
Abstract
Glomerulonephritis (GN) is a common cause of end-stage renal disease in Canada and worldwide, and results in significant health care resource utilization and patient morbidity. However, GN has not been a traditional priority of provincial renal health care organizations, despite the known benefits to health services delivery and patient outcomes from integrated provincial care in other types of chronic kidney disease. To address this deficiency, the British Columbia (BC) Provincial Renal Agency created the BC GN Network in 2013 to coordinate provincial GN health services delivery informed by robust population-level data capture on all GN patients in the province via the BC GN Registry. This report describes the use of the BC GN Network infrastructure to systematically develop and evaluate a provincial GN drug formulary to improve patient and physician access to evidence-based immunosuppressive treatments for GN in a cost-efficient manner that successfully halted historical trends of increasing medication costs. An example is provided of using the provincial infrastructure to implement and subsequently evaluate an evidence-informed health policy of converting brand to generic tacrolimus for the treatment of GN. The BC GN Network, including the provincial drug formulary and data infrastructure, is an example of the benefits of expanding the mandate of provincial renal health administrative organizations to include the care of patients with GN, and constitutes a viable health delivery model that can be implemented in other Canadian provinces to achieve similar goals.
What was known before
The benefits of integrating a provincial health service model with administrative data capture in all-cause CKD are well established, however the application to glomecular diseases has not been studied.
What this adds
The BC GN network and its centralized drug formulary and data infrastructure demonstrate the benefits of expanding the mandate of provincial renal health administrations organizations to include glomerular diseases, and is a model that can be implemented in other Canadian provinces.
Introduction
Each year, over 2900 Canadians are diagnosed with glomerulonephritis (GN),1,2 of whom 20% to 80% will eventually progress to end-stage renal disease (ESRD) despite treatment with expensive immunosuppressive therapies that have substantial side effects and toxicity.3-8 Consequently, GN accounts for 16% to 22% of all ESRD in Canada and the United States,9,10 and results in significant patient morbidity and health care resource utilization.11-13 Despite the substantial burden of disease to patients and society, GN has not been a traditional priority of provincial health care organizations that target other types of kidney diseases, such as advanced all-cause chronic kidney disease (CKD) or ESRD. The benefits of integrating a provincial health services model with administrative data capture in all-cause CKD have been well established, including the ability to develop and subsequently evaluate effective health policies, and optimizing equitable, efficient, and cost-effective delivery of health care resources.14-17 Expanding the mandate of provincial renal health care organizations to specifically target glomerular diseases would be expected to convey similar benefits to the health outcomes and health care resource utilization of patients with GN.
The British Columbia (BC) GN Network is an initiative of the BC Provincial Renal Agency that was created in 2013 to address the deficiency of GN-focused health services delivery in BC. 18 A major goal of the Network is to use the analysis of local BC data to develop evidence-based health policies that are financially sustainable and improve the care of patients with GN (see Table 1). The BC GN Registry was created in this regard as the data infrastructure capable of informing health policy development and implementation, and uses existing administrative databases to prospectively capture population-level clinical, histological, and outcome data on all patients with GN in BC as of the time of kidney biopsy. 18 At the time the GN Network was created, a national survey reported that 83% to 86% of Canadian nephrologists had poor access to insurance coverage for immunosuppression (IS) medications for the treatment of GN, and felt that centralized provincial funding for IS medications would improve patient care. 19 There was therefore a unique opportunity for the GN Network to develop health policy for a provincial GN drug formulary that improved patient access to IS treatments for GN in a cost-effective manner and that could be implemented and evaluated using data from the GN Registry. This article describes such a policy initiative in further detail so that other provinces may use the BC experience to inform the development of provincial GN health administration organizations across Canada.
Domains and Activities of the BC GN Network With Specific Examples, Modified From Barbour et al. 18
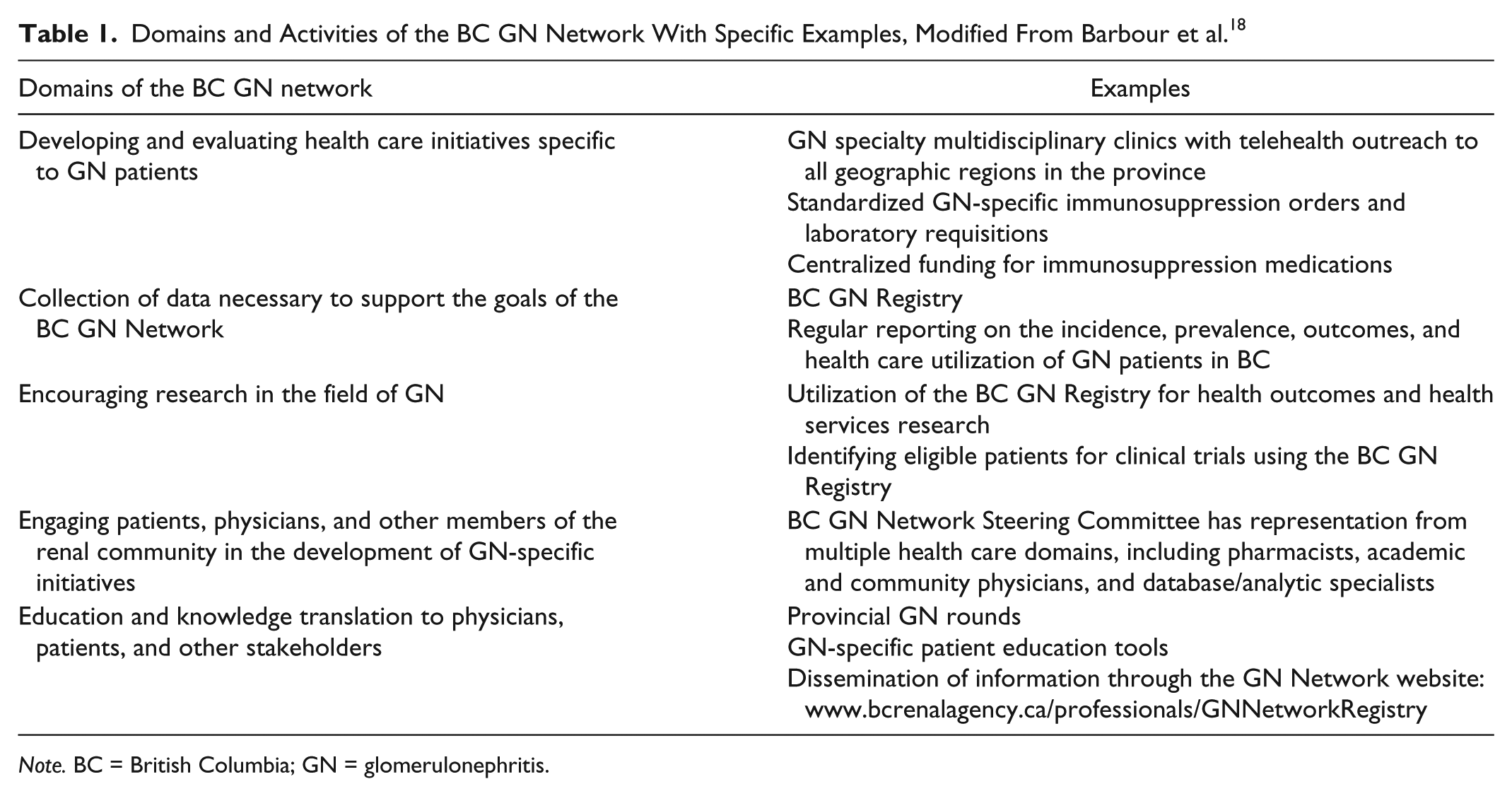
Note. BC = British Columbia; GN = glomerulonephritis.
Historical IS Medication Costs for the Treatment of GN
It is important to accurately describe historical trends in the population-level medication costs for treating glomerular diseases to understand the potential fiscal impact and financial sustainability of a provincial GN drug formulary. Therefore, we linked biopsy data in BC from 2000 to 2012 with a provincial medication administrative database, and described a 7-fold increase in the medication costs per treated patient over a 13-year period from $205 in 2000 to $1394 in 2013 (see Figure 1). 1 The increasing medication costs over time were due to a systematic change in patterns of practice from older cheaper IS medications such as azathioprine, cyclophosphamide, and prednisone, to newer more expensive therapies such as mycophenolate mofetil and calcineurin inhibitors. These practice patterns were not dictated by provincial health policy, but rather by clinical decisions made by individual physicians. In addition, rituximab was used in <4% of patients but contributed 32% toward the increase in per patient medication costs, which emphasizes the disproportionate financial implications of treating a rare minority of patients with extremely expensive medications. Increasing treatment costs over time are not unique to GN, and a similar trend has been observed in kidney transplantation in Canada due to the more frequent use of more expensive induction and maintenance IS medications. 20 With future research focusing on novel but expensive biologic or small molecule therapies, the costs of treating GN are likely to further increase over time and strain the sustainability of provincial health care budgets. This underscores the need for evidence-based provincial GN health policy that will contain medication costs while ensuring patient access to organ- and life-saving therapies.

The mean medication cost per treated GN patient in BC each year for different types of IS medications.
The BC GN Drug Formulary
The BC GN drug formulary is a health policy initiative of the BC GN Network that started in 2014 and was designed to improve patient access to IS therapies while ensuring defensible and transparent control of medication costs. Historically in BC, IS medications were covered by the provincial drug insurance plan (BC PharmaCare) with significant deductibles based on household income. Approval for coverage was determined on a case-by-case basis by nonexpert administrators unfamiliar with glomerular diseases, and drug costs were dictated by individual contracts between distributors and private pharmacies. There was no central accountability or tracking of medication costs or patient outcomes. The BC GN drug formulary centralized funding, approval, and distribution of IS medications for GN under the mandate of the BC Renal Agency, which offers several financial and health services related benefits. First, cost-mitigation strategies can be effectively implemented, including leveraging provincial drug contracts to reduce medication costs, centralized distribution through a limited number of approved pharmacies, and mandating the use of generic instead of brand medications. Second, patients were not required to pay deductibles, similar to other all-cause CKD and ESRD renal-specific medication formularies through the BC Renal Agency. Third, adjudication processes for individual IS medications were created by relevant stakeholders (such as renal pharmacists and nephrologists) with knowledge of glomerular diseases and a vested interest in patient care. Finally, the tracking of medication use, patient outcomes, and the use of treatment protocols offer an opportunity for ongoing quality improvement and comparative outcome assessment.
The financial impact of the BC GN drug formulary health policy has recently been established, resulting in a complete attenuation of the historical increase in IS medication costs. After creation of the GN drug formulary, there was a slow transition of patient coverage from the existing provincial drug insurance plan, which stopped covering GN-related IS medications in 2014. By 2016, transition was likely complete with 627 patients covered under the GN formulary compared with 650 in 2013 under the provincial drug insurance plan. The trend of increasing medication costs over time up to $1394 per treated patient in 2013 was attenuated after creation of the BC GN formulary, with per patient treatment costs of $1405 in 2016 and $1411 in 2017 (see Figure 1). Cost containment was achieved while concurrently improving patient access to the more expensive IS medications. For example, the use of calcineurin inhibitors, mycophenolate mofetil, and rituximab increased substantially after creation of the GN formulary, from 44.6% of treated patients in 2013 to 85.2% in 2016 and 88.3% in 2017. These results demonstrate the BC GN formulary is a successful health policy initiative that contained rising medication costs while improving patient access to evidence-based therapies, and was made possible by to the presence of a coordinated GN-specific provincial health care infrastructure such as the GN Network embedded within the BC Provincial Renal Agency.
Systematic Provincial Conversion of Brand to Generic Tacrolimus
Brand name tacrolimus (Prograf; Astellas, Ontario, Canada) was the most common formulation of tacrolimus historically covered for the treatment of GN in BC. There are multiple forms of approved generic comparators, with estimated costs savings exceeding 40% to 50% depending on the individual health care systems. 21 The equivalence of Prograf and generic tacrolimus in transplantation remains an area of significant controversy, with several,22-25 but not all,26,27 studies suggesting similar pharmacokinetics and short-term graft outcomes. Despite these limitations, generic tacrolimus is increasingly considered a safe, effective, and less costly alternative to Prograf, and has been adopted by many transplant centers across North America. 28 While such an approach would have similar cost benefits in the treatment of GN, the safety and efficacy of Prograf compared with generic tacrolimus in GN patients are not currently known.
The GN Network offered the ideal infrastructure to facilitate a provincial policy of converting brand Prograf tacrolimus to Sandoz generic comparator for the treatment of GN in the context of no prior published data, as it facilitates following all affected patients to ensure efficacy, safety. and tolerability. Prior to June 2015, due to substantial cost differences, the GN formulary covered Prograf tacrolimus only for patients with an intolerance or contraindication to cyclosporine. After that date, all 17 adult patients in BC on Prograf tacrolimus were systematically converted to Sandoz generic tacrolimus in a 1:1 mg ratio. Information was sent to all physicians recommending drug levels at baseline and weekly for 1 month after conversion, with target levels and dosing under the discretion of individual physicians. The GN Registry data infrastructure was used to capture laboratory and medication data, and to flag patients for a baseline and 1-month postconversion telephone assessment by a renal pharmacist to quantify drug side effects using a validated questionnaire. 29 After conversion to generic tacrolimus, there was no difference in the mean tacrolimus level (5.2 vs 5.0 ng/mL, P = .9) or in the mean tacrolimus level normalized to daily dose (100 vs 107 ng/mL/mg/kg/day, P = 1.0), and only 2 patients required dose adjustments (1 mg/d each). There were no disease flares after conversion, no difference in overall adverse event scores (3.35 vs 2.71 out of a maximum score of 35, P = .1), and no difference in tacrolimus-specific side effects including dyspepsia, diarrhea, tremor, headache, or diabetes. This demonstrates the importance of a provincial GN health care and data infrastructure to allow implementation and subsequent evaluation of cost-saving health policy measures while ensuring patient safety and drug tolerability.
Conclusion
The BC GN Network with its centralized drug formulary and data infrastructure is an example of the benefits of expanding the mandate of provincial renal health administrative organizations to include the care of patients with glomerular diseases. The integrated capture of longitudinal population-level data is instrumental to the success of the BC GN Network, facilitating the evaluation of health resource utilization and patient outcomes. A coordinated provincial infrastructure allows for the development of evidence-informed health policies that improve patient care, facilitate access to organ- and life-saving therapies, and mitigate cost increases, while permitting the concurrent systematic evaluation of the impact of specific policy decisions to ensure accountability and safety. Leveraging existing provincial renal health administrative resources for application to a specific high-risk subgroup of patients with glomerular diseases constitutes a viable model that can be implemented in other Canadian provinces to achieve similar goals.
Footnotes
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Consent for publication was obtained from all authors.
Availability of Data and Materials
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.