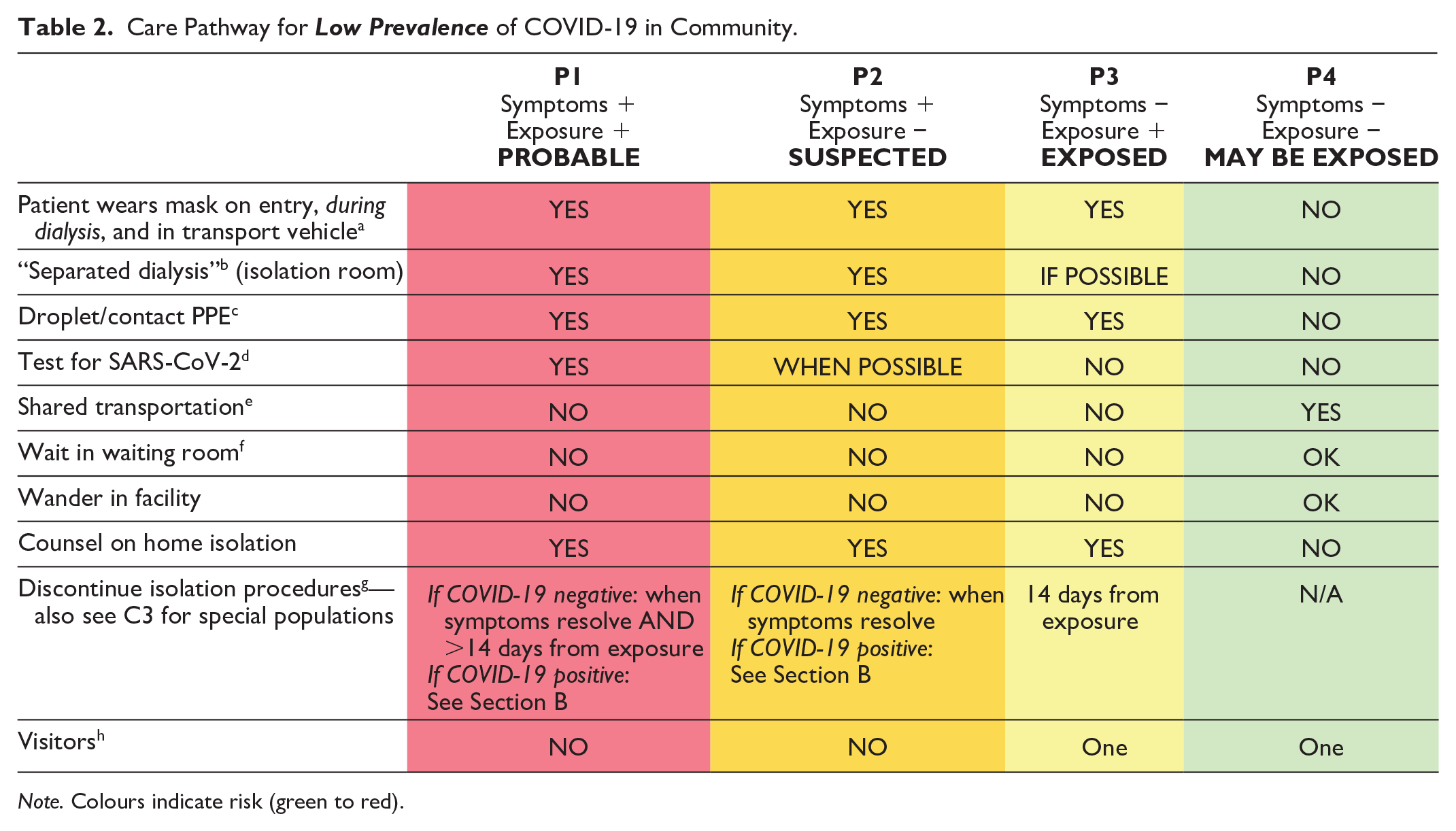
Note. Colours indicate risk (green to red).
Care Pathway for High Prevalence of COVID-19 in Community.

Masks for Patients:
• When the prevalence of COVID-19 in the community is high (as determined by public health), all patients should wear masks throughout the treatment, including P4. When prevalence is low, patients who are asymptomatic with no known exposures do not need masks.
Separated Dialysis (Isolation Rooms):
• Ideally, P1, P2, and P3 patients should be dialyzed in separate isolation rooms. If this is not possible, maintain droplet/contact precautions by keeping >2 m distance between patients AND using a physical barrier to separate treatment stations, such as plexiglass screens, washable curtains, or disposable plastic sheets. See section H.
• P1, P2, and P3 patients should NOT be cohorted together, even with patients of the same category. This is to avoid transmission from positive (but not yet confirmed) patients to those who are negative.
• Negative pressure ventilation rooms are NOT required for routine dialysis. They are recommended ONLY if an aerosol-generating medical procedure (AGMP) is anticipated, such as high-flow oxygen, intubation, or mechanical ventilation. For this reason, we recommend unstable patients are dialyzed in an appropriate location (see C1).
• Cleaning of the treatment area, machines, and isolation rooms should follow provincial public health agency guidelines.
PPE (Personal Protective Equipment):
• Health care workers who care for patients in categories P1, P2, and P3 (ie, exposed or symptomatic) require appropriate PPE for droplet/contact precautions when providing treatment or care within 2 m of the patient. This means procedure mask, visor, gloves, and gown. Airborne precautions (N95 masks) are NOT required, except for AGMPs. Dialysis is NOT an AGMP.
• For patients in category P4 (ie, no exposure, asymptomatic): Public health agencies determine whether COVID-19 is highly prevalent in the community. When this is the care, we recommend that health care workers wear a mask and visor for all patients, without changing between patients (ie, they are supplied with 1 or 2 masks for each shift and wear them continuously except for breaks).
• Whether to reuse PPE, and how to process PPE for reuse, should follow provincial public health agency guidelines.
Repeat Testing for P1 and P2 Patients who are Initially Negative:
• When there is a high clinical suspicion for COVID-19 and negative nasopharyngeal swab, the test may be repeated. The sensitivity of nasopharyngeal swab for COVID-19 may be less than 100%. Whether to do more than 2 tests for a single patient should be determined on an individual basis in consultation with local infectious disease specialists.
Transportation:
• The recommendations in section B3 apply here, except that patients who are P1, P2, or P3 should NOT be cohorted together in the same vehicle.
Waiting Room:
• If feasible, medically stable patients can opt to wait in their car or transport vehicle and be contacted by cellphone when their treatment spot is ready, to avoid the waiting room.
• If the patient must use the waiting room, practice distancing measures with patients separated by at least 2 m. This includes moving chairs to the required separation, or taping chairs that are not to be used, to maintain separation.
Discontinuation of Isolation Procedures:
• Patients in categories P1 and P2 should remain isolated until they have NO symptoms AND the patient has definitively tested negative for COVID-19.
• The duration of isolation may be longer than 14 days for immunocompromised patients—consultation with local infectious disease experts on a case-by-case basis is suggested.
• Patients in categories P1 and P3 who have been exposed to outbreaks in a group facility (eg, long-term care facility) should be isolated until at least 14 days AFTER THE OUTBREAK IS CLEARED from their group facility.
Visitors—see section D
Colours indicate level of risk (green to red).
D. Visitors.

Rationale
We recognize that not allowing visitors into the dialysis unit may be very distressing for dialysis patients and their families. The recommendations required consideration of principles II and III over principle V.
E. COVID-19 Testing in the Dialysis Unit.

Rationale
Swabbing for COVID-19 is rapid and may be easily performed by trained nurses. Ideally, it should be done in the hemodialysis unit rather than sending patients to another facility, to reduce the risk of exposing other people and to ensure the swab is performed expeditiously. There are significant differences between swabbing test kit availability and practices across provinces and different regions in Canada: the above recommendations should be discussed with local Infection Prevention and Control authorities and adjusted as needed.
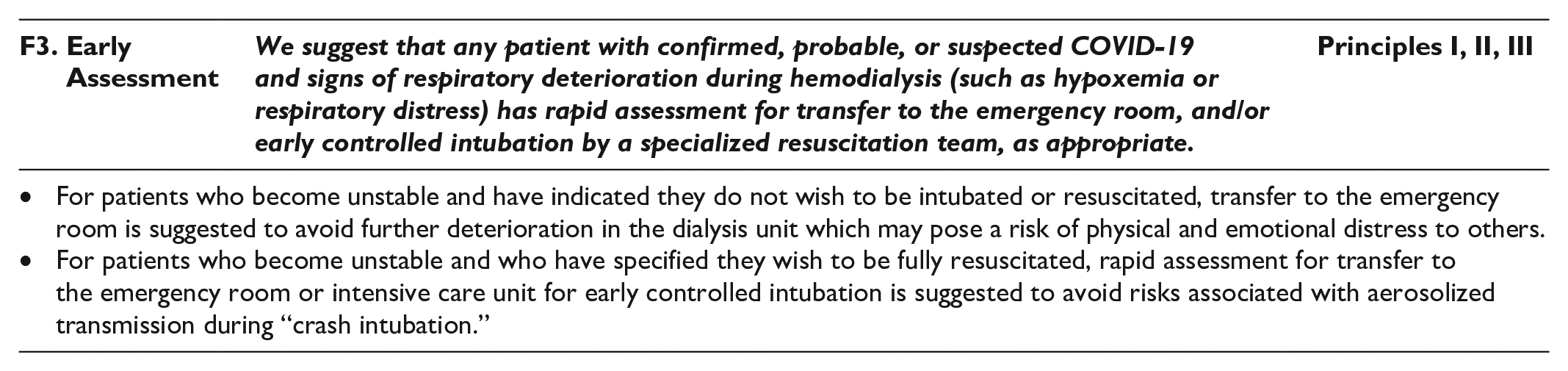
F. Resuscitation.



Rationale
The importance of respecting patient wishes, where possible (principle V), and of providing appropriate, beneficial medical interventions (principle I) were considered. However, with finite resources, it is appropriate to allocate resources (eg, ICU, ventilation) to patients most likely to survive (principal IV). Patients should have these forms in their home so that if they deteriorate at home, paramedics and other health care workers may be informed of the code status and patients’ wishes respected.
The decision to implement protected codes blue during the pandemic considers the need to protect against the risk of aerosolized transmission of the virus to other patients and health care workers24,25 and is in keeping with most provincial public health guidelines.
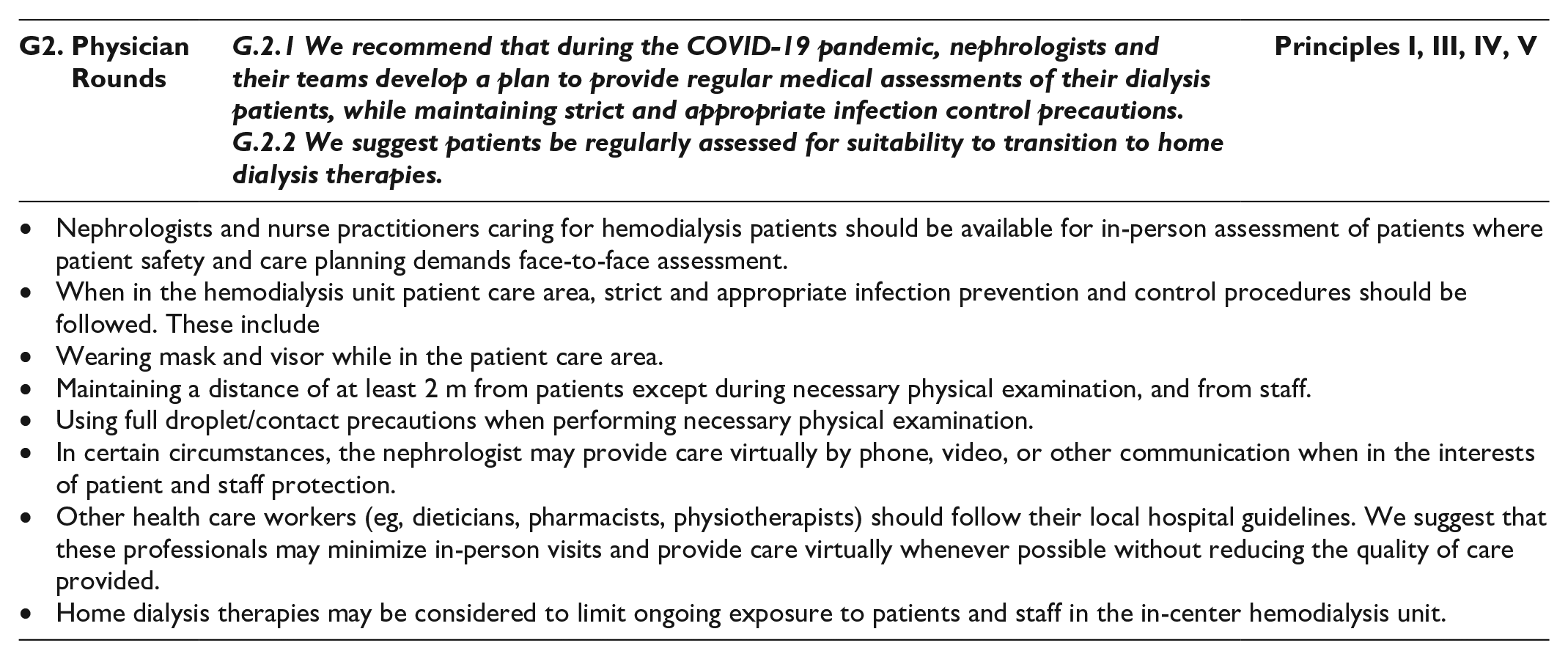
G. Routine Dialysis Care.

Rationale
Whether to continue in-person rounds or switch to a type of virtual rounds was a matter of considerable controversy among the workgroup members and was discussed at length. Pros and cons of each method were duly considered and discussed during the webinar. The need to minimize the risk of infection transmission by nephrologists rounding physically in the unit on large numbers of patients was recognized. Conversely, others were of the strong opinion that the very small (albeit nonzero) risk of infection transmission while wearing appropriate PPE and respecting >2 m physical distance is greatly outweighed by the benefits of physical presence in being able to detect patient problems and provide more optimal medical care. All workgroup members agreed that physical examination of patients should be limited to those in whom it was deemed absolutely necessary.
H. Dialysis Under Fixed Dialysis Resources.



Rationale
Most of the hemodialysis facilities do not have enough isolation rooms to be able to accommodate large numbers of patients requiring droplet/contact isolation precautions (confirmed COVID-19, probable or suspected COVID-19, asymptomatic exposed to COVID-19, non-COVID-19 infections such as Clostridium difficile, etc). Ensuring protection of noninfected patients and staff is paramount and may require modifications to dialysis treatment schedules, but this should be duly balanced with the need to ensure adequate dialysis treatment for the individual patient requiring isolation.
Summary of Risk Categories.

Note. Exposure is defined as travel outside of Canada, close contact with a person infected with or suspected to have COVID-19, or contact with bodily fluids from a person with or suspected to have COVID-19, OR living in a nursing home, regardless of whether there is an outbreak. COVID = coronavirus disease.
Similarly, if a severe shortage of hemodialysis nursing staff during the pandemic (eg, from illness, quarantine, deployment to other units, or because of markedly increased numbers of patients needing acute dialysis for acute kidney injury), multiple options may need to be considered to change nursing-to-patient ratios, or to temporarily change dialysis schedules so that the greatest number of patients be allowed to receive an acceptable minimum amount of dialysis.
Some observational studies have shown that twice-weekly dialysis can be used for a subset of patients with preserved residual kidney function and minimal interdialytic weight gain, who do not have hyperkalemia or marked comorbidity.26-28 In these selected patients, residual kidney function is preserved and survival is comparable to that of patients receiving thrice-weekly hemodialysis. If residual renal urea clearance cannot be measured, reliance on urine volume is an option (using a threshold of >600 mL to identify those that can switch to a twice-weekly hemodialysis schedule). Alternatively, an algorithm may be used based on average weekly weight gains and potassium values (Tables 4 and 5, Supplementary Material). The period of twice-weekly dialysis should be limited, with careful monitoring of symptoms, blood work, hemodialysis ultrafiltration, and residual urine output on a routine basis.
Limitations
To expedite timely publication of these recommendations to aid decision-making during the pandemic, a systematic review was not undertaken. The recommendations are based on expert opinion and subject to bias. The parallel review process that was created may not be as robust as the standard peer review process.
Implications
These recommendations may provide guidance for dialysis unit directors, clinicians, and administrators on how to limit infection and risk while providing necessary dialysis care in a setting of finite resources. Items requiring prioritization of resource allocation by provincial funding agencies are also identified.
Supplemental Material
Appendix – Supplemental material for Management of Outpatient Hemodialysis During the COVID-19 Pandemic: Recommendations From the Canadian Society of Nephrology COVID-19 Rapid Response Team
Supplemental material, Appendix for Management of Outpatient Hemodialysis During the COVID-19 Pandemic: Recommendations From the Canadian Society of Nephrology COVID-19 Rapid Response Team by Rita S. Suri, John E. Antonsen, Cheryl A. Banks, David A. Clark, Sara N. Davison, Charles H. Frenette, Joanne E. Kappel, Jennifer M. MacRae, Fabrice Mac-Way, Anna Mathew, Louise M. Moist, Elena Qirjazi, Karthik K. Tennankore and Hans Vorster in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The CSN COVID-19 RRT thanks Julie Leidecker and Filomena Picciano for their invaluable assistance; they were instrumental in organizing the workgroups and webinars. The workgroup thanks and acknowledges the BC Hemodialysis Infection Control Working group and the Institut national de santé publique for indirect contributions to the content of the recommendations. The workgroup thanks Dr Kathryn Hart (infectious diseases expert) and Dr JP Harmon (community nephrologist) for thoughtful parallel peer review of this document, as well as those who participated in the webinar and or gave feedback in the open online review. All comments were considered and incorporated into this work. R.S.S. is supported by a Chercheur-boursier clinicien (Junior 2) award from the Fonds de recherché du Québec—Santé (FRQS).
Ethics Approval and Consent to Participate
This work did not involve human subjects.
Consent for Publication
All authors provided consent for publication.
Availability of Data and Materials
Not applicable as original data was not collected for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.