
Abstract
Background:
Previous guidelines recommend that living kidney donors receive lifelong annual follow-up care to assess renal health.
Objective:
To determine whether these best practice recommendations are currently being followed.
Design:
Retrospective cohort study using linked health care databases.
Setting:
Alberta, Canada (2002-2014).
Patients:
Living kidney donors.
Measurements:
We determined the proportion of donors who had annual outpatient physician visits and laboratory measurements for serum creatinine and albuminuria.
Results:
There were 534 living kidney donors with a median follow-up of 7 years (maximum 13 years). The median age at the time of donation was 41 years and 62% were women. Overall, 25% of donors had all 3 markers of care (physician visit, serum creatinine, albuminuria measurement) in each year of follow-up. Adherence to physician visits was higher than serum creatinine or albuminuria measurements (67% vs 31% vs 28% of donors, respectively). Donors with guideline-concordant care were more likely to be older, reside closer to the transplant center, and receive their nephrectomy in more recent years.
Limitations:
Our results may not be generalizable to other countries that do not have a similar universal health care system.
Conclusions:
These findings suggest significant evidence-practice gaps, in that the majority of donors saw a physician, but the minority had measurements of kidney function or albuminuria. Future interventions should target improving follow-up care for all donors.
What was known before
Recommended care for living kidney donors includes lifelong annual blood pressure measurement, serum creatinine measurement with glomerular filtration rate (GFR) estimation, and albuminuria measurement. Currently, it is unclear what proportion of living kidney donors are receiving follow-up care and how frequently the follow-up is occurring.
What this adds
Only one-quarter of donors are currently receiving the postdonation follow-up care recommended by best practice guidelines. Reassuringly, the majority of donors continued to see a physician on an annual basis.
Introduction
More than 27 000 living donor kidney transplants are performed worldwide every year. 1 Generally, long-term clinical outcomes for living kidney donors are comparable to that of nondonors of similar baseline health.2-4 However, for certain outcomes, such as end-stage renal disease (ESRD), the risk in donors may be higher than that of healthy nondonors.5-10 Despite a higher relative risk, the absolute risks for these outcomes in living kidney donors remain low with a 15-year incidence of ESRD of less than 1%.5,7,8 To mitigate potential risks to the donor and ensure overall good health, a suggested practice is for living kidney donors to receive lifelong annual postdonation follow-up care. 11 This recommendation was supported in the Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guidelines on the evaluation and care of living kidney donors. 12 Recommended care includes lifelong annual blood pressure measurement, serum creatinine measurement with glomerular filtration rate (GFR) estimation, and albuminuria measurement.
Currently, it is unclear what proportion of living kidney donors are receiving follow-up care and how frequently the follow-up is occurring. A 2007 survey of 91 transplant centers in the United States found that while all centers provided early postoperative care within 3 months of donor nephrectomy, only 30% of centers recommended follow-up at 2 years. 13 In these centers, only 26% of donors were actually seen, meaning that <8% of all donors were followed at 2 years after donation. In 2013, United Network for Organ Sharing (UNOS) implemented mandatory reporting of clinical and laboratory data for living kidney donors to the national transplant registry at 6 months, 1 year, and 2 years after donation. 14 This mandate led to an increase in the rates of early follow-up data collection across the nation, from 33% preimplementation to 54% postimplementation.15,16 Currently, donor follow-up beyond 2 years, when medical conditions are more likely to develop, is not currently mandated in the United States.6,8 In a 2004 survey of Canadian transplant centers, only 25% of programs provided follow-up for living kidney donors beyond the first year for medical and nonmedical issues, despite almost half of donors expressing that ongoing follow-up should be provided by the transplant program. 11
Long-term surveillance and monitoring can either be provided by the transplant center, local nephrologists, or family doctors. 17 While many transplant programs rely on family doctors to continue annual surveillance of donor health, it is unclear whether continued assessments are actually being performed. 13 In a 2010 survey of 276 living kidney donors from a single US center, 88% of donors reported seeing a physician in the previous year. 17 These survey studies have limitations, including response bias (only ~40% response rates from transplant centers and donors),17,18 selection bias (responders tend to be different from nonresponders), and external validity (results may not be generalizable to a Canadian population with a universal health care system).13,17
To better understand the current state of follow-up care of living kidney donors, we performed a retrospective cohort study using health care administrative databases in Alberta, Canada. We examined the proportion of living kidney donors who had evidence of annual outpatient physician visits, serum creatinine measurements, and albuminuria measurements. We also examined what factors were associated with recommended follow-up care.
Methods
Design and Setting
We conducted a population-based, retrospective cohort study using linked health care databases within the Alberta Kidney Disease Network (AKDN). 19 More than 99% of Alberta residents are registered with Alberta Health and have universal access to hospital care and physician services. This study followed guidelines for observational studies (Table S1) and was approved by the research ethics boards at the Universities of Alberta and Calgary. A waiver of patient consent was granted.
Data Sources
We ascertained baseline characteristics, covariate information, and outcome data from the AKDN records (Table S2). The Alberta Health database contains information on demographics, vital statistics, and diagnostic and procedural information for inpatient and outpatient physician services. These data sources were linked to a provincial laboratory repository via unique, encoded, patient identifiers held by the AKDN. These databases have been previously used for research on health outcomes and services.20-22
Population
We identified all adult living kidney donors (≥18 years old) who underwent donor nephrectomy between May 1, 2002, and March 31, 2014, in Alberta, Canada (Figure S1). Living kidney donors were identified using an algorithm of 1 diagnostic code for kidney donation (International Statistical Classification of Diseases, Tenth Revision, ICD-10: Z52.4) and 1 procedural code for kidney procurement or excision (Canadian Classification of Health Interventions, CCI: 1.PC.58, 1.PC.89, or 1.PC.91) (Table S2). Similar codes have been used in previous studies to identify living kidney donors and assess for perioperative events.23,24 We have validated this algorithm and found it to have a sensitivity of 97% and a positive predictive value of 90% compared with the gold standard of living kidney donor identification by the provincial tissue and organ agency and verification through manual perioperative chart review. 25 The date of nephrectomy served as the start date for follow-up (index date). We excluded out-of-province donors and a small proportion of donors (<3%) with errors in their records (eg, missing sex or date of birth, date of death prior to nephrectomy).
Baseline Characteristics
Baseline demographics, including age and sex, were determined from Alberta Health administrative data files. Indigenous race/ethnicity was retrieved from the registry file. It was not possible to identify other race/ethnic groups, although more than 85% of the Alberta population is white. Postal codes were linked to the Canadian Census using the Postal Code Conversion file to determine median neighborhood household income quintile (level 5 being the highest) as well as rural versus urban location of residence and distance from the transplant center, as previously described.26,27 The presence of 1 or more diagnostic codes in the 3 years prior to the index date was used to identify comorbidities using validated International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and ICD-10 coding algorithms applied to physician claims and hospitalization data.28,29 Hypertension was identified from hospital discharge records and physician claims based on a validated algorithm.30,31 Demographic data were complete except for income quintile (0.4% missing).
Outcomes
The primary outcome was evidence of KDIGO guideline-concordant care as defined by annual outpatient physician visits, serum creatinine measurements, and albuminuria measurements in every year (±6 months of the anniversary date) following kidney donation. 12 We did not consider physician visits or laboratory values in the first 6 months after donation, as these are usually related to postoperative monitoring. Urinalysis, urine protein-creatinine ratio (PCR) measurement, or urine albumin-creatinine ratio (ACR) measurement qualified as albuminuria measurements in any given year. We also assessed the proportion of donors who met all 3 criteria in ≥75% of years of their observed follow-up, ≥50% of years of follow-up, and in no years of follow-up. We assessed trends in follow-up care over the first decade following donation. In additional analyses, we examined the components of the primary outcome (physician visits, serum creatinine measurements, albuminuria measurements) individually.
Statistical Analyses
Donors were followed from their index date (date of donor nephrectomy) until the first of death, development of ESRD (defined as chronic dialysis or transplantation), emigration from the province, end of last full year of available follow-up, or end of study period (March 31, 2015). We compared baseline characteristics of donors with guideline-concordant follow-up care versus donors without using χ2 or Fisher exact tests and Kruskal-Wallis tests. Associations of guideline-concordant follow-up care with donor demographic, socioeconomic, and comorbidity covariates were assessed using multivariable logistic regression (adjusted odds ratio). Statistical analyses were performed using Stata MP 13.1 (Stata Corporation, College Station, TX). A value of P < .05 was used to define statistical significance.
Results
Baseline Characteristics
There were 534 living kidney donors in Alberta between 2002 and 2014 who were included in the study (Figure S1). The median age at the time of donation was 41 years (interquartile range [IQR], 33-50) and 62% of donors were women (Table 1). Most donors resided in urban areas (88%) and within 50 km of the transplant center (59%). As expected, in the year prior to donation, donors had multiple physician visits (median, 7; IQR, 4-9), serum creatinine measurements (median, 3; IQR, 2-4), and albuminuria measurements (median, 5; IQR, 3-7). The median predonation estimated glomerular filtration rate (eGFR) was 100 mL/min/1.73 m2 (IQR, 88-113) and 90% of donors had none or very mild predonation proteinuria. At the time of donation, 12% of donors had a history of hypertension and 15% had a history of depression.
Baseline Characteristics of All Living Kidney Donors at the Time of Donor Nephrectomy and a Comparison Between Those With and Without Guideline-Concordant Follow-up Care. a
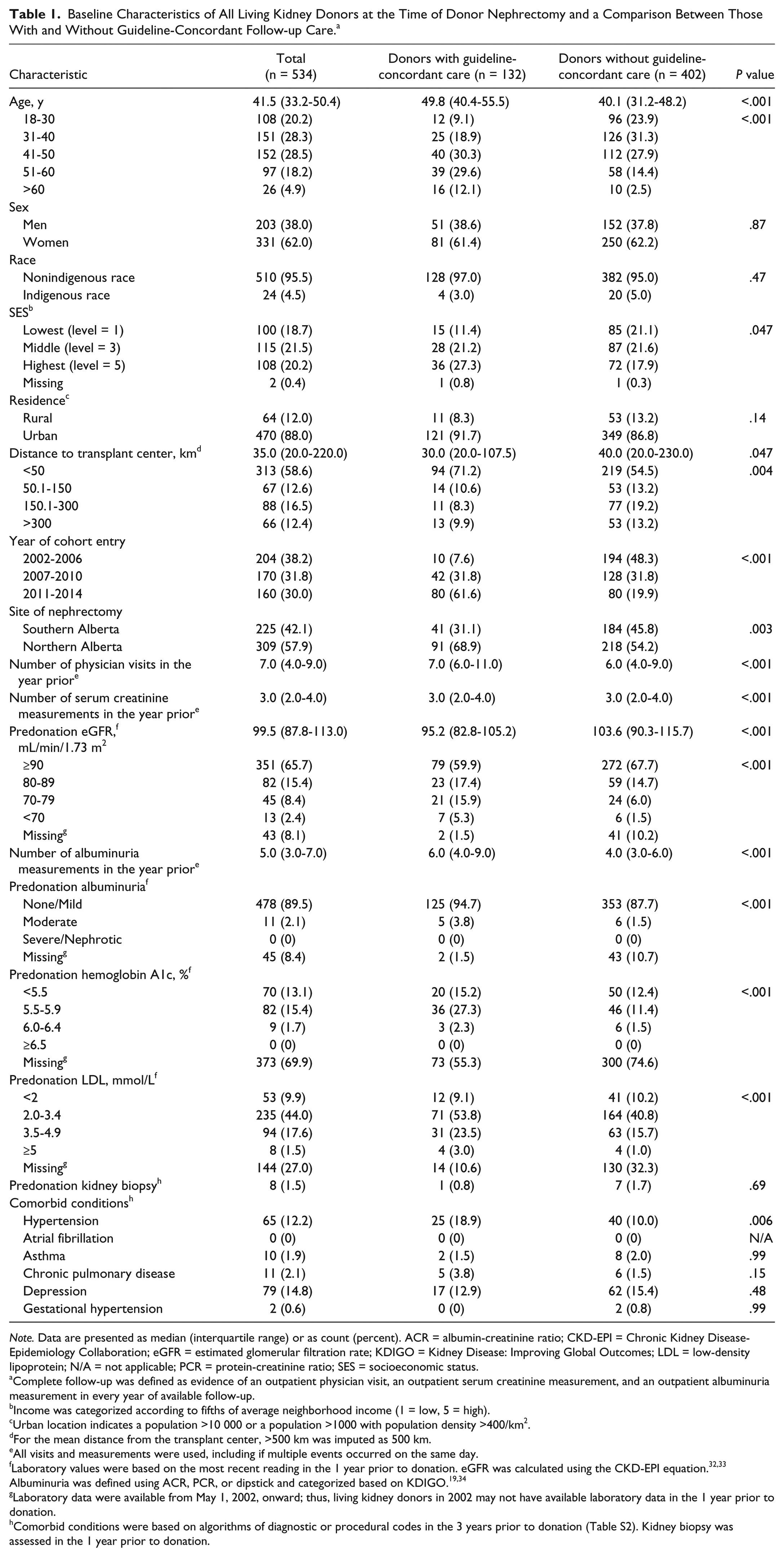
Note. Data are presented as median (interquartile range) or as count (percent). ACR = albumin-creatinine ratio; CKD-EPI = Chronic Kidney Disease-Epidemiology Collaboration; eGFR = estimated glomerular filtration rate; KDIGO = Kidney Disease: Improving Global Outcomes; LDL = low-density lipoprotein; N/A = not applicable; PCR = protein-creatinine ratio; SES = socioeconomic status.
Complete follow-up was defined as evidence of an outpatient physician visit, an outpatient serum creatinine measurement, and an outpatient albuminuria measurement in every year of available follow-up.
Income was categorized according to fifths of average neighborhood income (1 = low, 5 = high).
Urban location indicates a population >10 000 or a population >1000 with population density >400/km2.
For the mean distance from the transplant center, >500 km was imputed as 500 km.
All visits and measurements were used, including if multiple events occurred on the same day.
Laboratory values were based on the most recent reading in the 1 year prior to donation. eGFR was calculated using the CKD-EPI equation.32,33 Albuminuria was defined using ACR, PCR, or dipstick and categorized based on KDIGO.19,34
Laboratory data were available from May 1, 2002, onward; thus, living kidney donors in 2002 may not have available laboratory data in the 1 year prior to donation.
Comorbid conditions were based on algorithms of diagnostic or procedural codes in the 3 years prior to donation (Table S2). Kidney biopsy was assessed in the 1 year prior to donation.
Guideline-Concordant Care
During the study period, 0.8% of donors died, 0.2% developed ESRD, and 4% of donors emigrated from the province. Over a median follow-up of 7 years (IQR, 3-10, maximum 13 years), 25% (n = 132) of living kidney donors had complete follow-up care, defined as a physician visit, serum creatinine measurement, and albuminuria measurement in each year of available follow-up. Donors with complete follow-up care were more likely to be older, have higher income status, resided closer to the transplant center, have a history of predonation hypertension, and receive their nephrectomy in more recent years compared with donors without complete follow-up (Table 1). Donors with complete postdonation follow-up also had more predonation physician visits and less missing predonation serum creatinine and albuminuria measurements in the year prior.
There were 31% of donors who met all 3 criteria in ≥75% of their years of follow-up and 53% in ≥50% of their years of follow-up (Table 2). Sixty-seven percent of donors saw a physician in each year of follow-up, and the majority of these visits were to primary care physicians. A total of 31% of donors had serum creatinine measurements annually, whereas only 28% had an albuminuria measurement annually. Interestingly, almost 20% of donors never had guideline-concordant care, and a small, but sizable proportions of patients had no evidence of an outpatient physician visit (6%), never had a serum creatinine measurement (12%), or never had a measure of urine albumin excretion (15%) after donation.
Proportion of Donors (n = 534) Who Have Evidence of Guideline-Concordant Follow-up Care.

In the years following donation, the proportion of donors achieving guideline-concordant follow-up steadily declined due to the decrease in serum creatinine and albuminuria monitoring (Figure 1), whereas the proportion of donors seeing an outpatient physician remained constant. At 2 years, 50% of donors had all 3 markers of care (87% had a physician visit, 61% had a serum creatinine measurement done, and 55% had an albuminuria measurement performed).

Proportion of donors who have evidence of follow-up care during each postdonation year.
For the 98 donors who had at least 10 years of follow-up, 35% had all 3 markers of care performed in their 10th year after donation (83% had a physician visit, 54% had a serum creatinine measurement done, and 38% had an albuminuria measurement performed).
Predictors of Guideline-Concordant Care
After multivariable adjustment for predonation baseline characteristics, each increase in year of donor age at the time of donation was associated with a 7% higher likelihood of guideline-concordant care (Table 3). Every 10 km increase in distance to the transplant center was associated with a 2% lower likelihood of guideline-concordant care. We also observed a center effect as donors who underwent nephrectomy in the Northern Alberta program were 3 times more likely to achieve complete follow-up care, compared with donors who underwent nephrectomy in the Southern Alberta program. Compared with donors who underwent nephrectomy earlier in the study, donors from more recent years were more likely to achieve complete follow-up. For example, 23% of persons who donated in the year 2007-2010 had guideline-concordant care 5 years after donation, compared with 8% of persons who donated in the year 2002-2006. After adjustment, there was no significant correlation between sex, income status, predonation eGFR, or history of hypertension and guideline-concordant care.
Adjusted Associations of Baseline Characteristics With Guideline-Concordant Follow-up Care. a

Note. CI = confidence interval; eGFR = estimated glomerular filtration rate; SES = socioeconomic status.
Guideline-concordant follow-up care was defined as evidence of an outpatient physician visit, an outpatient serum creatinine measurement, and an outpatient albuminuria measurement (urine dipstick, albumin-creatinine ratio, or protein-creatinine ratio) in every year of available follow-up.
Data are presented as adjusted odds ratio (95% CI). Adjusted for age, sex, indigenous race, SES, residence, distance to transplant center, year of cohort entry, site of nephrectomy, predonation eGFR, predonation albuminuria, predonation hemoglobin, hypertension, asthma, chronic pulmonary disease, and depression.
Donors with missing income data (n = 2) were reclassified in the middle quintile for these analyses.
Discussion
Alberta, Canada, has the third highest living donor rate in the country (~20 per million population). 35 In this population-based study of living kidney donors, we found that only 25% of donors in Alberta received guideline-concordant care and that, in adjusted analyses, complete and consistent follow-up was associated with older age, closer proximity to the transplant center, and more recent date of nephrectomy.
Previous guideline recommendations on postdonation follow-up care are ungraded and based on expert opinion, as there was insufficient evidence available to ground evidence-based recommendations.11,12 Our study reports that only one-quarter of donors are receiving guideline-concordant care. The majority of donors appear to have regular follow-up with a physician, but recommended testing is only being done in a minority. To meet the best practice of care recommendations, our study highlights that we should focus on improving renal function monitoring.
Follow-up care may result in the prevention, early detection, and management of diseases. One systematic review reported that in the general population, annual preventive examinations had a consistently beneficial association with delivery of recommended preventive services and reductions in patient uncertainty and worry. 36 More recently, the Canadian Task Force on Preventive Health Care has challenged the utility of annual physical examination in the general population.37,38 In living kidney donors, early detection and treatment of conditions that are known to affect kidney function may protect them from further loss of kidney function and other complications related to low GFR.
Ongoing follow-up care also provides an opportunity to inform and educate living kidney donors on new research on long-term outcomes and complications. Recent evidence suggests that compared with healthy nondonor controls, the relative risk of ESRD may be higher in living kidney donors (adjusted hazard ratio, 11.4).5,7,8 However, the 15-year absolute risk of ESRD is low (15-year incidence 0.2%-0.5%).5,6,39-41 Living kidney donors may have a higher risk of gout compared with healthy matched nondonors, and female donors may have a higher risk of gestational hypertension or preeclampsia compared with matched nondonors, although the vast majority of women have normal healthy pregnancies after donation.9,10,42
Follow-up care also allows for continued monitoring of the overall health status and psychosocial well-being of living kidney donors. While the donor evaluation process can involve frequent testing and appointments with the transplant center, the postdonation care involves minimal, if any, contact. This can leave donors with a sense of abandonment after undergoing an altruistic procedure to save the life of another without any medical benefit to themselves. In interviews with living kidney donors on their follow-up experiences, 1 donor said, “Nobody cared for me any longer. Before the operation everybody was on his toes for me.” 43
Unfortunately, there are barriers to follow-up for living kidney donors, including sociodemographic and geographic factors, perception of unnecessary need for follow-up due to excellent donor health, unreimbursed costs, and limited resources and personnel.13,44-46 In our study, after adjustment for various factors, we found that donors who were older, resided closer to the transplant center, and donated more recently were more likely to achieve complete and consistent postdonation follow-up. We also found a center effect, as donors who underwent nephrectomy in 1 program were 3 times more likely to achieve complete follow-up care, compared with donors in another program. A better understanding of the barriers and facilitators that affect local practices regarding donor follow-up may help transplant centers develop strategies and policies to improve follow-up rates for their donors.
A few countries have instituted systematic approaches to long-term living donor follow-up that may serve as models. The European Living Donation and Public Health project mandates living donor registration and follow-up data collection through a centralized database and performs regulatory audits at the national and center level. 47 Similarly, the Swiss Living Donor Health Registry coordinates distribution of a health questionnaire and tubes for blood and urine samples and asks donor to make an appointment with the family physician at 1 year and then biennially thereafter. 48 In 2017, the US Scientific Registry of Transplant Recipients began a “Living Donor Collective” pilot project that seeks to achieve lifelong living donor follow-up through direct contacts by staff and novel data linkages. 49 Center-based initiatives to provide long-term donor follow-up and support through integrated clinical and laboratory monitoring, expansion of preventive health strategies, and fostering of peer education through social support networks between past, current, and future donors are also being tested. 50
Our findings fill an important knowledge gap in the existing literature. 12 To date, this is one of the largest, most comprehensive studies of real-world living kidney donor follow-up care that reports rates of physician visits, serum creatinine testing, and albuminuria testing. 51 Our results may not be generalizable to other countries or regions that do not have a similar universal health care system. Given its observational nature, the possibility of residual confounding must also be considered. We lacked data on certain baseline characteristics such as smoking, blood pressure control, and body mass index, as well as transplant-related characteristics, such as donor-recipient relationship. However, we were able to identify and control for important demographics and comorbidities commonly associated with follow-up care. We also looked at outpatient physician visits as a surrogate for blood pressure measurements, and other markers of care, including assessment of body weight and preventive health delivery. We are unable to confirm that these services were delivered and whether the lack of serum creatinine and albuminuria measurement was due to physician or patient decisions.
Although our study found that only one-quarter of donors are currently receiving the postdonation follow-up care recommended by best practice guidelines, we are reassured that the majority of donors continued to see a physician on an annual basis. This suggests that donors and their physicians should be counseled on the importance of renal health surveillance and that a framework of contact for such surveillance is in place. Further research is needed to determine whether routine follow-up of living kidney donors, who are generally of excellent health at donation, actually mitigates long-term risks and complications. Ensuring timely and adequate follow-up for living kidney donors is an internationally recognized priority aimed at protecting donors and ensuring the integrity, quality, and safety of organ donation. 12
Supplemental Material
LKD_Follow-up_-_Appendix_-_20180226 – Supplemental material for Follow-up Care of Living Kidney Donors in Alberta, Canada
Supplemental material, LKD_Follow-up_-_Appendix_-_20180226 for Follow-up Care of Living Kidney Donors in Alberta, Canada by Ngan N. Lam, Krista L. Lentine, Brenda Hemmelgarn, Scott Klarenbach, Robert R. Quinn, Anita Lloyd, Sita Gourishankar and Amit X. Garg in Canadian Journal of Kidney Health and Disease
Footnotes
List of Abbreviations
ACR, albumin-creatinine ratio; AKDN, Alberta Kidney Disease Network; CCI, Canadian Classification of Health Interventions; eGFR, estimated glomerular filtration rate; ESRD, end-stage renal disease; GFR, glomerular filtration rate; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; ICD-10, International Statistical Classification of Diseases, Tenth Revision; IQR, interquartile range; KDIGO, Kidney Disease: Improving Global Outcomes; PCR, protein-creatinine ratio; UNOS, United Network for Organ Sharing.
Ethics Approval and Consent to Participate
This study was approved by the institutional review board at the University of Alberta and the University of Calgary.
Consent for Publication
All authors consent for publication.
Availability of Data and Materials
Additional data is available in the Appendix.
Authors’ Note
This study is based in part on data provided by Alberta Health and Alberta Health Services. The interpretation and conclusions contained herein are those of the researchers and do not necessarily represent the views of the Government of Alberta or Alberta Health Services. Neither the Government of Alberta nor Alberta Health or Alberta Health Services express any opinion in relation to this study.
Author Contributions
N.N.L. conceived the study and drafted the manuscript. A.L. performed the statistical analyses and created the figure. All authors interpreted the results, revised the manuscript, and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Canadian Institutes of Health Research (CIHR) Project Grant and a University Hospital Foundation Medical Research Competition grant. N.N.L. was supported by a KRESCENT New Investigator Award. S.K. was supported by the Kidney Health Research Chair and the Division of Nephrology at the University of Alberta. A.X.G. was supported by a Clinician Investigator Award from the Canadian Institutes of Health Research and the Dr. Adam Linton Chair in Kidney Health Analytics.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.