
Abstract
Background:
Obesity is recognized as an independent risk factor for chronic kidney disease through multiple direct and indirect biological pathways. Bariatric surgery is a proven, effective method for sustained weight loss. However, there is a relative paucity of data on the impact of bariatric surgery on renal outcomes.
Objective:
The primary objective was to evaluate the change in urine albumin/creatinine ratio (ACR) in patients undergoing bariatric surgery, at 12 months after the procedure. Secondary objectives were to determine the changes in ACR at (6 and 24 months), estimated glomerular filtration rate (eGFR; 6, 12, and 24 months), and hemoglobin A1c (HbA1c); 12 and 24 months) after the procedure.
Design:
This observational retrospective cohort study included consecutive obese patients who underwent bariatric surgery.
Setting:
Provincial Bariatric Surgery Clinic at the Regina General Hospital, Saskatchewan.
Patients:
This study includes 471 consecutive obese adult patients who underwent bariatric surgery between 2008 and 2015.
Measurements:
We studied the impact of bariatric surgery on body mass index (BMI), renal outcomes (urine ACR and eGFR) and metabolic outcomes (fasting glucose, total cholesterol, low-density lipoprotein, triglycerides, and HbA1c) in 471 patients.
Methods:
Patients were followed for 2 years postsurgery in the bariatric clinic. Mixed linear models that accounted for the repeated nature of the data were used to access changes in outcomes over time.
Results:
Patients were predominantly female (81%) with a mean age (±SD) of 46 ± 10 years. Most patients (87%) had a BMI > 40 kg/m2 and 81% of the patients underwent Roux-en-Y gastric bypass. The mean BMI decreased from 47.7 ± 7.8 kg/m2 at baseline to 37.1 ± 7.9 kg/m2 at 6 months and 34.8 ± 8.8 kg/m2 at 12 months. In a subcohort of patients with microalbuminuria, ACR showed an improvement from a median [interquartile] value of 5.1 [3.7-7.5] mg/mmol at baseline to 2.3 [1.2-3.6] mg/mmol at 6 months (P = .007), to 1.4 [0.9-3.7] mg/mmol at 2-year follow-up (P < .001). Similarly, eGFR increased in patients with microalbuminuria from 109 ± 10 mL/min/1.73 m2 at baseline to 120 ± 36 mL/min/1.73 m2 at 2-year follow-up (P = .013). There were statistically significant reductions in triglycerides, fasting glucose, and HbA1c.
Limitations:
This was a retrospective chart review, with the lack of a control group. Patients with eGFR less than 60 mL/min/1.73 m2 were not considered for surgery, and we had to measure renal outcomes predominantly on the presence of proteinuria.
Conclusions:
Our results suggest bariatric surgery significantly decreased weight and consequently improved renal and metabolic outcomes (eGFR, ACR, fasting glucose, cholesterol, and triglycerides) in patients with elevated BMI.
What was known before
Bariatric surgery is an effective alternative to achieve significant and sustained weight loss. There was a relative lack of long-term data on renal outcomes.
What this adds
This study adds to the growing literature on renal outcomes after bariatric surgery. It adds to long-term (2 year) safety of the procedure and positive sustained impact on renal outcomes.
Background
Both obesity and chronic kidney disease (CKD) constitute high-prevalence medical conditions with a significant impact on health care systems. In 2014, 20% of adult Canadians were obese. At the same time, the global prevalence of CKD is estimated to be around 13%. 1 There seems to be a strong pathophysiological association between these 2 entities. 2 In addition to increasing the risk of hypertension and diabetes, excessive adipose tissue is responsible for the activation of the sympathetic nervous system and eventually renin-angiotensin system leading to hypertension. 3 It also leads to insulin resistance through disruption of insulin signaling pathways from lipolysis and release of inflammatory markers. 3 Obesity is also considered an independent risk factor for the development of CKD through multiple biological pathways including compression-induced increased renal sodium reabsorption leading to afferent arteriolar vasodilation and consequently, hyperperfusion, hyperfiltration, and worsening albuminuria/proteinuria.4-6 Furthermore, increased adipose tissue has been associated with the presence of histological changes in the kidney including focally thickened basement membrane, dilated capillary loops, thickened foot processes, glomerulomegaly, and eventually glomerulosclerosis.7-9 The combined direct effect of obesity and indirect impact of hypertension, diabetes, and metabolic syndrome on the glomerular barrier can be clinically evaluated by measuring albuminuria and altered glomerular filtration rates (GFRs).
Given the strong association between obesity and CKD, it is plausible that interventions leading to significant weight loss may benefit renal function. Previous studies have estimated that every kilogram of intentional weight loss may result in a 4% reduction of proteinuria, regardless of the beneficial effect of weight loss in blood pressure. 10 Bariatric surgery is a proven, effective procedure for sustained weight loss and is increasingly being considered for patients with morbid or severe obesity. Options for bariatric surgery include Roux-en-Y gastric bypass (RYGB), laparoscopic adjustable gastric banding, and laparoscopic vertical sleeve gastrectomy (LSG).2,11,12 All of these procedures are associated with significant and sustained weight loss and potential remission of diabetes, hypertension, and dyslipidemia.13-15
While there is strong evidence of improved metabolic outcomes, there is paucity of long-term data on renal outcomes (proteinuria and estimated glomerular filtration rate [eGFR]) in Canadian patients. Previous studies looking at renal measures in obese subjects have been limited by heterogeneity in outcomes and variable duration of follow-up.16-20 In this single center, retrospective population-based cohort, we attempted to identify the long-term impact of bariatric surgery on renal function of obese patients treated in a single-center provincial bariatric program.
Methods
Study Design
Retrospective review of electronic medical records of all the patients who underwent bariatric surgery at the Regina General Hospital between 2008 and 2015 was performed. Demographic, clinical, and biochemical data were collected. Demographic data included age (years) and sex. Clinical data included height (cm) and weight (kg), BMI (kg/m2), and the type of bariatric surgery (RYGB or LSG). Biochemical data included albumin (g/L), creatinine (μmol/L), albumin/creatinine ratio (ACR; mg/mmol), glucose (mmol/L), hemoglobin A1c (HbA1c; %), total cholesterol (mmol/L), triglyceride (mmol/L), and low-density lipoprotein (LDL) cholesterol (mmol/L). Diabetes was defined according to the American Diabetic Association (fasting glucose >7.0 mmol/L and HbA1c >6.5%) and normoglycemia (fasting glucose <5.6 mmol/L and HbA1c <5.7%). Microalbuminuria was defined as ACR >2.0 and <20 mg/mmol in men and >2.8 and <28 mg/mmol in women, and macroalbuminuria was defined as ACR >20 mg/mmol in men and >28 mg/mmol in women. Glomerular filtration rate was calculated by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula. 21 The study was approved by the Research Ethics Board of the former Regina Qu’Appelle Health Region (REB-17-86).
Surgical Eligibility Criteria
The provincial bariatric surgical program at the Regina General Hospital, Saskatchewan, Canada, accepts referrals from family doctors across the region for assessment for weight reduction surgery. Criteria for surgery were based on the National Institute of Health guidelines and included the following: body mass index (BMI) ≥40 kg/m2 or 35 to 40 kg/m2 with 1 obesity-related comorbidity and a prior attempt to lose weight. Patients aged <18 or >60 years and had GFR <60 mL/min/1.73 m2 were not eligible for bariatric surgery. Patients were initially assessed by a multidisciplinary program (psychologist, exercise therapist, and dietitian) along with the bariatric surgeon. They were instructed to follow a diet reduction regime for a period of 6 months and subsequently re-evaluated by the multidisciplinary team.
Surgical Interventions and Follow-Up
Two procedures (RYGB and LSG) were predominantly performed for weight loss surgery at the Regina General Hospital. In RYGB, the stomach is divided into an upper stomach pouch (15-30 mL) and a lower gastric remnant. The stomach pouch is then anastomosed to the mid jejunum, and the jejuno-jenunal anastomosis is created to connect the biliopancreatic limb and the gastric remnant, thereby allowing the gastric, pancreatic, and biliary secretion to mix with the food in the jejuno-jejunal anastomosis. 2 Laparoscopic vertical sleeve gastrectomy is a restrictive surgery that involves the removal of 70% to 80% of the lateral stomach. 2 Both procedures are widely accepted and validated as appropriate surgical options for weight loss by the American Society of Bariatric and Metabolic surgery. Postoperatively, patients were seen at scheduled intervals for 2 years to monitor for any surgical, metabolic, or nutritional complications from their procedures.
Statistics
All statistical analyses were performed using SPSS version 22 (SPSS Inc, Chicago, IL). Continuous variables are summarized as mean ± SD or median (interquartile range [IQR]), as appropriate. Differences in outcomes over time were assessed using mixed linear models that accounted for the repeated nature of the data and within-subject correlation; both intercept and time were specified as fixed effects and an unstructured covariance was specified. Time (visit) was treated as a repeat measure and was categoric when specified in the model. A P-value <.05 was considered statistically significant.
Results
Patient Characteristics
Baseline characteristics of the 471 study participants are shown in Table 1. Most of the study participants were women (81%), and the mean age at surgery was 46 ± 10 years.
Baseline Patient and Surgery Characteristics.

n = 417 due to missing data.
Weight loss and changes in metabolic parameters
There were significant changes in weight and BMI following surgery (Figure 1). Three percent of patients had a BMI of 30 to 34.9 kg/m2, 11% had a BMI between 35 and 35.9 kg/m2, and 87% had a BMI >40 kg/m2. Eighty-one percent of the patients underwent RYGB and 19% underwent LSD. The BMI was significantly lower 6 months after bariatric surgery for up to a 2-year follow-up period (Figure 1). The mean BMI decreased from 47.7 ± 7.8 kg/m2 at baseline to 37.1 ± 7.9 kg/m2 at 6 months after the procedure. The BMI further declined from 37.1 ± 7.9 kg/m2 to 34.8 ± 8.8 kg/m2 at 1 year. However, there was no further significant decrease in BMI in the second year after the bariatric surgery as compared with the first year. At 2-year follow-up, BMI was 34.8 ± 7.9 kg/m2.

Change in body mass index (A) and weight (B) over the study period.
Renal outcomes
Mean creatinine was 62 ± 16 μmol/L at baseline, 70 ± 15 μmol/L at 12 months, and 67 ± 18 μmol/L at 2-year follow-up. The mean eGFR was 107.5 ± 10.5 mL/min/1.73 m2 at baseline, 102.1 ± 22.4 mL/min/1.73 m2 at 1 year, and 106.2 ± 27.0 mL/min/1.73 m2 at 2-year follow-up. These results suggest that there was a decline in eGFR postsurgery that lasted up to a year and reverted back to baseline by 24 months (Table 2). The majority of patients (84%) had normal albumin excretion rates. In patients with microalbuminuria (n = 60, 12.7%), ACR and eGFR showed improvements (Figure 2). In patients with microalbuminuria, ACR showed an improvement from a median [IQR] value of 5.1 [3.7-7.5] mg/mmol at baseline to 2.3 [1.2-3.6] mg/mmol at 6 months (P = .007), to 1.4 (0.9-3.7) mg/mmol at 2-year follow-up (P < .001). Similarly, eGFR increased in patients with microalbuminuria changing from 109 ± 10 mL/min/1.73 m2 at baseline to 120 ± 36 mL/min/1.73 m2 at 2-year follow-up (P = .013).
Descriptive statistics of renal and metabolic measures over time for all patients.

significant change from baseline (P < .05).
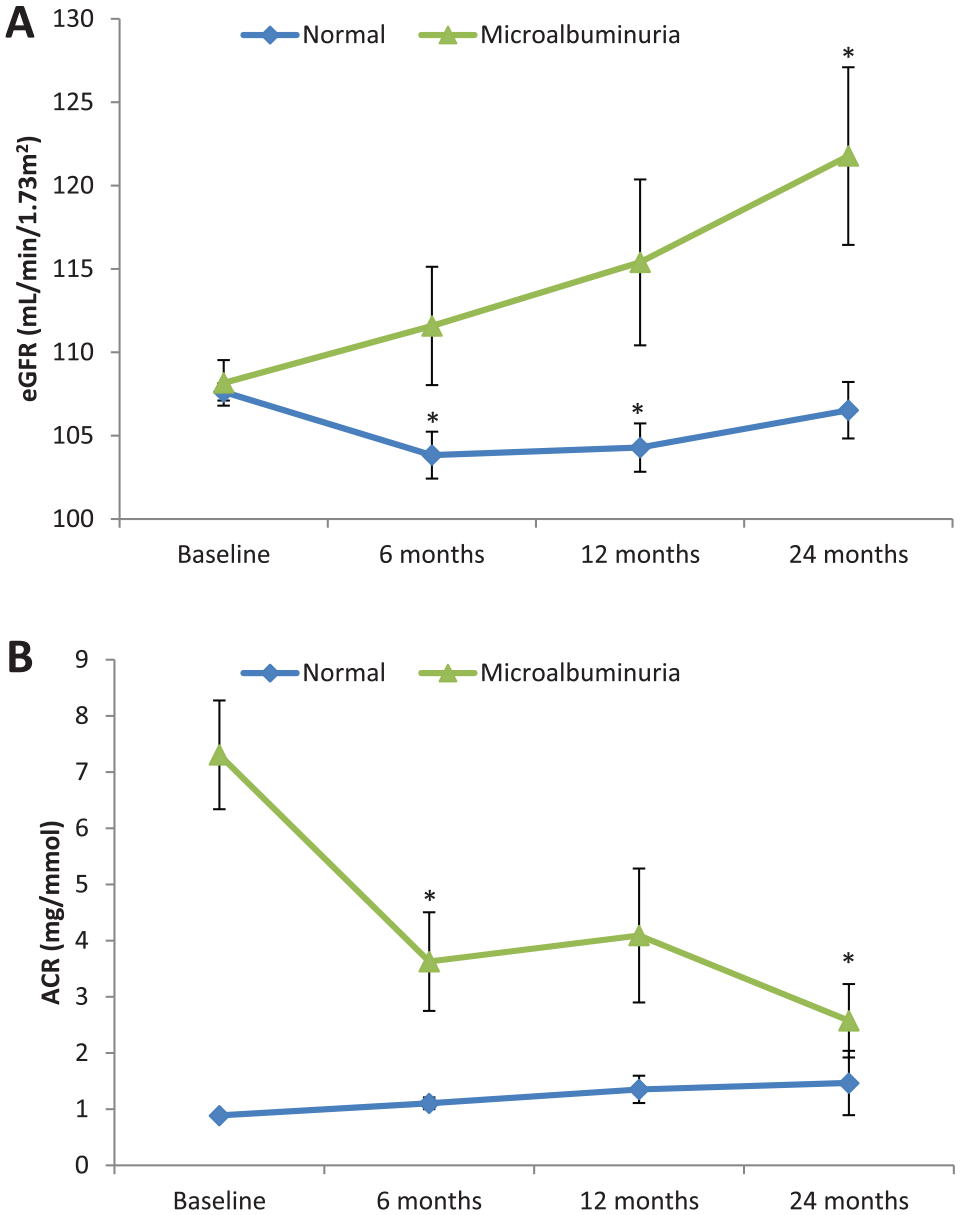
Two-year follow-up evaluation of estimated glomerular filtration rate (A) and albumin/creatinine ratio (B) in the cohort stratified according to the presence of baseline proteinuria.
Diabetes and lipid profile
A significant reduction in fasting glucose, and glycated hemoglobin levels was observed in our study at 6-month follow-up and maintained at 2-year follow-up (P < .001). There were significant improvements in serum total cholesterol and triglyceride levels at 6 months, which were maintained for 2 years (Table 2). Based on these lab values, the proportion of patients with diabetics reduced significantly from 27.8% (116/417) at baselines to 7.8% (14/179) at 6 months, 7.4% (12/162) at 1 year and 9.6% (16/146) at 2 years.
Discussion
In this single-center study, we examined the impact of bariatric surgery on renal and metabolic function using eGFR, albuminuria, serum lipid profile, glucose fasting, and HbA1c as biologic markers. We observed significant improvement in BMI from 47.7 ± 7.8 to 34.8 ± 8.8 kg/m2 by 1 year after the surgery. Our results are similar to the other published studies that show significant reduction in weight after the procedure.2,19 We also described a beneficial effect in glucose homeostasis and lipid profile comparable to those described by other groups. 22 Furthermore, we observed a reduction in albumin excretion rates amongst those subjects with albuminuria at baseline. These results are consistent with a recent systematic review that observed an overall reduction in proteinuria after bariatric surgery. 20
Over the years, bariatric surgery has built a safety record and has become an effective alternative to achieve a significant and sustained weight reduction. However, data regarding the impact and safety of bariatric procedures in patients with kidney impairment are lacking mainly because most centers will consider patients with significant renal impairment as noneligible for bariatric surgery. Preserved GFR with microalbuminuria and macroalbuminuria is the earliest clinical manifestation of renal involvement in obese patients.20,23 Although patients with abnormal albumin excretion rates contributed to only 16% of the study population, we observed a significant improvement in albuminuria after the surgery. The observed difference might have been different with a larger sample size.
Animal studies from the mid-1990s revealed several pathways for the development of proteinuria. These include elevated glomerular pressure by stretching of mesangial cells by increased hydraulic pressure,24,25 increased production of transforming growth factor beta, which impair the lysosomal enzyme activity in tubular cells 26 and endothelial cell dysfunction.27,28 There are human data to suggest that reduction in albuminuria following bariatric surgery is correlated with an improvement in insulin sensitivity, 29 favorable alterations in the levels of gut hormones that control insulin secretion, 30 reduction in renal cytokines, 31 and improvement in anti-inflammatory adipokine adiponectin. Irrespective of the pathogenesis of albuminuria in patients with obesity, improvement in albumin excretion rates following bariatric surgery suggests improved glomerular and/or systemic capillary function.
We observed that eGFR decreased for our entire cohort over the first year, which is in contrast to few other published studies showing an increase after the procedure.32,33 Obesity is hemodynamically associated with elevations in glomerular filtration (hyperfiltration). 34 Brochner-Mortensen et al 35 were the first group to demonstrate that GFR decreased after intestinal bypass surgery in obese subjects. Chagnac et al 36 also showed that after the bariatric surgery, there was a decrease in GFR, renal plasma flow, and microalbuminuria in obese patients. Our study is comparable with other published studies that showed a reduction in measured glomerular filtration rate (mGFR) due to a resolution of glomerular hyperfiltration after the bariatric surgery.36-38 We did not perform mGFR as performed in other studies and instead used creatinine-based formula (CKD-EPI equation) to estimate the GFR. It is practically impossible to measure iothalamate GFR in routine clinical care. Measurement of cystatin C would have provided a more accurate eGFR than creatinine, but we were hampered by the lack of an available assay in our Institution.
The STAMPEDE trial 39 and other randomized controlled trials40,41 further showed that bariatric surgery was superior to intensive medical therapy in improvement in lipid levels and quality of life along with better diabetic control. We similarly noticed statistically significant changes in total cholesterol and triglyceride levels, but not in LDL levels. As the key treatment goal of surgical intervention in obesity is prevention of long-term complications, it was reassuring to see results of Swedish Obesity Subject Study (SOS), show a reduction in microvascular and macrovascular complications after the bariatric surgery. 42
The effects of weight loss on diabetes status and HbA1c in our study were identical to previously published studies.43,44 Although we did not capture medication use (oral hypoglycemic agents and insulin), a significant decline in fasting glucose and HbA1c levels was seen in our cohort. Improved blood glucose regulation has been reported after the bariatric surgery leading to a reduction in the amount of insulin, and, in many cases, often discontinuation of insulin or oral hypoglycemic agents.39,43 A meta-analysis by Panunzi et al 45 reported that most obese patients (90%) entered remission of their type 2 diabetes after metabolic procedures in the short to medium term. It has been estimated that 24.2% of kidney disease cases in the United States among men and 34% among women could be prevented if overweight and obesity were eliminated. 46 Overall, the results confirm the success of bariatric surgery in our Institution. The strengths of this study include improved metabolic outcomes and reduction in albuminuria after the bariatric surgery. In addition, this is the largest Canadian cohort with 24 months of follow-up. Navaneethan et al 29 looked at 13 patients and followed them for 12 months. Similarly, the first published study from 1980 by Brochner-Mortensen et al looked at 8 patients after jejuno-ileal bypass surgery and followed them for 12 months. 35 In 2008, Agarwal et al 47 reported on 94 patients with microalbuminuria and followed them over 12 months. Serpa Neto et al 48 reported on 140 patients and followed them over 8 months. Fenske et al 49 looked at 34 patients and followed them over 12 months. Similarly, Stephenson et al 50 and Ruiz-Tovar et al 51 reported on 23 and 50 patients, respectively, and followed them over only 12 months. In contrast, in this single-center retrospective study, we present data on 471 patients followed over 24 months and is the largest Canadian cohort to our knowledge. Chang et al 2 followed 985 patients, but only 91 of the 985 patients had GFR <60 mL/min. More recent studies (Imam et al looked at 714 patients and Swedish Obesity Study) reported on a bigger cohort and followed patients over a longer period of time.52,53
Limitations of Study
Our study was a retrospective chart review, and there was no “control group” that underwent routine care in comparison, making it challenging to ascertain the kidney-specific risks and benefits of bariatric surgery. Patients with GFR less than 60 mL/min/1.73 m2 were not offered surgery by the surgical team due to perceived increased perioperative risk of acute kidney injury. Our assessment of renal outcomes was predominantly on the presence of proteinuria. Patients with impaired albumin excretion rates contributed to only 16% of patients at the time of surgery, and there was significantly high clinic dropout rate creating an opportunity for bias. We did not collect information on short- or longer-term complications related to bariatric surgery. Finally, we used CKD-EPI formula for the calculation of GFR. Creatinine-based eGFR equations have not been validated in morbidly obese adults or in patients with change in body composition after bariatric surgery. We were limited in our ability to explore the impact of the filtration rate any further because we did not measure iothalamate GFR and cystatin-based assays are currently not performed in our Institution.
Footnotes
Acknowledgements
The authors wish to acknowledge Regina Qu’Appelle Health Region, Research and Performance Support and Dr Christian Rueda-Classen, MD PhD for assisting with this study.
Ethics Approval and Consent to Participate
The study was approved by the Research Ethics Board of the former Regina Qu’Appelle Health Region (REB 17-86).
Consent for Publication
Not applicable as there is no patient identifying information in this manuscript.
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
B.P. edited the final manuscript and conceived, designed, and assisted with the multiple drafts. M.M. wrote the initial draft. G.K. assisted with the drafts. A.C. and W.B. performed the statistical analysis. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.