
Abstract
Background:
Our institution is the largest pediatric kidney transplantation (KT) center in Canada and the referral center for pediatric KT in Ontario. Pediatric KT recipients are referred to our center for KT and transferred back to their local tertiary care institutions for post-transplant care. This investigation assesses whether the current system of transferring patients back to their local tertiary care institutions following KT allows decreased burden and distribution of resources from a single centralized surgical center.
Methods:
A retrospective review of KT performed at our institution between 2000 and 2015 was performed. Patients were divided into those who began their chronic kidney disease (CKD) care at our institution and those who began their care elsewhere. Readmission to our institution within 1 year of KT for surgical and nonsurgical complications was compared. The geographical proximity of patients to our institution and institution of initial CKD care was assessed quantitatively and mapped visually.
Results:
Of 324 patients who underwent KT, 244 (75.3%) began their CKD care at our institution. Those who began their CKD care at other institutions had shorter initial admissions to our institution (17 [14-24] vs 14 [12-17], P < .0001) and were less likely to be readmitted to our institution for nonsurgical concerns at <6 months after transplant (P < .0001) and 6 to 12 months after transplant (P < .0001). There were similar readmissions for complications requiring surgical management. The relationship between the center of CKD initiation and readmission remained significant on multivariate analysis. There was a significant difference in distance (km) to our institution between the 2 groups (46 [interquartile range = 24-109] vs 203 [117-406], P < .0001).
Conclusion:
Patients who are geographically distanced from our institution began their CKD care at their closest institution and were managed effectively at those institutions following initial discharge/transfer of care, suggesting that there is an effective distribution of health care resources with regard to CKD and KT care.
Introduction
Kidney transplantation (KT) is a definitive treatment of end-stage renal disease (ESRD) in children and adults. Although kidney transplant often allows improved survival and quality of life benefits compared with being on dialysis, patients are often subjected to a kidney transplant center where a multidisciplinary transplant team is involved in the preoperative, intraoperative, and postoperative planning and management.1,2
In a previous investigation by Kim et al, 3 a higher rate of hospitalizations was observed for kidney transplant patients in a Canadian tertiary institution than those reported by hospitals in the United States. This may be attributed to the geographic limitations of Canadian transplant centers. There are a total of 25 KT centers in Canada, with even only fraction of those offering routine pediatric transplantation. In comparison, there are more than 200 KT centers in the United States, with 37 institutions offering pediatric transplants.4-7 Our institution is the largest pediatric KT center in Canada, as well as the referral center for pediatric KT for the province of Ontario. Children who receive their chronic kidney disease (CKD) care at their local tertiary care institution are referred to our center for transplant assessment and receive their kidney transplant at our center. Following the transplant surgery and initial transplant care, their long-term post-transplant follow-up is provided by their local tertiary care institution. This system may allow for decreased burden on our institution from taking over care for all kidney transplant patients in Ontario and dividing the long-term kidney transplant care across Ontario’s other pediatric tertiary care institutions. Moreover, if necessary, post-kidney transplant follow-ups are being appropriately transferred to patients’ local tertiary care institutions; hence, there is decreased burden on patient and their families from traveling long distances to follow up at our institution.
Therefore, we hypothesize that there is an effective geographical distribution of post-KT care between our institution and other tertiary care institutions as our institution is able to transfer patients who had received surgical care back to their local tertiary care institutions. We aim to investigate this by assessing the distribution of ESRD patients among tertiary care institutions based on geographical distance and comparing the number of post-transplant hospitalizations/complications that present to our institution following initial discharge/transfer of care. We expect to find higher number of readmissions for nonsurgical concerns for patients whose ESRD care was arranged at our institution when compared with patients whose ESRD care was arranged elsewhere. However, the number of readmissions for surgical complications requiring intervention should be similar as transplant recipients are transferred back to our institution where the transplantation was performed for management of surgical complications.
Methods
Following approval by the institutional research ethics board (REB 1000027922), all pediatric kidney transplant patients (age <18 years) who underwent a KT in our institution between 2000 and 2015 were identified. All patients required a pretransplant evaluation by our multidisciplinary transplant team to be considered for KT. Following KT, all recipients received triple immunosuppressive regimen according to institutional protocol that includes prednisone, an antiproliferative agent, and a calcineurin inhibitor. All patients received induction therapy with thymoglobulin or anti-CD25 monoclonal antibodies (daclizumab/basiliximab).
The clinical parameters were collected using the institutional electronic patient database. Baseline characteristics collected included age, first 3 digits of postal code (represents a geographical area covering an average of 8000 households), 8 sex, weight, height, donor kidney volume, ESRD etiology, previous dialysis type, donor type, vascular anastomotic time off ice, number of anastomosed arteries/veins/ureter, site of artery/vein/ureter anastomosis, prior KT, and estimated blood loss. Clinical outcomes assessed included duration of hospitalizations (initial admission for transplant, other hospitalizations within 1 year of transplant), medical complications, and surgical complications.
The collected data were internally validated through a random counter-verification of 15% of the total extracted data. An additional validation was performed using the institutional CKD database, which is maintained separately from the electronic patient database.
Patients were divided into 2 groups for analysis: (1) patients who received their CKD care at the Hospital for Sick Children, and (2) patients who received their CKD care at other tertiary care institutions and were referred to the Hospital for Sick Children for kidney transplantation. The patient distribution was further plotted using the first 3 digits of patients’ postal code on a mapping software (MaptiveTM) and a heatmap marking patient distribution, as well as approximate areas covered by our institution and nearby tertiary care pediatric institutions were created.
Primary clinical outcomes of interest (readmission rates between 0 and 6 months and 6 to 12 months, any surgical complications requiring intervention) were compared between the 2 groups using χ2 or Fisher exact test for categorical variables and Mann-Whitney U test for comparison of continuous data. All statistical tests were performed using Statistical Package for Social Sciences Software (version 20.0.0, IBM Corp, Armonk, New York).
Results
A total of 332 patients were identified. Eight patients were excluded following external validation due to inconsistencies in data that included inadequate procedure details and lack of post-transplant outcomes. Of the 324 patients included in the analysis, 244 patients received their CKD care at our institution and 80 patients received their CKD care at another institution. The heatmap of patients’ distributions based on proximity to pediatric tertiary care institutions is shown in Figure 1 (patients who received CKD care at our institution) and Figure 2 (patients who received CKD care at another institution). The heatmap allows visualization of patients’ geographic proximity to their initial tertiary care institution where CKD care was initiated. The tertiary care institution where CKD care was initiated is an approximate epicenter of patient distribution, suggesting that patients are being appropriately followed at the local tertiary center institution, minimizing the necessity for travel.

Heatmap distribution of patients who began their chronic kidney disease care at the Hospital for Sick Children.

Heatmap distribution of patients who began their chronic kidney disease care at other tertiary care pediatric institutions in Ontario.
In comparing the baseline characteristics, there were significant differences in age, weight, height, donor kidney volume, and site of venous anastomosis (Table 1). Patients whose care was initiated at other institutions were more likely to be younger, weighing less, and shorter than the other 2 groups. This difference can be explained as adolescents whose CKD care is provided by their local tertiary care institution may not be referred for KT at our center, but receive their KT at their local tertiary care institution.
Comparison of Baseline Characteristics Between Patients Who Began Their Chronic Kidney Disease Care at the Hospital for Sick Children (SickKids) Compared to Those Who Began Their Chronic Kidney Disease Care at Other Institutions.

Note. IQR = interquartile range.
When comparing the days of initial admission, those who began their CKD care at other institutions had shorter admissions to our institution (P < .0001; Table 2); however, they were also less likely to be readmitted to our institution for nonsurgical concerns at both <6 months after transplant (P < .0001) and 6 to 12 months after transplant (P < .0001). In comparison, there were no differences in readmissions for complications requiring surgical management (Table 2).
Summary of Admission Statistics to the Hospital for Sick Children Within 1 Year of Kidney Transplant.

Note. IQR = interquartile range.
The geographical distance from the Hospital for Sick Children was significantly greater for patients whose CKD care was provided at other institutions (P < .0001, Table 3). When broken down into specific institutions, the median distance for patients from each institution correlated with the actual distance of each institution from the Hospital for Sick Children (Table 3, Figures 1 and 2). Patients’ distances from their own institution were closer to their institutions and saved at least 50 km of travel distance and up to >300 km if initially receiving care in Ottawa.
Geographic Distance to the Hospital for Sick Children, Based on Institution of Initial Chronic Kidney Disease Care.

Note. IQR = interquartile range.
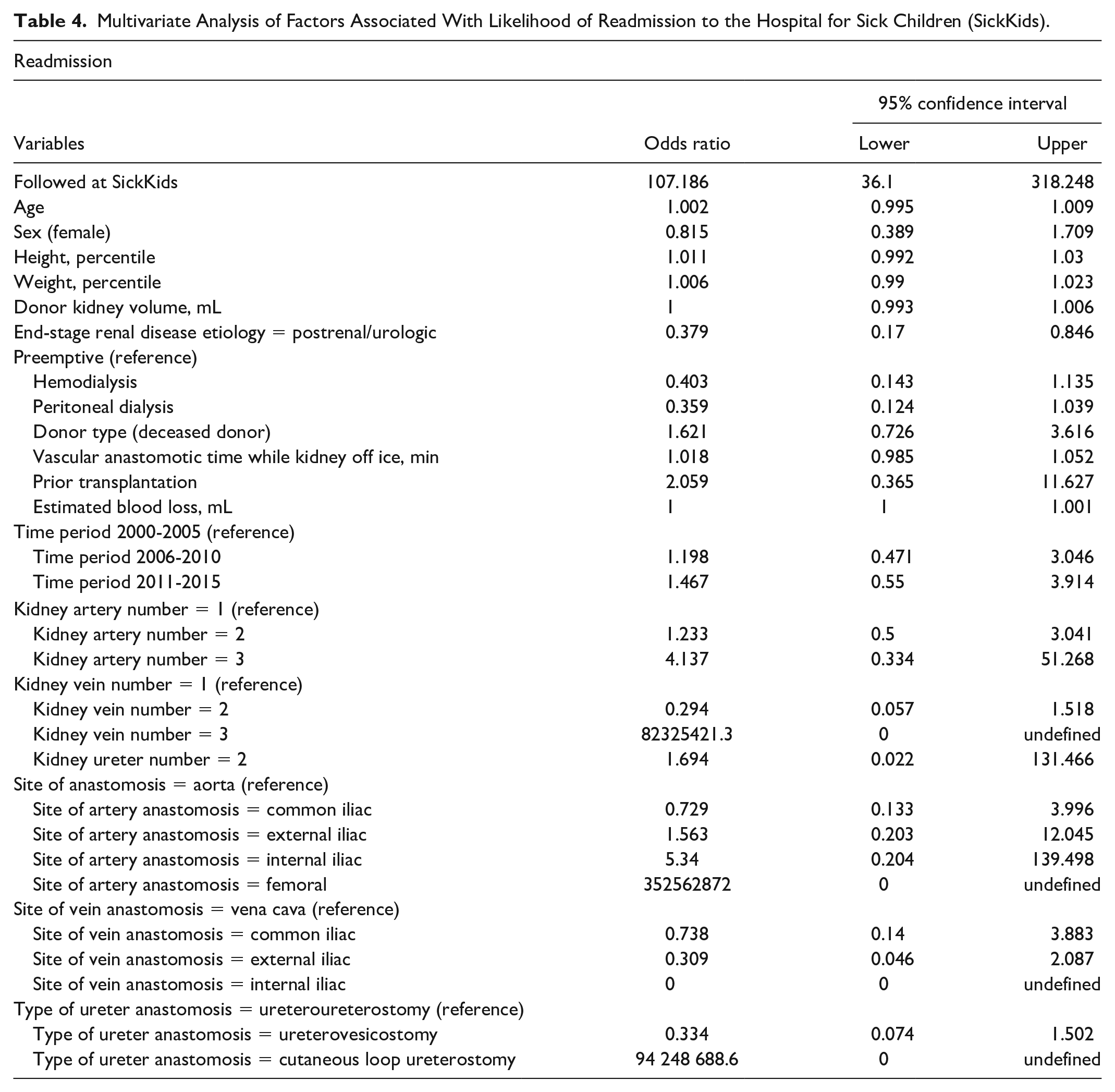
Multivariate analyses controlling for baseline characteristics were performed for univariate analyses shown in Table 2. Those who were followed at our institution were still significantly more likely to be readmitted at our institution following KT (P < .0001, odds ratio = 107.2 [95% confidence interval = 36.1-318.2]; Table 4). No associations between the length of initial admission and readmission for complications requiring surgical management were found on multivariate analyses (Tables 5 and 6).
Multivariate Analysis of Factors Associated With Likelihood of Readmission to the Hospital for Sick Children (SickKids).
Multivariate Analysis of Factors Associated With Length of Initial Admission to the Hospital for Sick Children.

Multivariate Analysis of Factors Associated With Complications Requiring Surgical Intervention.

Discussion
Kidney transplant, despite being a definitive and preferred treatment for ESRD, has limitations in requiring a multidisciplinary team in a kidney transplant center due to its complexity. In Canada, where there are much fewer KT centers compared with the United States and even fewer pediatric KT centers, geographical distribution of patients may play a large role in their access to medical care following KT. Despite this, there have not been any investigations that attempted to understand how effective the CKD care is distributed within Canada. Thus, this investigation attempted to characterize this by comparing institutional distribution, based on geographical distance from our institution, of all patients who underwent KT at our institution between 2000 and 2015 while also assessing the likelihood of readmission to our institution following initial discharge/transfer of care.
When assessing the geographical distances for patients, those whose CKD care was initiated at our institution were significantly closer to our institution compared with those whose CKD care was initiated at other institutions. There was substantially less travel distance when patients were traveling to their initial institution, with median distances saved in Ontario residents that varied from 50 km to more than 300 km. In addition, the median distance for patients from their specific institution correlated with their actual distance from our institution, suggesting that there is shared CKD care that is appropriately distributed based on geographical location of patients (ie, the median distance from our institution, least to greatest, was in order of McMaster Children’s Hospital, London Health Sciences Centre, and Children’s Hospital of Eastern Ontario). This can also be visually observed in Figures 1 and 2. In Figure 2, specifically, one can observe the focused density of patient population around other tertiary care pediatric institutions where they began their CKD care.
Furthermore, patients who were referred from other institutions had fewer days of initial admission after transplant surgery at our center. This is because they were transferred back to their local institution once they were stable to complete their medical management post-KT prior to discharge home (ie, the initial admission to our institution does not reflect the number of additional days that they would be admitted at their local tertiary care institution), as compared with our own patients who remained as inpatients in our institution until they were ready to be discharged home. Nonetheless, this association was not statistically significant in our multivariate model. In addition, there was a noticeable difference in the rates of readmission for nonsurgical concerns when comparing those whose CKD care was initiated at our institution with those whose CKD care was initiated at other institutions. The latter group was less likely to be readmitted within 1 year of KT, and this association remained statistically significant in our multivariate model. This is because their ongoing management for nonsurgical concerns is delivered by their home pediatric institutions. In comparison, there was no difference in the proportions of surgical complications that presented to our institution within 1 year of KT as we manage the surgical aspects of pediatric KT in these children.
These results reflect the pediatric KT model employed in the current Ontario system—any surgical complications require readmission and further management at our institution, whereas medical management occurs at their local tertiary care institutions where their initial CKD care was initiated. This model allows decreasing the burden of travel and associated costs to the family while also allowing the care to be delivered more efficiently and timely at the closest major pediatric institutions with experience in managing KT patients. These findings indirectly represent aspects of cost-effectiveness in the Canadian health care system. 9 By distributing the patient cohort across multiple tertiary care institutions, we are able to avoid burdening a single large tertiary care institution from all of the pharmaceutical, typical in-hospital care services, diagnostic/investigational services, and physician/nonphysician professional services associated with each patient follow-up and visit, especially if patients require readmission. Moreover, we are able to minimize the personal costs, including personal travel costs and caregiver costs, for patients’ families who would otherwise be required to travel extended lengths for each follow-up visit to our institution. Therefore, the results of this investigation support that this model may be a way of the Canadian health care system in compensating for large catchment areas covered by few pediatric KT centers available across the country.
Although there were some differences in the baseline characteristics between patients, if these were viewed with a conservative outlook with Bonferroni correction applied, only age, height, and weight had statistically significant results, as α value would be set at approximately 0.003. However, as mentioned, these differences can be explained by the higher likelihood of older pediatric patients undergoing KT with adult kidney transplant surgeons at their local tertiary care institutions.
This investigation has several important limitations. First, as a retrospective investigation, there is potential for sampling bias; however, this was minimized by ensuring all patients within our assessed timeline were included. Moreover, there is potential for unaccounted confounders, although this was minimized by collecting all available clinical information on our institutional electronic patient record and internally validating them. Despite the differences that exist in baseline characteristics such as age, weight, height, donor kidney volume, and site of vein anastomosis, this investigation focuses on the logistics behind how the current logistics allows effective distribution of health care resources in the universal access to care system, and these clinical limitations of clinical findings may not be applicable in highlighting the significance of our findings. Other variables often reported for KT outcomes include graft loss; however, this was not reported in our cohort as the authors did not believe it was within the scope of the research question, which was to understand the division of care among tertiary care institutions based on geographical location of patients. This investigation is also not generalizable to the whole Canadian pediatric kidney transplant experience, as the Canadian health care is delegated on the provincial level and there are different distributions of pediatric KT centers in other Canadian provinces and territories.
Despite these limitations, this investigation is the first to investigate the patient distribution burden of post-KT care in Ontario’s current system. Our investigation suggests that the model that divides medical and surgical management of KT patients across major pediatric institutions may compensate for the large catchment area for pediatric KT centers with large catchment areas. Despite these findings suggesting the effectiveness of the current system employed in Ontario, in a resource-constrained setting of universal health care system, further investigations are required to understand whether there are means of creating a more cost-effective system. As there are suggestions from previous investigations for differences in clinical outcomes such as hospitalization rates between Canada and the United States, there is further role in investigating the differences in systems and designing quality improvement and cost-effectiveness studies are required to explain such differences for further optimization of Ontario and Canadian system. 3
Conclusion
The current system where patients undergo their CKD care occurs in their local tertiary institutions and subsequently transferred back following their KT may be an effective way of patient care for KT centers with large catchment areas.
Footnotes
Ethics Approval and Consent to Participate
This study was approved by the Research Ethics Board from Hospital for Sick Children (REB 1000027922). Consent was waived due to retrospective nature of study.
Consent for Publication
Not applicable.
Availability of Data and Materials
For more information on protocol, raw data, or statistical analyses, please email corresponding author at:
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.