
Abstract
Introduction:
Chronic knee pain is a common musculoskeletal condition, which usually leads to decreased quality of life and a substantial financial burden. Various non-surgical treatments have been developed to relieve pain, restore function and delay surgical intervention. Research on the benefits of medical cannabis (MC) is emerging supporting its use for chronic pain conditions. The purpose of this study was to evaluate the cost-effectiveness of MC compared to current non-surgical therapies for chronic knee pain conditions.
Methods:
We conducted a cost-utility analysis from a Canadian, single payer perspective and compared various MC therapies (oils, soft gels and dried flowers at different daily doses) to bracing, glucosamine, pharmaceutical-grade chondroitin oral non-steroidal anti-inflammatory drugs (NSAIDs), and opioids. We estimated the quality-adjusted life years (QALYs) gained with each treatment over 1 year and calculated incremental cost-utility ratios (ICURs) using both the mean and median estimates for costs and utilities gained across the range of reported values. The final ICURs were compared to willingness-to-pay (WTP) thresholds of $66 714, $133 428 and $200 141 Canadian dollars (CAD) per QALY gained.
Results:
Regardless of the estimates used (mean or median), both MC oils and soft gels at both the minimal and maximal recommended daily doses were cost-effective compared to all current knee pain therapies at the lowest WTP threshold. Dried flowers were only cost-effective up to a certain dosage (0.75 and 1 g/day based on mean and median estimates, respectively), but all dosages were cost-effective when the WTP was increased to $133 428/QALY gained.
Conclusion:
Our study showed that MC may be a cost-effective strategy in the management of chronic knee pain; however, the evidence on the medical use of cannabis is limited and predominantly low-quality. Additional trials on MC are definitely needed, specifically in patients with chronic knee pain.
Introduction
Chronic knee pain is a common musculoskeletal condition, which usually leads to disability, decreased quality of life and a substantial financial burden. 1 Knee osteoarthritis (OA) is one of the leading causes of chronic knee pain. 2 The Global Burden of Disease 2010 study estimated that the prevalence of radiographically confirmed knee OA was about 4% in the global population, and knee OA was ranked as the 11th highest contributor to disability worldwide. 3
On the basis of different hypotheses surrounding the pathophysiology of knee OA, various treatments have been developed and researched, all of which intend to relieve pain, restore function and delay the necessity for a surgical joint replacement. Current non-surgical options for knee OA pain-relief include treatments such as opioids, non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, viscosupplementation, glucosamine, chondroitin and injection therapies, as well as more conservative means such as exercise, weight control and bracing. Given the number of available interventions for these patients, there is an ongoing emphasis on establishing how they compare to each other in terms of treatment effects, patient satisfaction and tolerability and healthcare costs. 4
Research on the potential analgesic benefits of medical cannabis (MC) is emerging. Cannabis works on the endocannabinoid system – one of the body’s natural analgesic systems and a viable target for reducing pain.5,6 Delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) are 2 major components of MC. They both treat pain, but only THC has psychoactive properties which can cause a sense of euphoria and heightened sensory perception. 7 THC and its analogues have been synthesized for pharmaceutical use for years, whereas the pace of synthesising CBD was slower. Though guidance and suggestions exist, no universally accepted standards have been established on the proper dosing of MC products in chronic pain populations. 8 Currently, on the global market, dronabinol and nabilone are synthetic forms of THC, and Nabiximol and Sativex are a combination of THC and CBD; however, these cannabinoid-based products are manufactured by pharmaceutical companies whereas MC can potentially be a natural form of therapy.
There is also a risk of adverse effects with MC, which primarily occur with products containing higher levels of THC, as it has been shown to be associated with psychoactive effects.8,9 It is important to consider the specific side-effects that are associated with MC, which include fatigue/drowsiness, dizziness, dry mouth, cough/phlegm/bronchitis (when smoked), anxiety, euphoria, nausea and some effects on cognitive ability, as their potential impact on a person’s day-to-day life can vary between patients.8,10
There has been a growing body of evidence supporting the use of MC for chronic pain conditions, such as neuropathic pain,11,12 pain associated with multiple sclerosis 13 and fibromyalgia. 14 In terms of treating arthritis-related pain, published clinical trials are very few; however, a number of trials are ongoing, such as the CBD Treatment in Hand Osteoarthritis and Psoriatic Arthritis (NordCAN, NCT03693833) and the Cannabinoid Profile Investigation of Vapourized Cannabis in Patients With Osteoarthritis of the Knee (CAPRI, NCT02324777) studies. Other than its analgesic effect, MC also shows some effects that may be highly desirable to patients with chronic pain. For example, adding MC to a patient’s treatment protocol could decrease the amount of opioids needed for pain relief and, consequently, reduce the likelihood of opioid-related adverse effects and addiction. 15
Cost-effectiveness analysis (CEA) compares the relative costs and health benefits of different interventions. 16 An intervention is considered cost-effective, relative to another intervention, when the incremental cost-effectiveness ratio (ICER), or cost-utility ratio (ICUR), is less than one’s willingness to pay for the added health benefit. One commonly used measure of health benefit is the quality-adjusted life years (QALYs), which incorporates both the quality and quantity of life in a given health state. 17
Past cost-effectiveness studies on the use of MC products have been conducted in the context of multiple sclerosis, 18 but, as there is limited evidence on MC for chronic knee pain or knee arthritis, there is currently no cost-effectiveness study on these topics. Little is known about whether the health benefits provided by MC could be a cost-effective method for treating chronic knee pain. The purpose of this study was to evaluate the cost and health benefits of MC compared to non-surgical treatments currently used to treat chronic knee pain conditions from a Canadian, single payer perspective.
Methods
Literature search
We conducted a systematic literature search in the MEDLINE database from inception to November 19th, 2019 to collect utility and cost data from published clinical trials or economic evaluations. We developed the structured search strategies using indexed terms and free-text terms related to the patient population (ie, chronic knee pain or knee arthritis) and interventions (ie, cannabis, opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), bracing, glucosamine and chondroitin). We selected these interventions for comparison due to their similarities with MC in terms of their frequencies and methods of administration (ie, daily use/intake and oral ingestion [for pharmacological or dietary supplements]); injection therapies are generally considered a non-surgical, pharmacological intervention as well, but only require a single injection procedure or a small number of injections over just a few weeks, so we deemed such treatments unsuitable for comparison with MC. We included studies published in English, but did not restrict our search by the publication date. We also searched the references lists of included studies and previously performed related reviews for additional eligible articles. In terms of the inclusion of clinical trial data, we prioritized randomized controlled trials (RCTs). We only included trials that provided sufficient baseline and follow-up data so that we could calculate the utilities gained in the study.
After completing the search, we identified no eligible clinical trial data on MC in a chronic knee pain population; therefore, we included outcome data from studies investigating MC for other chronic, non-cancer pain conditions and used this information to quantify utility scores for this treatment. We did not restrict the inclusion of such trials to RCTs due to the limited evidence base on this topic.
For cost data, we prioritized studies conducted in Canada to ensure the values were most representative of costs that would be incurred in Canada. If we did not identify any cost studies conducted in Canada for a given treatment, we referred to studies performed in the United States (US) and included their cost data in our analysis. Then, if we did not locate any cost data for a given treatment in a US study, we referred to economic literature outside of North America.
Data extraction
Three reviewers independently extracted the relevant data. We created the data extraction forms Google sheets and pilot-tested it across the reviewers. We examined all extracted data in duplicate and resolved any discrepancies through discussion. We extracted study characteristics, outcome data expressed as a utility score or that could be converted to a utility score via an established mapping algorithm,19–23 and relevant cost data related to the treatment medication, additional prescription time (if applicable), and required concomitant therapies (if applicable).
Treatment utility scores
We used quality of life (QoL) outcomes to estimate utility scores or converted outcome measure scores to utilities using previously published mapping algorithms. These included the following outcome measures: (1) EuroQoL5D (EQ-5D), (2) Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), (3) 36-item or 12-item Short Form Survey (SF-36 or SF-12), (4) Knee Injury and Osteoarthritis Outcome Score (KOOS), (5) Fibromyalgia Impact Questionnaire (FIQ), (6) 4-item Patient Health Questionnaire, (7) Health Utilities Index Mark 3 (HUI) and (8) Health Assessment Questionnaire (HAQ). We ensured all utility scores were on a 0 to 1 scale, where 1 represented perfect health. 17 When multiple utility scores were available for a given treatment, we considered the entire range of utility scores and calculated a mean and median of this range.
Cost data
We used a Canadian, single payer perspective with respect to costs. For current knee pain therapies (ie, opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), bracing, glucosamine and chondroitin), we acquired cost data for a given treatment from the economic literature, prioritising studies conducted in Canada; otherwise, we referred to studies conducted in the US and, then, outside of North America for treatment costs. For the cost of MC products, we referred to the Spectrum Therapeutics website. 24 We converted all cost data to 2019 Canadian dollars (CAD), using the Bank of Canada Inflation Calculator when needed. 25
When multiple cost estimates were available for a given treatment, we considered the entire range of costs and calculated an arithmetic mean and median of this range. For MC, celecoxib and opioids, only we only considered medication costs. For bracing, we included both the cost of the orthotic device and time spent on brace fitting. For non-selective NSAIDs (diclofenac, naproxen and ibuprofen), we also added the cost of a proton-pump inhibitor for gastrointestinal protection. For the cost of diclofenac, we applied the same cost estimates retrieved for naproxen and ibuprofen, as we did not identify any cost data specific to diclofenac. We considered any other costs related to the treatment of chronic knee pain to be equivalent between therapies.
Cost-utility analysis
We calculated cost-utility ratios as the cost per QALY gained. For each included study, we subtracted the average utility score at the study’s latest follow-up (up to 1 year) by the average baseline utility score. We then calculated incremental cost-utility ratios (ICURs) between treatments under 2 different scenarios:
Mean values from the range of costs and utilities gained
Median values from the range of costs and utilities gained
Based on the available cost data provided on the Spectrum Therapeutics website, we classified MC products as:
Oils
Soft gels
Dried flowers
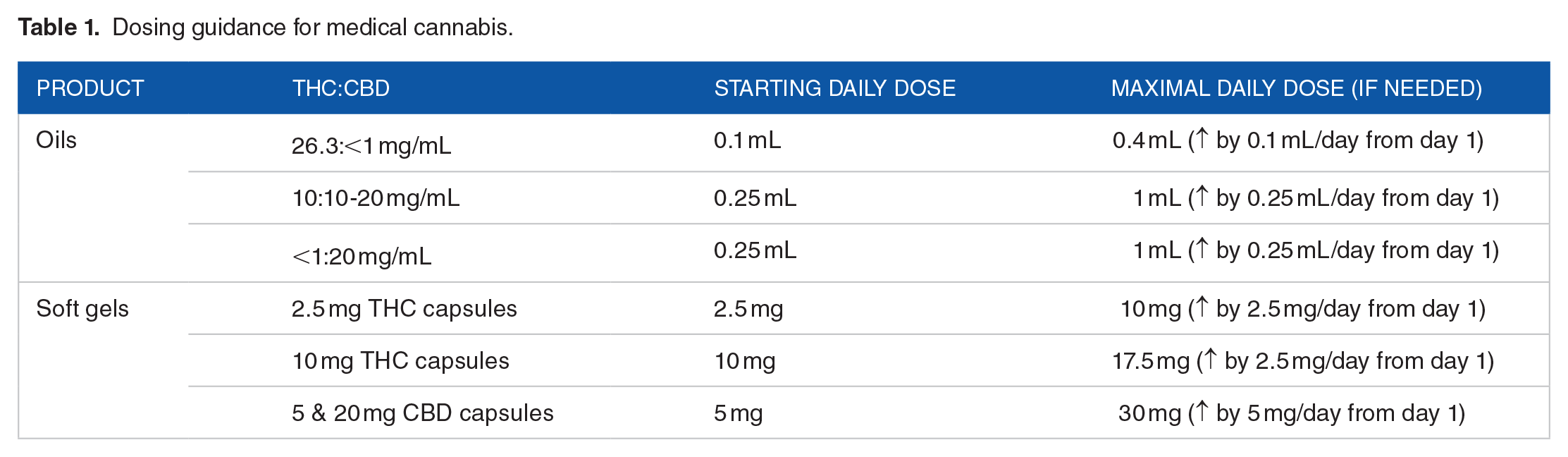
The minimal and maximal recommended doses of MC oils and soft gels were provided by a representative from Spectrum Therapeutics (Table 1), as was the price per gram of dried flowers. Oils and soft gels are priced differently depending on the THC:CBD content, so we calculated the mean and median price across the range of options, according to both minimal and maximal dosing recommendations. As there is no standard dosing recommendation for the inhalation of dried flowers, we examined outcomes across a range of different doses between 0.5 to 1.25 g per day, based on average per month consumption estimates in 2018 published by Statistics Canada. 26 On the Spectrum Therapeutics website, dried flowers can be purchased in either a 2- or 15-g jar, which results in a different price per gram (cheaper with a 15-g jar at $6.53 vs $8 CAD per gram with a 2-g jar); for our analysis, we assumed the purchase of a 15-g jar. Due to the lack of evidence in this area, we could not differentiate treatment effects between the different types of MC (ie, oils, soft gels, dried flowers and the variable THC:CBD ratios); therefore, we assumed similar treatment effects across all MC products. We conducted data extraction and analysis using Microsoft Excel (Version 2010, Microsoft, Redmond, WA, USA) over a 1-year time horizon.
Dosing guidance for medical cannabis.
For comparisons against a willingness-to-pay (WTP) threshold, we used values of $50 000, $100 000 and $150 000 USD,27–29 which, currently, are approximately equal to $66 714, $133 428 and $200 141 CAD, respectively.
Results
Utility scores
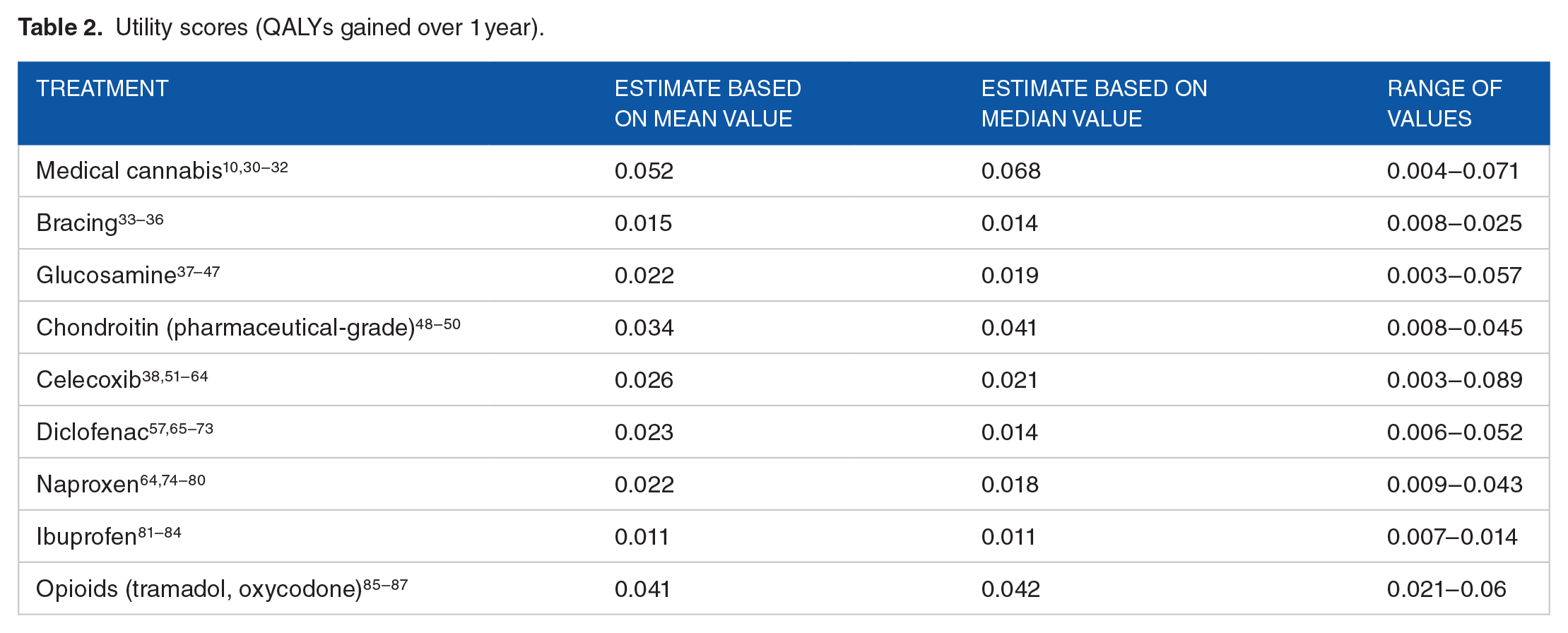
The estimated utilities gained for each treatment are presented in Table 2, showing the mean, median and range of QALYs gained over 1 year across the included trials. Regardless of the estimate chosen, MC appears to provide the greatest QALYs gained among all treatments, while ibuprofen results in the least. Generally speaking, pharmaceutical-grade chondroitin and opioids also provide more favourable gains in QALYs over 1 year.
Utility scores (QALYs gained over 1 year).
Costs
Treatment costs are summarized in Table 3. Based on the average estimate of cost data, MC oils can range from $164 to $657 per year, and soft gels can range from $616 to $1296 per year; the yearly cost of smoking dried flowers can vary dramatically depending on how many grams are smoked per day. For current knee pain therapies, orthotic intervention with bracing and dietary supplementation with glucosamine are the cheapest therapies, pharmaceutical-grade chondroitin is priced in the mid-range, and oral NSAIDs and opioids are, generally, priced highest.
Costs for 1 year of treatment (2019 CAD, rounded to nearest dollar).

Mean estimate = median estimate.
Cost-utility
Based on mean estimates (Table 4) and a WTP threshold of $66 714 CAD, all forms of MC consumption were cost-effective compared to any knee pain therapy, except dried flowers at 1 and 1.25 g/day; dried flowers at 1 g/day compared to pharmaceutical-grade chondroitin and dried flowers at 1.25 g/day versus glucosamine, pharmaceutical-grade chondroitin and opioids were only cost-effective when the WTP was increased to $133 428 CAD/QALY gained.
Incremental cost-utility ratios (ICURs) based on mean utility and mean cost estimates (cost/QALY gained).

Abbreviations: Cele., celecoxib; Chon., chondroitin; Diclo., diclofenac; Dom., dominated (ie, MC product is more effective and cheaper than the comparator treatment); Glucos., glucosamine; Ibu., ibuprofen; Naprox., naproxen.
Positive ICUR indicates that the MC product is more effective but also more costly than the comparator treatment.
Cost-effective at a WTP of $66 714 CAD/QALY gained.
Cost-effective when WTP increased to $133 428 CAD/QALY gained only.
Based on median estimates (Table 5) and a WTP threshold of $66 714 CAD, all forms of MC consumption were cost-effective compared to any knee pain therapy, except dried flowers at 1.25 g/day; dried flowers at 1.25 g/day versus pharmaceutical-grade chondroitin were only cost-effective when the WTP was increased to $133 428 CAD/QALY gained.
Incremental cost-utility ratios (ICURs) based on median utility and median cost estimates (cost/QALY gained).

Abbreviations: Cele., celecoxib; Chon., chondroitin; Diclo., diclofenac; Dom., dominated (ie, MC product is more effective and cheaper than the comparator treatment); Glucos., glucosamine; Ibu., ibuprofen; Naprox., naproxen.
Positive ICUR indicates that the MC product is more effective but also more costly than the comparator treatment.
Cost-effective at a WTP of $66 714 CAD/QALY gained.
Cost-effective when WTP increased to $133 428 CAD/QALY gained only.
Regardless of the estimates used (ie, mean or median estimates), both MC oils (Figure 1) and soft gels (Figure 2) at both the minimal and maximal recommended daily doses were cost-effective compared to all current knee pain therapies at the lowest WTP threshold (ie, $66 714/QALY gained). Medical cannabis dried flowers were only cost-effective compared to all knee pain therapies at the lowest threshold up to a certain dosage (0.75 and 1 g/day based on mean and median estimates, respectively).
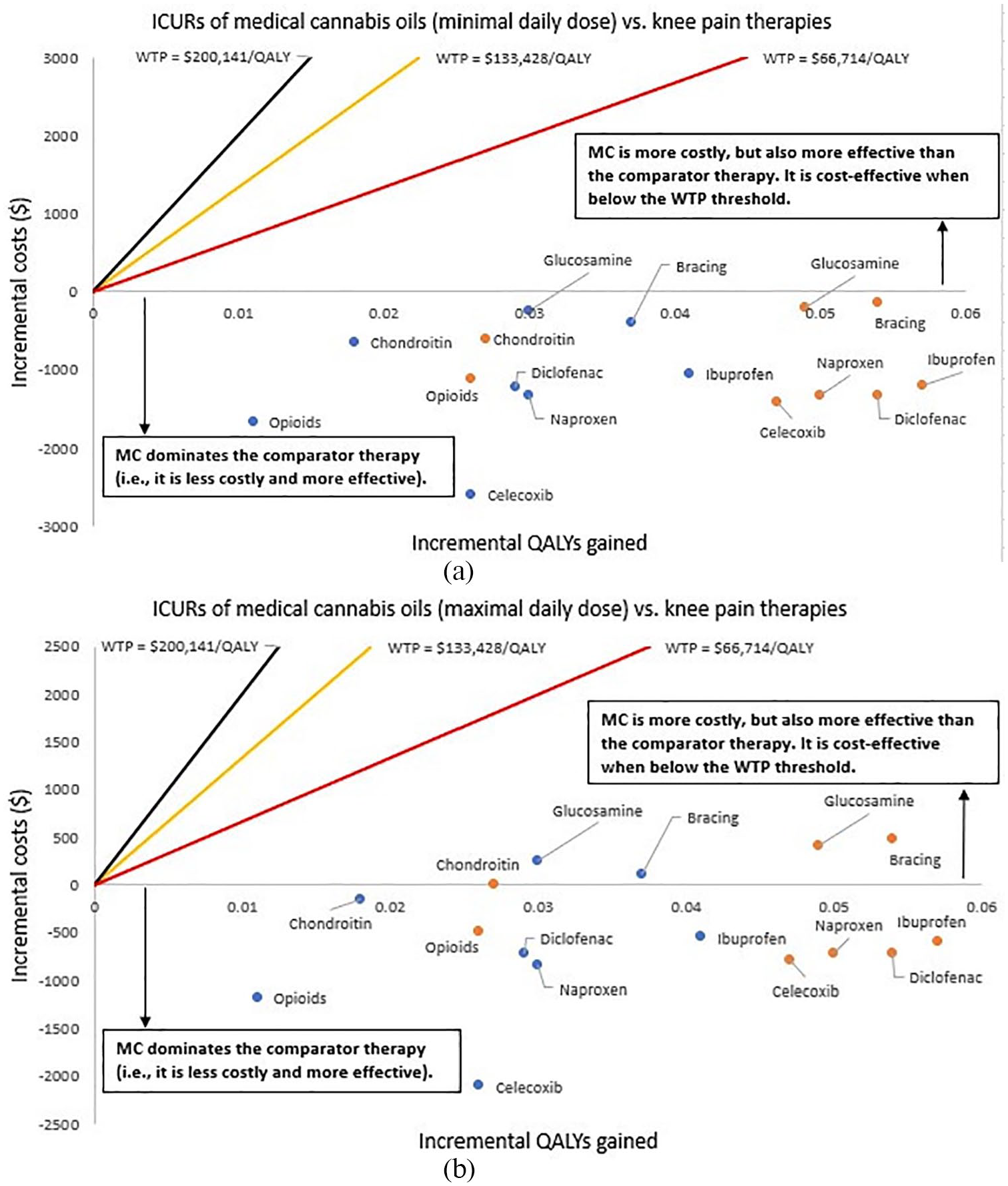
Incremental cost-utility ratios (ICURs) of medical cannabis oils versus knee pain therapies at the (a) minimal and (b) maximal recommended daily doses.

Incremental cost-utility ratios (ICURs) of medical cannabis soft gels versus knee pain therapies at the (a) minimal and (b) maximal recommended daily doses.
Discussion
The purpose of this study was to estimate the cost-effectiveness of MC in patients with chronic knee pain. Prior cost-effective studies have looked at cannabinoid-based therapies in multiple sclerosis with Sativex and chronic neuropathic pain with smoked cannabis.97–101 This analysis showed that, depending on the chosen WTP threshold, MC therapies could be a cost-effective strategy relative to current non-surgical knee pain therapies, namely, bracing, glucosamine, pharmaceutical-grade chondroitin, various oral NSAIDs and opioids. More specifically, MC oils and soft gels at both the minimal and maximal recommended daily doses were all cost-effective at the most conservative (ie, lowest) WTP value of $66 714 CAD (or $50 000 USD) per QALY gained compared to current knee therapies; MC consumption via dried flowers may only be cost-effective up to a certain daily dose, unless the WTP is increased to $133 428 CAD (or $100 000 USD) per QALY gained.
In terms of AEs, the extent to how related and how serious these AEs are must also be considered. The reported estimate for bracing appears high (ie, 67%), but this was just from 1 study and the nature of adverse effects related to the device are likely not severe, largely being associated with superficial skin irritation and patient discomfort while wearing the device. 35 Glucosamine and chondroitin have been shown to be generally well-tolerated102,103; however, certain patients may be allergic, some may experience minor gastrointestinal effects and they are usually administered with a salt, which would increase daily sodium intake.103–105 In addition, there is some uncertainty regarding glucosamine’s effect on glucose metabolism.103,104 Toxicities that have been considered related to chronic oral NSAID use, especially non-selective types, are gastrointestinal bleeding, erosion or ulceration, dyspepsia, chronic diarrhea, cardiovascular risks, renal failure and colonic perforation,106–109 while those related to opioids include constipation, respiratory depression, nausea, urinary retention, hyperalgesia, behavioural side-effects and, more importantly, overdose-related mortality due to addiction and increased tolerance.8,107,110 In order to limit the gastrointestinal effects of non-selective NSAIDs, gastrointestinal protective agents, such as proton pump inhibitors, and COX-2 inhibitors were developed, but those come at increased costs and there is still a risk.107,109 Also, COX-2 inhibitors may lessen gastrointestinal toxicity, but they may still increase the risk of adverse cardiovascular effects.107,110,111
Adverse events related to MC are primarily seen with products containing higher levels of THC as it has been shown to be associated with the psychoactive effects of MC consumption.8,9 The current recommendation for THC consumption is no more than 30 mg/day and, preferably, in conjunction with CBD. 8 In the 2 included trials that reported the risk of AEs following MC therapy, the 1 associated with a higher incidence of AEs (88% over 12 months) prescribed herbal MC with 12.5% THC, 10 whereas the 1 reporting the lower incidence (10% over 3 months) initially provided patients with an oral MC capsule containing a 1:1 ratio of THC to CBD, though a vapor pen containing 2 mg of THC per 0.1 mg of CBD (20:1 ratio) was also prescribed to any patient experiencing breakthrough pain. 30 The most common side-effects that have been seen with MC include fatigue/drowsiness, dizziness, dry mouth, cough/phlegm/bronchitis (when smoked), anxiety, euphoria, nausea and some effects on cognitive ability; it appears to have a similar safety profile as pharmaceutical cannabinoids.8,10 According to the study by Ware et al. (2015) on patients with chronic, non-cancer pain, the chronic administration of herbal cannabis revealed no increase in serious AEs, no harm on cognitive function, pulmonary function tests and biochemical measures. 10 There is currently no evidence to suggest that death due to MC overdose should be a concern and it has been shown that patients maintain the same daily dose for years, unlike opioids;8,9 however, contraindications have been established and include individuals who are pregnant or lactating and those with a history of psychosis or respiratory disease (for cannabis smoking), and caution should be taken with those who have an unstable heart condition and when there is potential for drug interactions.8,112
Strength and limitations
A strength of our study was that we retrieved our estimates for utility scores and cost data, when possible, from a systematic review of the literature and, except with MC, we extracted utility scores from RCT. We considered all eligible studies in order to limit bias in our final estimates. As our study was from a Canadian, single payer perspective, prioritized cost data from studies conducted in Canada, when feasible, so that our final cost estimates were most representative of what payers would have to pay in Canada. We also performed 2 types of analyses (ie, mean and median estimates) in order to assess if our final conclusions could change depending on the estimates included in our analysis.
Our study was limited by the fact that we had to use evidence from MC studies that were on patient populations not exactly representative of our target patient population (ie, chronic knee pain). The patients included in these MC studies predominantly had chronic, noncancer pain, though it is unclear if such patients benefit from MC differently than those who have chronic knee pain. Also, due to the limited evidence in this area, we had to include observational data to acquire utility estimates for MC. Another potential limitation was that, when utility scores were not provided in a study, we mapped scores from other outcome scoring measures in order to estimate utility scores. This included a heterogeneous set of different outcome measures and it is unclear how accurate they are at actually capturing utility. Lastly, again due to the limited evidence, we assumed that the effects of MC were the same regardless of the route of administration (ie, oils, soft gels or dried flowers), THC:CBD ratio or daily dosing, which may not truly be the case.
Conclusion
Our study showed that MC therapies may be a cost-effective strategy in the non-surgical management of chronic knee pain relative to current knee pain therapies; however, the evidence on the medical use of cannabis is limited and predominantly low-quality. Additional trials on MC are definitely needed, specifically in patients with chronic knee pain. Future investigations should also focus on establishing if there are any differences in therapeutic effects between the different methods of MC consumption, THC:CBD ratio and daily dosing. The relatedness and severity of adverse events must also be further evaluated as this should be an important part of the decision-making process due to their potential impact on a patient’s quality of life and healthcare costs.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A research grant was received by Spectrum Therapeutics, a Canopy Growth Corporation.
Declaration of conflicting interests:
The author(s) declared no other potential conflicts of interest with respect to the research, authorship and/or publication of this article.