
Abstract
Background:
Survivors of acute kidney injury (AKI) are at risk of adverse outcomes. Post-discharge nephrology care may improve patients’ AKI knowledge and prevent post-AKI complications.
Objective:
The purpose of this study was to examine patients’ awareness about their AKI diagnosis and self-rated knowledge and severity of AKI before and after their first post-discharge AKI Clinic encounter.
Design:
We conducted a pre- and post-survey study among AKI survivors who attended a post-discharge AKI Clinic.
Setting:
AKI Clinic at the University of Kentucky Medical Center (October 2016 to December 2017). Education about AKI was based on transformative learning theory and provided through printed materials and interdisciplinary interactions between patients/caregivers and nurses, pharmacists, and nephrologists.
Patients:
A total of 104 patients completed the survey and were included in the analysis.
Measurements:
Three survey questions were administered before and after the first AKI Clinic encounter: Question 1 (yes-no) for awareness, and questions 2 and 3 (Likert scale, 1 = lowest to 5 = highest) for self-rated knowledge and severity of AKI.
Methods:
Two mixed-model analysis of variance (ANOVA) was used for between-group (AKI severity) and within-group (pre- and post-encounter) comparisons. Logistic regression was used to examine parameters associated with the within-group change in self-perceived knowledge.
Results:
Twenty-two out of 104 (21%) patients were not aware of their AKI diagnosis before the clinic encounter. Patients’ self-ratings of their AKI knowledge significantly increased after the first AKI Clinic encounter (mean ± SEM: pre-visit = 1.94 ± 0.12 to post-visit = 3.88 ± 0.09, P = .001), even after adjustment for age, gender, Kidney Disease Improving Global Outcomes (KDIGO) severity stage, or poverty level. Patients with AKI stage 3 self-rated their AKI as more severe than patients with AKI stage 1 or 2.
Limitations:
Our study population may not be representative of the general AKI survivor population. Administered surveys are subject to response-shift bias.
Conclusions:
Patients’ self-perceived knowledge about AKI significantly increased following the first post-discharge AKI Clinic encounter that included interdisciplinary education. This is the first survey study examining self-perceived AKI knowledge in AKI survivors. Further examination of AKI literacy in survivors of AKI and its effect on post-AKI outcomes is needed.
Trial registration:
Not applicable.
What was known before
To our knowledge, this is the first pre- and post-survey study examining awareness and self-perceived acute kidney injury (AKI) knowledge in survivors of AKI followed in a specialized AKI Clinic, in which interdisciplinary educational interventions were implemented.
What this adds
The results of this study highlight patients’ AKI knowledge as a potential modifiable intervention in survivors of AKI. Our study may also have implications for what educational maneuvers should physicians target when evaluating survivors of AKI.
Introduction
Acute kidney injury (AKI) occurs in approximately 20% of hospitalized patients, and the incidence doubles in patients admitted to intensive care units.1,2 Acute kidney injury carries high morbidity and mortality and adversely influences hospital resource utilization and health care costs,3,4 particularly in critically ill patients in whom mortality rates are as high as 50%.4,5 Post-AKI complications are also common and include the development or progression of chronic kidney disease (CKD),6-9 hypertension, 10 and cardiovascular disease.11-14 Acute kidney injury survivors are also susceptible to early rehospitalization and an overall increased risk of long-term mortality.15,16
Although AKI survivors are at high risk of several multiorgan complications, only a minority of them are evaluated by a nephrologist within the first 3 months of hospital discharge.17-19 Furthermore, there are only few specialized AKI Clinics dedicated to following AKI survivors post-discharge.20-22 In this context, there is paucity of research dedicated to examine and/or promote AKI literacy in AKI survivors. Most importantly, there are no standardized or validated educational tools or interventions to enhance AKI knowledge in this susceptible population. Improving patients’ knowledge about their AKI diagnosis is a cornerstone of post-AKI care and may be essential to promote kidney recovery and prevent recurrent episodes of AKI or the development of CKD.
The purpose of this study was to examine patients’ awareness about their AKI diagnosis and patients’ self-rated AKI knowledge before and after their participation in a specialized post-discharge AKI Clinic that has developed and implemented educational tools to promote AKI knowledge throughout the encounter experience. We hypothesized that most of the patients who attend the AKI Clinic are aware of their AKI diagnosis and that the overall experience during the AKI Clinic visit will significantly improve their self-perceived knowledge about AKI, particularly in those who suffered from severe AKI.
Methods
Study Design
We conducted a survey study to examine AKI awareness and self-rated AKI knowledge in AKI survivors followed in a specialized post-discharge AKI Clinic. The same survey questions were completed before and after the first AKI Clinic visit. A total of 113 patients were evaluated in the post-discharge AKI Clinic from October 2016 to December 2017 at the University of Kentucky Medical Center. Of these, 104 (92%) completed the survey examination and were included in the study (Figure 1). The study was approved by the institutional review board (IRB) of the University of Kentucky (IRB: 17-0471-P2H).

Patient selection for survey examination.
AKI Clinic: Description
Acute kidney injury survivors were defined as patients who have achieved clinical stability and were discharged from the hospital, irrespective of their degree of kidney recovery. 18 The post-discharge AKI Clinic was established at the University of Kentucky Medical Center in October of 2016 following the model described by Silver and colleagues. 22 The main goal of the AKI Clinic was to evaluate kidney recovery in AKI survivors during the first 90 days post-discharge as this may be informative for their subsequent risk of recurrent AKI or incident/progressive CKD or end-stage renal disease (ESRD).23,24 The post-discharge AKI Clinic comprises an interdisciplinary team of nurses, pharmacists, physician assistants, nephrologists and ancillary staff, and has standard operating procedures that include structured follow-up (Supplementary Figure 1) and AKI education for patients and caregivers (Figure 2).
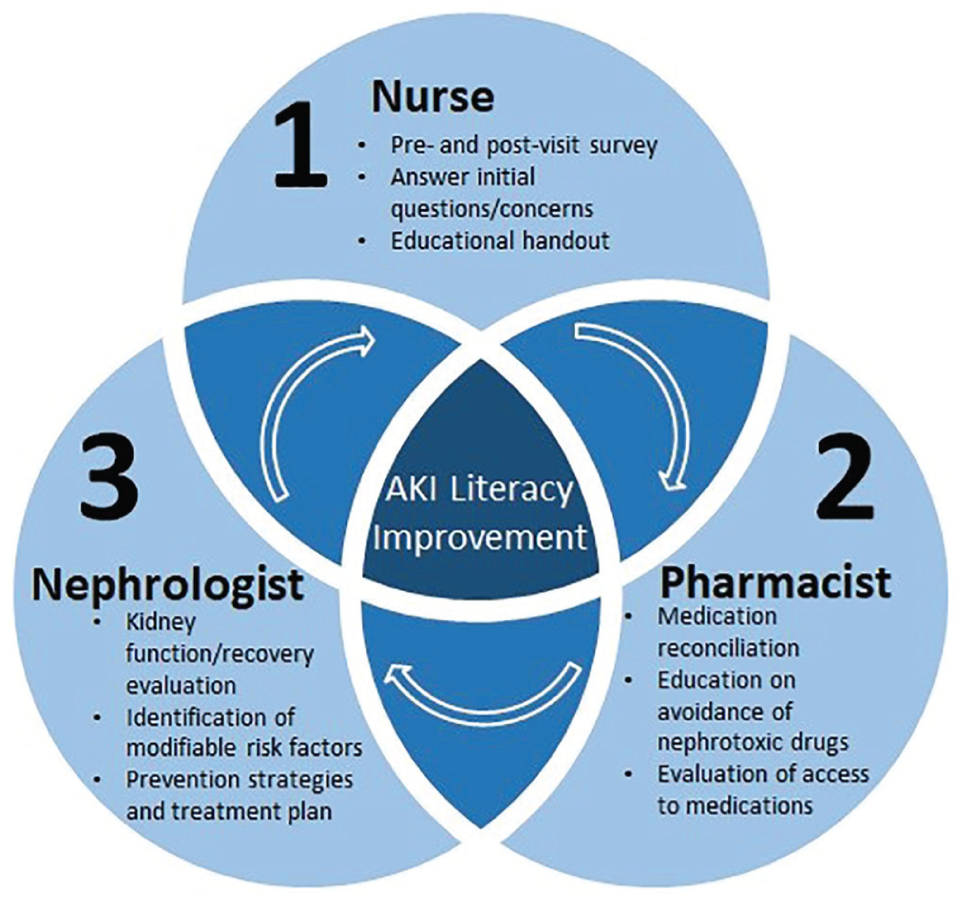
Interdisciplinary educational procedures performed in the Acute Kidney Injury Clinic.
AKI Clinic: Target Patient Population
We use the following referral criteria for follow-up in the AKI Clinic:
Inclusion criteria:
All patients diagnosed with severe AKI (Kidney Disease Improving Global Outcomes [KDIGO] stage 2 or 3) 25 during a recent hospitalization. Occasionally, patients with AKI stage 1 were evaluated in the AKI Clinic at the request of the inpatient nephrology consulting team
Exclusion criteria:
Baseline estimated glomerular filtration rate (eGFR) <15 mL/min/1.73 m2
Kidney transplant recipients
Persistent requirement for outpatient hemodialysis at the time of hospital discharge
AKI Clinic: Referral Process and Structured Follow-up Visits
Our AKI Clinic staff received referrals mostly coming from inpatient nephrology consult teams at the time of signing off. The first AKI Clinic visit was targeted to occur 4 to 6 weeks after hospital discharge. Subsequent visits were scheduled at 3, 6, 12, and 18 months as outlined in the Supplementary Figure 1. After the fifth visit, the nephrologist evaluated the patient’s kidney function status and determined whether the patient required referral to the CKD Clinic or if routine follow-up with his or her primary care provider would suffice.
AKI Clinic: Education Procedures
The education procedures were conducted during the entire clinical encounter and were based on transformative learning theory 26 (critical reflection to challenge the learner’s beliefs and assumptions). The first educational interaction (nurse-patient, 10-15 minutes) occurred at the time of room boarding: (1) The nurse asked the patient about his or her understanding of AKI using terms such as “acute kidney injury,” “acute kidney failure,” “kidney damage,” “kidney disease,” “sick kidneys,” and so on and through open questions and self-reflection of their recent hospital experience (dissonance phase: recognize what is unknown); (2) the nurse provided an educational handout containing information about AKI for the patient to review. The handout material is accessible through the National Kidney Foundation website (Supplementary Figure 2) 27 and includes information about the following: What is AKI? What are the most common causes of AKI? What are the consequences of AKI? What should you do to protect your kidneys after an episode of AKI? The second educational interaction (pharmacist-patient, 10-15 minutes; organization phase) consisted of (1) review of patients’ medication list; (2) review of use of over-the-counter supplements, pain control medications, or herbal remedies; and (3) education regarding common nephrotoxic drugs (ie, nonsteroidal anti-inflammatory agents) and the importance to avoid these medications in the recovery phase of AKI. The final and third educational interaction (physician or physician assistance-patient, 20-25 minutes) included a comprehensive review of AKI etiology and characteristics, patient- and hospitalization-specific risk factors, and the identification of modifiable risk factors that can potentially prevent new episodes of AKI and/or complications from AKI. During this final interaction (feedback and consolidation phases), all patients’ and/or caregivers’ questions related to preventive maneuvers and treatment plan were addressed and answered. A summary of our educational interventions is provided in Table 1.
Educational Intervention About AKI Focusing on Three Main Domains.
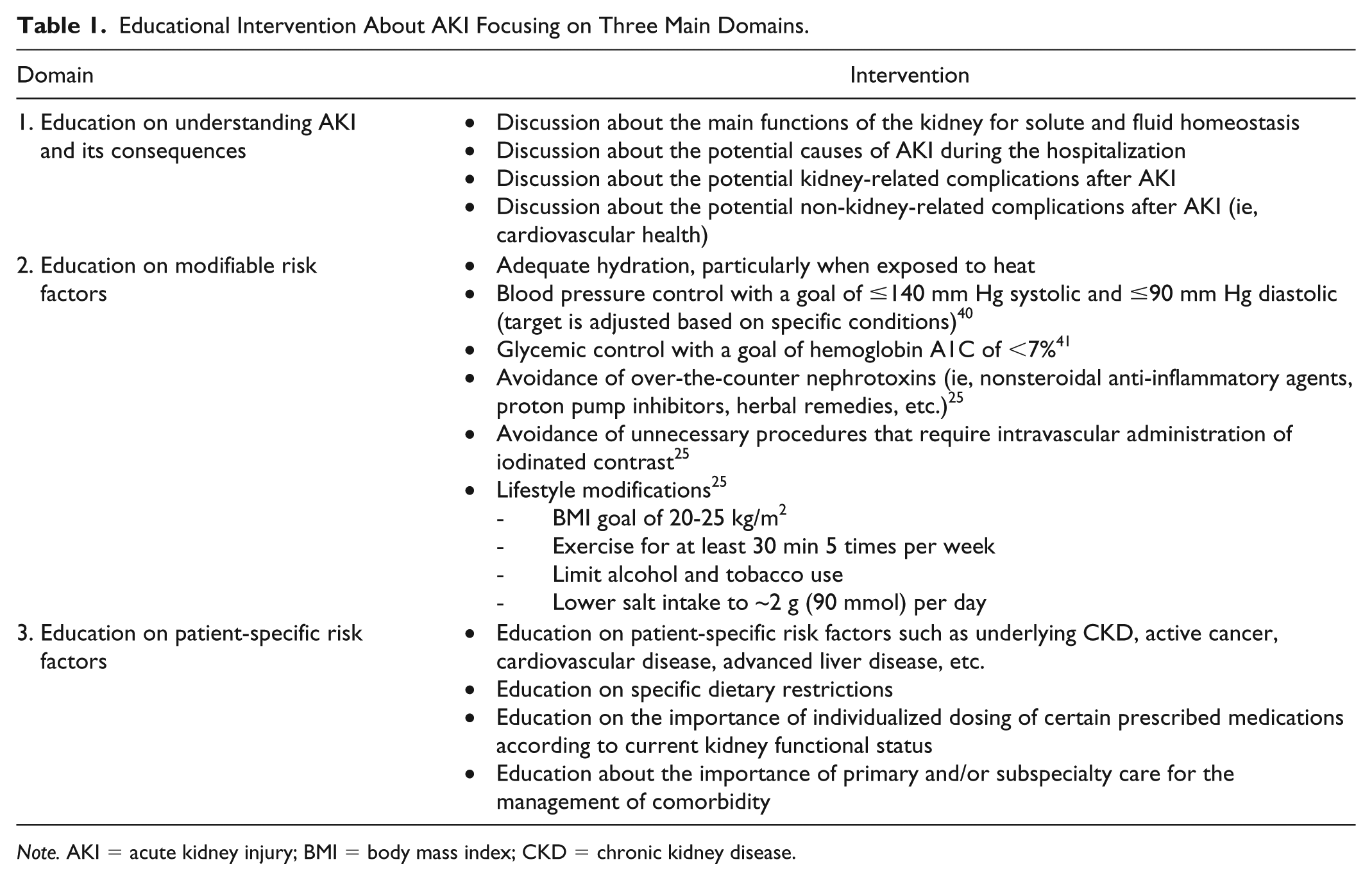
Note. AKI = acute kidney injury; BMI = body mass index; CKD = chronic kidney disease.
AKI Clinic: Survey Examination
The survey was part of the standard-of-care operations of the AKI Clinic and was administered by the ancillary staff before and after the first clinic encounter. The person in charge of administering the survey was not directly involved in the educational procedures to minimize response-shift bias. The survey consisted of 3 questions to determine awareness about the AKI diagnosis, to determine self-rated knowledge about AKI, and to determine self-rated severity of AKI. If the patient answered “NO” to the first (awareness) question, we assigned the lowest score to the following 2 questions for the pre-encounter time point. The ancillary staff was trained to use alternative terms to “acute kidney injury” such as “acute kidney failure,” “kidney damage,” “kidney disease,” “sick kidneys,” and so on when appropriate during the administration of the survey.
Clinical Data and Definitions
We collected demographic, comorbidity, and social history data from chart review. Poverty level was defined as the percentage of people whose income in the past 12 months is below the poverty level of their area of residence. We determined poverty level according to the postal code of residence for each patient. We used poverty level as a surrogate metric of patients’ educational level. Baseline serum creatinine (SCr) was defined as the outpatient SCr value closest to the day of hospital admission during the 6 months before the date of hospitalization. 25 If unavailable, the lowest SCr throughout the AKI hospitalization was recorded as the baseline SCr. The duration of AKI was defined as the period from AKI diagnosis to the improvement (decrease) in SCr of at least 50% from the peak value. The AKI recovery was determined if there was less than 25% eGFR reduction from baseline at the time of first AKI Clinic encounter. 28 We used Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) 29 equation for calculating eGFR. We defined improvement of self-rated knowledge of AKI as an increase of ≥1 versus <1 points from pre- to post-clinic encounter in the applied survey scale. This variable was then examined as a binary outcome.
Statistical Analysis
Data are reported as mean (SD) or median (IQR) for continuous variables or frequency and percentage for categorical variables. The AKI KDIGO SCr-criteria
25
were used to create groups based on AKI severity. One-way analysis of variance (ANOVA) was used to compare continuous variables across AKI severity groups. Chi-square analyses were conducted to compare categorical variables across groups. Two mixed-model ANOVAs were used to analyze patients’ self-rated knowledge about AKI and self-rated severity of their AKI. We used post hoc comparison with Bonferroni correction to analyze the mean self-rated knowledge and severity of AKI. The independent variables in both mixed-model ANOVAs were AKI stage groups (ie, stages 1 and 2, stage 3, and stage 3-RRT [renal replacement therapy]; between-subjects factor) or AKI recovery groups (YES/NO; between-subjects factor) and time point (pre- and post-AKI Clinic encounter; within-subjects factor). Patients’ self-rated knowledge and severity was the dependent variable for the mixed-model ANOVAs. Planned post hoc comparisons following significant main or interaction effects were conducted with Sidak correction for both mixed-model ANOVAs. Effect sizes for significant results were calculated as partial eta squared (
Finally, multivariable logistic regression models for awareness of AKI diagnosis and improvement in self-rated knowledge of AKI (from pre- to post-AKI Clinic encounter) as dependent variables were constructed. The AKI severity (stage 3 or 3-RRT vs stage 1 or 2) and AKI recovery status were the main independent variables. Covariates forced into the models were age, gender, Charlson comorbidity score, 30 and poverty level. These covariates were selected based on clinical rationale or univariate analysis. The model was tested by the Hosmer and Lemeshow goodness-of-fit test. Statistical analyses were performed in SPSS Version 22 (IBM Corporation, Armonk, New York) and SAS 9.4 (SAS Institute, Cary, North Carolina) with an alpha level set at P ≤ .05 (2-tailed) for all comparisons.
Results
Patients’ Characteristics
A total of 113 patients were followed in the AKI Clinic from October 2016 through December 2017. Of these, 104 patients completed the survey and were included in the analysis (Figure 1). The mean (SD) patient age was 55.1 (13.8) years, 50% were male, and 88.5% were white. The median (IQR) length of hospitalization was 13 (7-20) days. The median (IQR) time between hospital discharge and the first AKI Clinic encounter was 28 (13-45) days. Our cohort consisted of 9 (8.7%) patients with AKI stage 1, 10 (9.6%) with AKI stage 2, 50 (48.1%) with AKI stage 3, and 35 (33.6%) with AKI stage 3-RRT. A total of 88 (84.6%) of patients had inpatient nephrology consultation for AKI management. Patients’ characteristics according to AKI severity stages are reported in Table 2.
Patient Characteristics.

Note. AKI = acute kidney injury; RRT = renal replacement therapy; IQR = interquartile range; eGFR = estimated glomerular filtration rate; SCr = serum creatinine; ATN = acute tubular necrosis.
Patients’ Awareness About AKI Diagnosis
At the beginning of the first AKI Clinic encounter, 22 (21.2%) patients were not aware of their AKI diagnosis: 6 out of 10 (60%) patients with AKI stage 1, 3 out of 9 (33.3%) patients with AKI stage 2, 10 out of 50 (20%) patients with AKI stage 3, and 3 out of 35 (8.5%) patients with AKI stage 3-RRT. Patients with AKI stage 3 or 3-RRT were more aware of their AKI diagnosis than those with AKI stage 1 or 2, even after adjustment for age, gender, Charlson score, and poverty level (adjusted odds ratio [OR] = 3.74, 95% confidence interval [CI] = 1.07-13.12, P = .038) (Table 3). Fifty-five patients (52.9%) recovered at least 75% of kidney function relative to baseline by the time of their first visit to the post-discharge AKI Clinic. The pre-visit awareness of AKI was not associated with AKI recovery status (P = .93) (Table 3). After the first AKI Clinic encounter, all patients were aware of their recent AKI diagnosis.
Multivariable Logistic Regression Models of Pre-Encounter Awareness of AKI Diagnosis and Improvement in Self-Rated Knowledge After the First AKI Clinic Encounter (Dependent Variables) and (a) AKI Severity (Stage 3 or 3-RRT vs Stage 1 or 2) and (b) AKI Recovery Status (No Recovery vs Recovery) as the Main Independent Variables.

Note. AKI = acute kidney injury; RRT = renal replacement therapy; OR = odds ratio; CI = confidence interval; eGFR = estimated glomerular filtration rate.
In reference to AKI stage 1 or 2.
In reference to AKI recovery, determined if there was less than 25% eGFR reduction from baseline at the time of first AKI Clinic encounter.
Patients’ Self-Rated Knowledge About AKI
Patients significantly improved their self-rated knowledge about AKI following the first AKI Clinic encounter as there was a significant main effect of time point, F(1, 91) = 160.94, P = .001,

Patients’ ratings of their self-rated knowledge before and after the first AKI Clinic encounter (mixed-model ANOVA, P = .001).
Patients’ Self-Rated Severity of Their AKI
Patients who had AKI stage 3-RRT self-rated their AKI as more severe than patients with AKI stage 3 or stages 1 and 2. Similarly, patients with AKI stage 3 self-rated their AKI as more severe than patients with AKI stages 1 and 2—main effect of AKI severity stage, F(2, 91) = 12.62, P = .001,
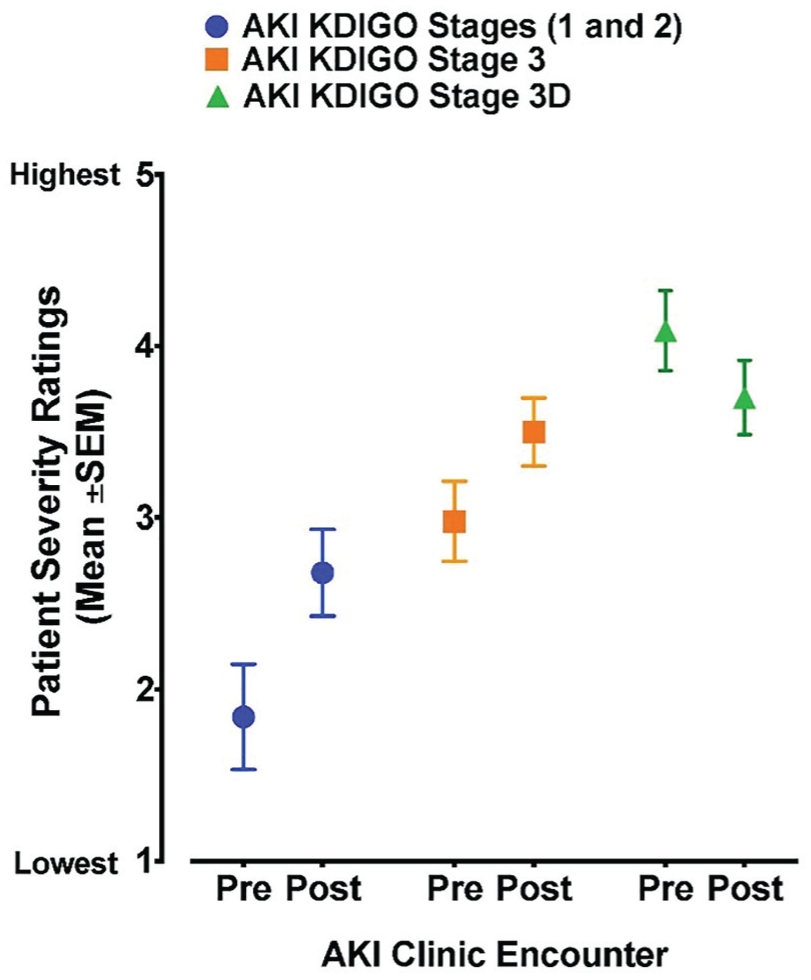
Patients’ ratings of their self-rated severity before and after the first AKI Clinic encounter (mixed-model ANOVA, P = .001).
Discussion
The principal finding of this study is that the implementation of AKI education throughout the first visit encounter in a specialized post-discharge AKI Clinic increased patients’ self-rated knowledge about AKI. Patients with more severe AKI were more likely to be aware of their AKI diagnosis before the first clinic encounter with the nephrologist. Importantly, almost one quarter of the patients did not know that they suffered from AKI. These findings are timely and critically important to aid the development of effective strategies to promote patients’ AKI knowledge, which may have a positive impact on the prevention or amelioration of post-AKI complications. We based our educational intervention on 3 main domains. The first one focused on patient’s understanding about AKI and its consequences. The second one consisted of the identification of modifiable risk factors, such as blood pressure and glycemic control, healthy lifestyle changes (ie, weight loss, tobacco cessation), and avoidance of over-the-counter nephrotoxins (ie, nonsteroidal anti-inflammatory agents). The third one focused on individualized preventive measurements according to specific patient’s needs such as underlying CKD and another comorbidity that can affect kidney health (ie, active cancer, chemotherapy, cardiovascular disease, advanced liver disease, etc.). This study constitutes the first step toward establishing and validating educational tools and strategies to improve knowledge about AKI in survivors of AKI.
AKI survivors are at significant risk for renal and cardiovascular complications, and frequent rehospitalizations.11-16 Despite this evolving evidence, only a few AKI survivors follow up with a nephrologist or primary care physician in the first few weeks after hospital discharge. 31 According to the 2013 report from the US Renal Data System, 13% of AKI survivors saw a nephrologist within 3 months of hospital discharge. 32 Siew et al 17 found that only 8.5% of AKI survivors received a referral to a see a nephrologist. Similarly, Harel et al 19 studied a cohort of 3877 hospitalized patients with AKI requiring RRT from 1996 to 2008 and found that only 40.8% visited a nephrologist within 90 days of hospital discharge. Patients who were referred to see a nephrologist (mean of 13 days from discharge to clinic visit) had a higher likelihood of having preexisting CKD, hypertension, and a nephrologist’s visit before the index hospitalization. Importantly, these patients had a lower rate of death compared with those without nephrology follow-up (8.4 vs 10.6 per 100-patients years, adjusted hazard ratio = 0.76, 95% CI = 0.62-0.93).
There are no well-established risk-stratification tools to identify AKI survivors who can benefit from specialized nephrology follow-up versus standard of care.7,33 These tools need to integrate more accurate assessment of kidney function and kidney functional reserve utilizing novel biomarkers, functional imaging studies, and possibly machine learning algorithms that provide information from available clinical data.34-36 Before these tools are fully developed and validated, it is reasonable to follow AKI survivors who suffered from severe AKI (KDIGO stage ≥2) or are suspected to be at high risk for recurrent AKI or progression to CKD. 31 The impact of specialized nephrology care in these patients may be critical to prevent or ameliorate post-AKI adverse outcome. However, the value of the AKI Clinic model needs to be further studied with properly designed interventional studies that focus not only on hard outcomes such as mortality, CKD, or ESRD but also on patient-centered outcomes including quality of life, cardiovascular comorbidity and cognitive function. 18 We believe that the barriers for optimal follow-up of AKI survivors include incomplete awareness of the multiple AKI consequences by the health care team and ineffective education maneuvers for patients and/or caregivers during the hospitalization.
Evolving evidence suggests that health literacy is essential in the care of patients with kidney disease. However, most of these studies have focused on CKD patients. Taylor et al 37 performed a systematic review to explore the association between health literacy and clinical outcomes in patients with CKD. They found that there is an association between inadequate CKD literacy and hospitalizations and cardiovascular events in nondialysis CKD patients, and with reduced dialysis adherence, hospitalizations, and mortality in dialysis patients. Importantly, health literacy examination tools were heterogeneous across studies limiting the reproducibility of the findings. Similarly, Devraj et al 38 described an association between health literacy and kidney function decline in CKD patients. They used the Newest Vital Sign (NVS) instrument to measure health literacy in a cohort of 150 patients with CKD stages 1 to 4 referred to an outpatient nephrology clinic. 39 They found that for every unit increase in the health literacy metric, there was a 2.2% increase in the eGFR during a follow-up of 5 months. The relationship between health literacy and improvement in eGFR remained significant after adjusting for gender and race but not after adjusting for age. This evolving evidence supports our hypothesis that improving the understanding of AKI and its consequences in survivors of AKI may have a positive effect on post-AKI outcomes. However, one should be cautious when extrapolating health literacy data from CKD patients into survivors of AKI with heterogeneous kidney recovery phenotypes, particularly because it is not known which high-risk subgroups of AKI survivors may benefit the most from dedicated educational interventions.
Our study has several strengths. First, this is the first survey study examining awareness and self-perceived AKI knowledge in survivors from AKI followed in a specialized AKI Clinic with standard educational interventions and structured follow-up. 22 Second, we utilized a survey that has external and constructs validity as patients with more severe forms of AKI had higher self-rated severity scores. Third, our study suggests that simple and replicable interdisciplinary educational interventions may improve self-rated patients’ knowledge about a complex syndrome such as AKI.
Our study also has limitations. First, administered surveys are subject to response-shift bias. However, we minimize this bias by not including the staff administering the survey in the educational procedures. Second, the survey employed for this study does not test the patient’s actual knowledge about AKI but rather self-rated knowledge about this condition. However, we consider that these data are critically informative to develop and validate educational tools for AKI survivors. Third, our study population may not be representative of the general AKI survivor population, as we had prespecified criteria for clinic referral and approximately 30% of all patients referred to the clinic did not attend the clinic.
Conclusion
Almost one quarter of the patients were not aware of the AKI diagnosis even after scheduling an appointment to follow in the post-discharge AKI Clinic. Patients’ self-rated knowledge about AKI significantly increased following the first AKI Clinic encounter in a specialized setting that incorporated simple and replicable educational maneuvers by an interdisciplinary team. Future studies should aim to validate standard educational interventions in AKI survivors and, most importantly, examine the relationship between AKI literacy and post-AKI outcomes in this susceptible population.
Supplemental Material
Supplementary_Figure_1_and_2 – Supplemental material for A Survey Study of Self-Rated Patients’ Knowledge About AKI in a Post-Discharge AKI Clinic
Supplemental material, Supplementary_Figure_1_and_2 for A Survey Study of Self-Rated Patients’ Knowledge About AKI in a Post-Discharge AKI Clinic by Victor Ortiz-Soriano, Joseph L. Alcorn, Xilong Li, Madona Elias, Taha Ayach, B. Peter Sawaya, Hartmut H. Malluche, Ron Wald, Samuel A. Silver and Javier A. Neyra in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors would like to extend their gratitude to the following members of the AKI Clinic team: Lauren Berry, Brook Sargent, Emily Wells, Abigail Hines, and Brian Armentrout.
Ethics Approval and Consent to Participate
Ethics approval was obtained from the University of Kentucky Institutional Review Board. Informed consent was waived for this study.
Consent for Publication
All authors reviewed the final manuscript and provided consent for publication.
Availability of Data and Materials
Data and materials may be made available upon written request to the corresponding author.
Author Contributions
V.O.S. and J.A.N. helped in study concept and design. V.O.S., J.L.A., M.E., and J.A.N helped in analysis and interpretation of data. V.O.S. and J.A.N. helped in drafting of the article. T.A., B.P.S., H.H.M., R.W., and S.A.S. helped in critical revision of the article for important intellectual content. J.L.A. and X.L. helped in statistical analysis. B.P.S., H.H.M., and J.A.N. helped in administrative, technical, and material support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Neyra is supported by an Early Career Pilot Grant from the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1TR001998 and the Kentucky Nephrology Research Trust. Dr. Alcorn was supported through Grant T32DA07304.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.