
Abstract
Background:
Survival and hospitalization are critically important outcomes considered when choosing between intensive hemodialysis (HD), conventional HD, and peritoneal dialysis (PD). However, the comparative effectiveness of these modalities is unclear.
Objective:
We had the following aims: (1) to compare the association of mortality and hospitalization in patients undergoing intensive HD, compared with conventional HD or PD and (2) to appraise the methodological quality of the supporting evidence.
Data Sources:
MEDLINE, Embase, ISI Web of Science, CENTRAL, and nephrology conference abstracts.
Study Eligibility, Participants, and Interventions:
We included cohort studies with comparator arm, and randomized controlled trials (RCTs) with >50% of adult patients (≥18 years) comparing any form of intensive HD (>4 sessions/wk or >5.5 h/session) with any form of chronic dialysis (PD, HD ≤4 sessions/wk or ≤5.5 h/session), that reported at least 1 predefined outcome (mortality or hospitalization).
Methods:
We used the GRADE approach to systematic reviews and quality appraisal. Two reviewers screened citations and full-text articles, and extracted study-level data independently, with discrepancies resolved by consensus. We pooled effect estimates of randomized and observational studies separately using generic inverse variance with random effects models, and used fixed-effects models when only 2 studies were available for pooling. Predefined subgroups for the intensive HD cohorts were classified by nocturnal versus short daily HD and home versus in-center HD.
Results:
Twenty-three studies with a total of 70 506 patients were included. Of the observational studies, compared with PD, intensive HD had a significantly lower mortality risk (hazard ratio [HR]: 0.67; 95% confidence interval [CI]: 0.53-0.84; I2 = 91%). Compared with conventional HD, home nocturnal (HR: 0.46; 95% CI: 0.38-0.55; I2 = 0%), in-center nocturnal (HR: 0.73; 95% CI: 0.60-0.90; I2 = 57%) and home short daily (HR: 0.54; 95% CI: 0.31-0.95; I2 = 82%) intensive regimens had lower mortality. Of the 2 RCTs assessing mortality, in-center short daily HD had lower mortality (HR: 0.54; 95% CI: 0.31-0.93), while home nocturnal HD had higher mortality (HR: 3.88; 95% CI: 1.27-11.79) in long-term observational follow-up. Hospitalization days per patient-year (mean difference: –1.98; 95% CI: –2.37 to −1.59; I2 = 6%) were lower in nocturnal compared with conventional HD. Quality of evidence was similarly low or very low in RCTs (due to imprecision) and observational studies (due to residual confounding and selection bias).
Limitations:
The overall quality of evidence was low or very low for critical outcomes. Outcomes such as quality of life, transplantation, and vascular access outcomes were not included in our review.
Conclusions:
Intensive HD regimens may be associated with reduced mortality and hospitalization compared with conventional HD or PD. As the quality of supporting evidence is low, patients who place a high value on survival must be adequately advised and counseled of risks and benefits when choosing intensive dialysis. Practice guidelines that promote shared decision-making are likely to be helpful.
What was known before
Prior studies have yielded conflicting results on the effect of intensive hemodialysis on survival and hospitalization, related to differences in patient population and methodological issues such as selection bias and small sample size.
What this adds
We systematically reviewed the available evidence on the effect of intensive hemodialysis compared with conventional hemodialysis or peritoneal dialysis on survival and hospitalization, and applied the GRADE approach to appraise the quality of evidence. We found that intensive hemodialysis regimes may be associated with reduced mortality and hospitalization, compared with conventional hemodialysis or peritoneal dialysis, but with low or very low overall quality of evidence.
Introduction
Conventional hemodialysis (HD), comprised of 3 weekly sessions of 3- to 4-hour duration, remains the standard regimen for approximately 90% of all prevalent dialysis patients in the United States. 1 Although survival among HD patients in the United States has improved over time, long-term survival remains comparatively poor,2,3 with adjusted all-cause mortality rates up to 7.9 times that of the general Medicare population.2,3 Approximately 1% of all US HD patients dialyze via an intensive regimen, delivered as either short daily (5-7 weekly sessions over 1.5-3 hours in duration) or nocturnal (3-7 weekly sessions over 6-8 hours in duration) treatments, in-center or at home. Intensive HD provides enhanced solute removal, and a growing body of evidence4-9 has suggested improvements in various physiological surrogate outcomes such as phosphate control, nutritional status, left ventricular mass, and anemia, suggesting that intensive regimens could potentially reduce the morbidity and mortality associated with HD. While conventional HD is the most common therapy, home and intensive HD therapies are becoming increasingly accessible, with more options for dialysis modalities from which patients can choose.
The comparative effects of dialysis regimens on mortality have been a major research priority for decades. While it has been argued that the dialysis comparative effectiveness research agenda should shift away from survival, and toward patient-reported outcomes, 10 a recent international Delphi survey confirmed that both patients and health care professionals consider survival a critical outcome in dialysis treatment–related decision-making and research. 11 Moreover, practice guidelines generally consider survival and morbidity-related events, such as hospitalization critical outcomes in formulating practice recommendations. 12
It is well recognized that studies reporting survival outcomes with intensive HD—both randomized trials and observational designs—have yielded conflicting results due to various factors, including differences in study populations and other methodological issues. 13 For clinicians seeking to engage patients in shared decision-making around modality choice, these seemingly disparate findings are barriers to truly informed discussions of benefits and harms.
We therefore undertook this systematic review and meta-analysis of mortality and hospitalization comparing intensive HD with other dialytic therapies. Our primary objective was to use formal methodological quality appraisal methods to determine which bodies of evidence should be used to inform decision-making through future practice guidelines and patient decision-aids addressing modality selection.
Materials and Methods
See Appendix A for detailed methods. This article was prepared in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. 14 An experienced health information specialist developed the search strategies using terms to identify studies of intensive dialysis (see Appendix B for sample search strategy). We included cohort studies with comparator arm, and randomized controlled trials (RCTs) with >50% of adult patients (≥18 years) comparing any form of intensive HD (>4 sessions/wk or >5.5 h/session) with any form of chronic dialysis (peritoneal dialysis, HD ≤4 sessions/wk or ≤ 5.5 h/session), that reported at least 1 predefined outcome (mortality or hospitalization). We excluded studies of hemodiafiltration, hemofiltration, continuous renal replacement therapy, acute kidney injury, and pre-post studies with no separate patient cohort as a comparator arm. To reduce era effects, we excluded studies published before 2000. Two reviewers independently screened citations, evaluated the eligibility of each full-text article using prepiloted eligibility forms, and resolved discrepancies by consensus.
The 2 outcomes assessed were mortality and hospitalization, all-cause or cause-specific. Hospitalization was defined by either the admission rate or the number of days in hospital (per patient-year). We did not collect individual patient-level data. Two reviewers independently extracted study-level data from included studies using custom-made data extraction forms. For each outcome of interest, we extracted the unadjusted effect estimate, any adjusted effect estimates with factors included in the adjusted model, and methodological factors relevant to the quality appraisal. Disagreements in data collection were resolved by consensus.
Methodological Quality Appraisal
We applied the GRADE quality appraisal criteria summarized in GRADE evidence profile tables, which include risk of bias, 15 indirectness, 16 inconsistency, 17 imprecision, 18 and publication bias. 19 For RCTs, risk of bias was assessed using criteria proposed by the Cochrane Collaboration. 20 For observational studies, we used the modified Newcastle-Ottawa criteria proposed by the CLARITY Group. 21
Data Synthesis
We planned to compute pooled effect estimates of randomized and observational studies separately, and used the I2 statistic to quantify heterogeneity. We used mean differences to pool the continuous outcomes of hospitalization days/patient-year and hospitalization rates/patient-year, and used hazard ratios to pool the dichotomous outcome of mortality. We used a random effects model to account for within- and between-study heterogeneity when there were more than 2 pooled studies, and a fixed model when there were 2 studies. 22 All statistical analyses were conducted using Review Manager (RevMan) Version 5.3 Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Results
Study Characteristics
Our search yielded 8198 citations. After excluding 1379 duplicates, 6819 citations were screened and 348 were reviewed in full-text. Twenty-three articles fulfilled all eligibility criteria and were included in the final review23-45 (Figure 1), with a total of 70 506 reported patients (45 370 on conventional HD, 9582 on PD, and 15 444 on intensive dialysis). Three of the 23 included studies were RCTs,25,28,42 and the remaining 20 were observational cohort studies. Follow-up ranged from 1 to 23 years. Study population mean age ranged from 40.9 to 55.8 years in the intensive HD group, and from 40.9 to 62.4 years in the comparator group (conventional HD or PD) (Table 1). Definitions for intensive dialysis varied by study, with 8 studies of frequent short daily HD (ranging from 5 to 6 days per week) and 15 studies of long nocturnal HD (ranging from 5.0 to 10 hours per day).

Study flow diagram.
Baseline Characteristics of Included Studies.

Note. HD = hemodialysis; PD = peritoneal dialysis; NHD = nocturnal hemodialysis; SDHD = short daily hemodialysis; NR = not reported. Pros. Obs = Prospective Observational Ret. Obs = Retrospective Observationa NHMRC = National Health and Mental Research Council NIH = National Institutes of Health NIDDK = National Institute for Diabetes and Digestive Diseases CMS = Centers for Medicare and Medicaid Services CIHR = Canadian Institutes for Health Research
Hospitalization outcomes also reported.
Most contemporary reported cohort.
In 95% of sample.
In 99% of sample.
In 94% of sample.
Median.
In 61% of sample.
Results of Individual Studies
Effect estimates for mortality and hospitalization in individual studies are described in Tables 2 and 3. Factors included in adjustment analysis varied across studies (Table 4).
Mortality Event Rates From Individual Studies.
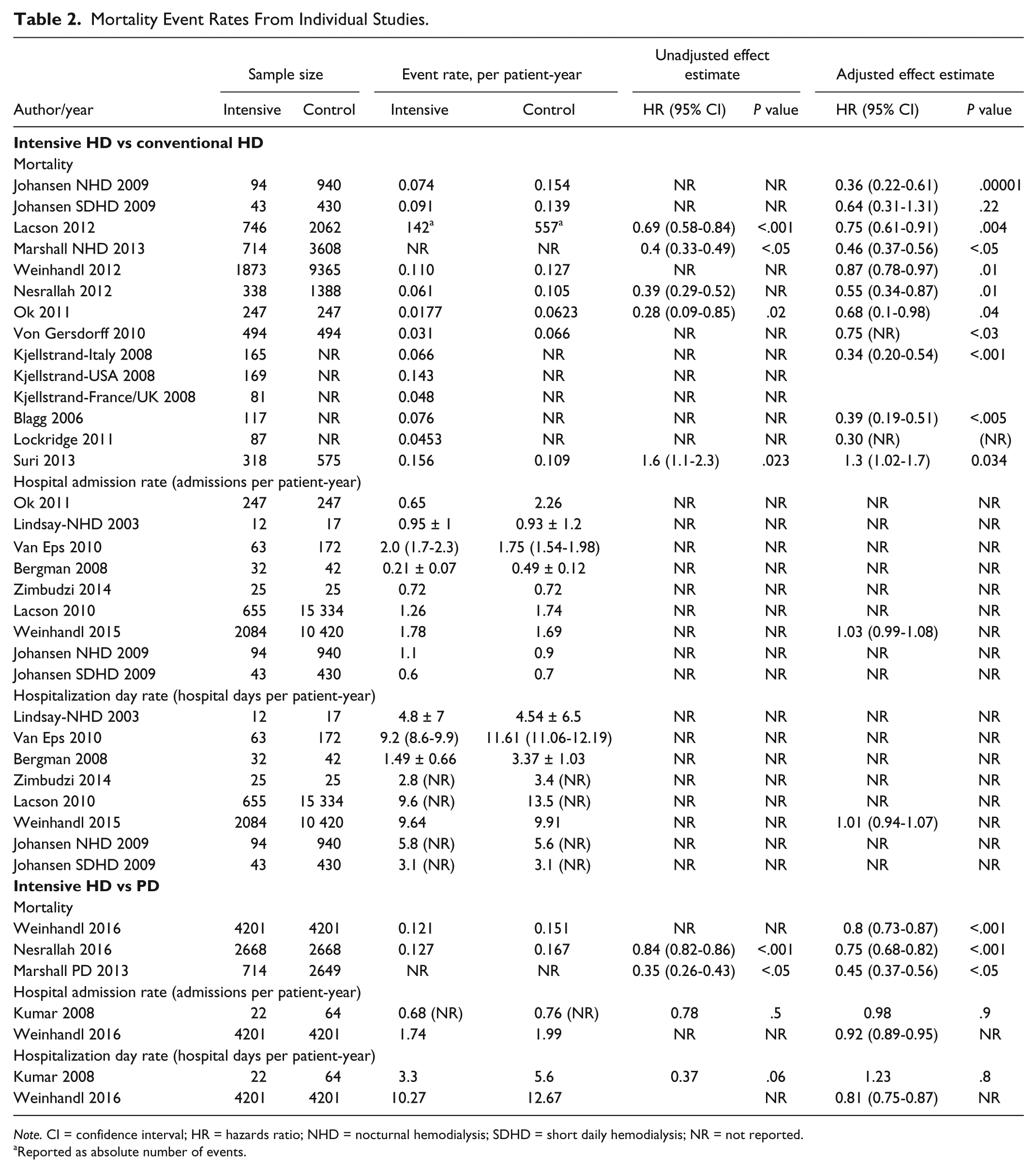
Note. CI = confidence interval; HR = hazards ratio; NHD = nocturnal hemodialysis; SDHD = short daily hemodialysis; NR = not reported.
Reported as absolute number of events.
Mortality Event Rates From Randomized Controlled Trials.
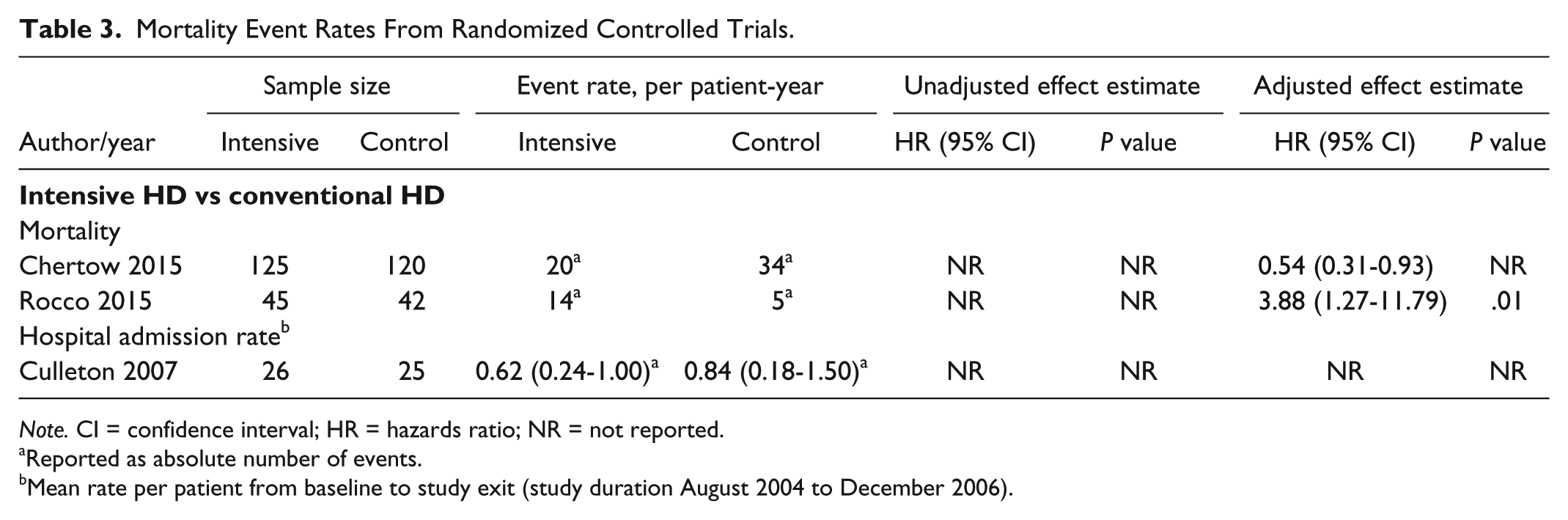
Note. CI = confidence interval; HR = hazards ratio; NR = not reported.
Reported as absolute number of events.
Mean rate per patient from baseline to study exit (study duration August 2004 to December 2006).
Factors Adjusted and Not Adjusted for in Multivariable Analysis and/or Study Design.

Note. BMI = body mass index; ESRD = end-stage renal disease; GFR = glomerular filtration rate; HD = hemodialysis; LVM = left ventricular mass.
Additionally adjusted for Charlson comorbidity index; cardiovascular-related, myocardial infarction; congestive heart failure; peripheral vascular disease; cerebrovascular disease; hyperparathyroidism; and cancer.
Did not adjust for any factors.
Additionally adjusted for Charlson Comorbidity Index, cardiovascular-related, myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, hyperparathyroidism or cancer.
Mortality: Thirteen studies23-35 examined mortality in intensive HD compared with conventional HD (2 RCTs and 11 observational studies). The 2 RCTs25,28 were long-term follow-up studies from the Frequent Hemodialysis Trials group, analyzed using intention-to-treat principles, but with inconsistent continuation of the randomization intervention. In a follow-up study to the Frequent Hemodialysis Network (FHN) short daily trial over a median of 3.6 years, Chertow et al described the relative mortality hazard for daily versus conventional HD as 0.54 (95% confidence interval [CI]: 0.31-0.93). Similarly, in a follow-up to the FHN nocturnal trial over a median of 3.7 years, Rocco et al described the relative mortality hazard for follow-up for nocturnal versus conventional HD as 3.88 (95% CI: 1.27-11.79). Of the remaining 11 observational studies, the adjusted hazard ratio (HR) for intensive HD compared with conventional HD ranged from 0.36 (95% CI: 0.22-0.61) to 0.87 (95% CI: 0.78-0.97).
Three observational studies examined mortality in intensive HD compared with PD.26,43,45 The adjusted HR for intensive HD compared with PD varied from 0.45 (95% CI: 0.37-0.56) to 0.8 (95% CI: 0.73-0.87).
ii. Hospitalization: One RCT 42 reported adverse events of mean hospitalizations per patient from baseline to study exit in both the nocturnal (0.62; 95% CI: 0.24-1.00) and conventional HD groups (0.84; 95% CI: 0.18-1.50) (Tables 2 and 3).
Ten observational studies reported hospitalization rates. Eight compared intensive HD with conventional HD,23,30,36-41and 2 compared intensive HD with PD43,44 (Tables 2 and 3). Only 3 of these studies also reported an unadjusted and/or adjusted relative treatment effect estimate comparing intensive HD with PD or conventional HD.41,43,44
Synthesis of Results
Due to incomplete data reporting, only 13 of the 23 studies in this systematic review were included in the meta-analysis23,26,27,29,30,32,33,36-38,43,45,46 (Figures 2-7 and Tables 5-8).

Comparative risk of mortality in nocturnal home HD versus conventional HD.

Comparative risk of mortality in nocturnal in-center HD versus conventional HD.

Comparative risk of mortality in short daily home HD versus conventional HD.

Comparative risk of mortality in intensive HD versus PD.

Comparative mean difference in hospitalization days/patient-year for nocturnal home HD versus conventional HD.

Comparative mean difference in hospital admission rate/patient-year for nocturnal home HD versus conventional HD.
GRADE Evidence Profile Table: Effects of Nocturnal Home HD Compared With Conventional HD in Patients on Chronic HD.

Note. CI = confidence interval; HR = hazard ratio; MD = mean difference.
Risk of bias due to incomplete adjustment for prognostic factors in statistical analysis.
Absolute event counts not provided, precluding estimation of absolute event rates.
Extremely low control group event rate suggests uneven baseline prognosis between treatment groups.
Low event rates and small overall sample size reduce precision for this outcome; optimal information size criterion not met.
Small sample size; observed effect may be due to random error.
I2 = 77% for pooled effect estimate, possibly due to unexplained heterogeneity in study population and study design.
CI overlaps, no effect.
Lack of blinding may have biased hospitalization practices and adjudication of hospitalization events.
GRADE Evidence Profile Table: Effects of Nocturnal In-Center HD Compared With Conventional HD in Patients on Chronic HD.

Note. HD = hemodialysis; CI = confidence interval; HR = hazard ratio;
Some concern for incomplete adjustment for prognostic factors in statistical analysis.
I2 = 57% for pooled effect estimate, could not exclude heterogeneity due to study design.
Absolute event counts not provided, precluding estimation of absolute event rates.
GRADE Evidence Profile Table: Effects of Short Daily Home HD Compared With Conventional HD in Patients on Chronic HD. a

Note. Only 1 study compared short daily in-center HD with conventional HD, precluding pooling. HD = hemodialysis; CI = confidence interval; HR = hazard ratio.
Concerns that selection of exposed and unexposed from different population, and concern for residual confounding.
I2 = 82% for pooled effect estimate, possibly due to unexplained heterogeneity in study design.
Absolute event counts not provided, precluding estimation of absolute event rates.
GRADE Evidence Profile Table: Effects of Intensive HD Compared With PD in Patients on Chronic HD.
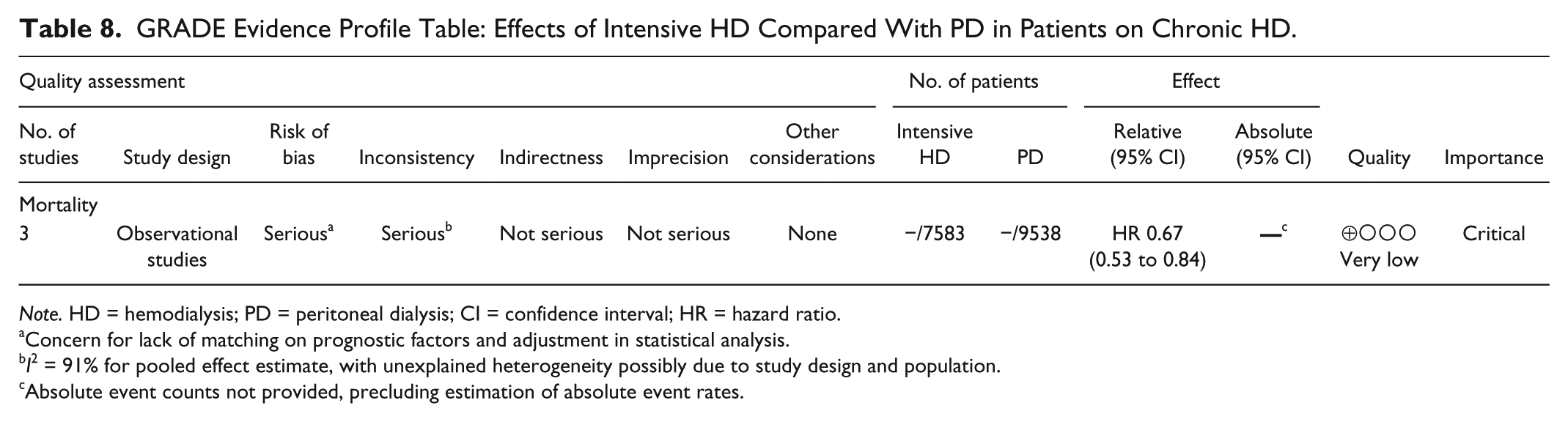
Note. HD = hemodialysis; PD = peritoneal dialysis; CI = confidence interval; HR = hazard ratio.
Concern for lack of matching on prognostic factors and adjustment in statistical analysis.
I2 = 91% for pooled effect estimate, with unexplained heterogeneity possibly due to study design and population.
Absolute event counts not provided, precluding estimation of absolute event rates.
Nocturnal HD versus conventional HD: Three observational studies23,26,29 reported risk of all-cause mortality in nocturnal home HD compared with conventional HD, with a pooled hazard ratio of 0.46 (95% CI: 0.38-0.55; I2 = 0%), favoring nocturnal home HD over conventional HD. Two observational studies30,46 reported risk of all-cause mortality in nocturnal in-center HD compared with conventional HD, and favored nocturnal in-center HD (HR: 0.73; 95% CI: 0.60-0.90; I2 = 57%). Only 1 RCT 28 by Rocco et al reported mortality in this patient group, precluding pooling.
Three studies36 -38 reported mean hospitalization days per patient-year in nocturnal home HD compared with conventional HD, with a pooled mean difference of −1.98 (95% CI: –2.37 to −1.59; I2 = 6%) favoring nocturnal HD. The mean hospital admission rate per patient-year favored nocturnal home HD, with a pooled mean difference of −0.04 (95% CI: –0.46 to 0.38; I2 = 77%).
ii. Short Daily HD versus conventional HD: Four studies23,27,32,33 reported risk of all-cause mortality in short daily home HD compared with conventional HD, and favored short daily home HD (HR: 0.54; 95% CI: 0.31-0.95; I2 = 82%).
One observational study 35 by Suri et al and one RCT 25 by Chertow et al compared short daily, in-center HD with conventional HD, precluding pooling of estimates for this predefined group.
iii. Intensive HD versus PD: Three studies26,43,45reported risk of all-cause mortality in intensive HD compared with PD (2 examined nocturnal home HD, and 1 examined short daily, home HD). Pooled HR was 0.67 (95% CI: 0.53-0.84; I2 = 57%) favoring intensive HD over PD.
The remainder of studies in predefined patient groups did not report adequate data such as measures of dispersion, precluding pooling.
Methodological Quality
Tables 5 to 8 summarize the quality appraisal by predefined patient groups on an outcome-by-outcome basis. RCTs assessed outcomes of mortality and hospitalization rate in nocturnal home HD. Quality of evidence for the RCTs assessing mortality was low (imprecision). Quality of evidence for the RCT assessing hospitalization rate was also low (imprecision and risk of bias due to lack of blinding). For observational studies, risk of bias was serious in all pooled estimates. Concern for risk of bias was due to incomplete adjustment for all important prognostic factors and selection of exposed and unexposed cohorts from different populations (Appendix C). Inconsistency (due to heterogeneity from study design, study population characteristics, treatment indication, or unexplained heterogeneity) and imprecision (due to small sample size or CIs overlapping no effect) also affected the quality of most estimates. Small numbers of included studies in any predefined patient group precluded meaningful analysis of publication bias by funnel plots. The overall quality of evidence was low or very low for critical outcomes.
Discussion
To our knowledge, this is the first systematic review and meta-analysis of mortality and hospitalization in intensive HD compared with conventional HD and PD. Compared with conventional HD, nocturnal home HD, nocturnal in-center HD, and short daily home HD were all significantly associated with decreased mortality. Intensive HD was also significantly associated with decreased mortality when compared with PD. With respect to hospitalization outcomes, nocturnal home HD was significantly associated with decreased rate of hospitalization days per year, but had no appreciable association with the rate of hospital admissions per year. The overall quality of evidence for these outcomes was similarly low across observational studies (primarily due to residual confounding and selection bias) and RCTs (primarily related to imprecision due to small study populations and low event rates) for a given modality comparison.
Among the studies reporting outcomes with nocturnal home HD, one RCT by Rocco et al 28 reported higher mortality in patients on nocturnal home HD versus conventional HD. In contrast, our pooled analysis of observational studies found reduced mortality with home nocturnal HD. Reasons for this discrepancy may include the following: (1) The RCT was not powered to detect differences in mortality alone, and observed differences in patient survival could be explained by chance alone; (2) RCT conventional HD participants had a very low death rate of 0.032 events per patient-year, 5-fold lower compared with HD patients in the US Renal Data System, 47 thus increasing the risk of type I error; (3) frequent modality changes over long-term follow-up precluded attributing causality to the baseline dialysis regimen—the as-treated analysis of the FHN nocturnal cohorts using the prior 6-month average exposure in fact found no significant difference in long-term survival 28 ; (4) in the observational studies, patients who selected home nocturnal HD represent a healthy population with lower mortality risk, with residual confounding remaining despite statistical adjustment; and (5) loss of residual renal function in the predominantly incident nocturnal HD patients of the RCT (median dialysis vintage 0.9 years) may have contributed to the observed increased mortality.48,49 The observational studies in our pooled analysis did not report residual kidney function, but included prevalent patients who had likely lost most residual function at the time of cohort entry. Patients on nocturnal dialysis in the reports by Johansen et al 23 and Nesrallah et al 29 had a mean time on dialysis of 5 to 6 years at enrolment. Marshall et al 26 included only incident conventional HD patients, while intensive HD patients were all prevalent patients. Loss of residual kidney function in the conventional HD group may have contributed to their observed increased mortality.
Among the studies reporting on short daily HD patients treated in-center, we identified one observational study and one RCT. Using international registry data and a matched cohort design, Suri et al 35 reported higher mortality with in-center short daily HD compared with conventional HD (very low quality of evidence due to risk of bias from incomplete risk adjustment). Conversely, in the long-term follow-up study of FHN daily trial participants, Chertow et al 25 reported lower mortality for in-center short daily HD patients (moderate quality of evidence—rated down one level for imprecision). However, patients in the study by Suri et al were older, had more comorbidities, had a high overall mortality rate, and were typically prescribed daily HD as a “salvage” therapy. 35 Their higher death rate compared with matched controls may have been due to incomplete risk adjustment for disease severity, frailty, and other factors. Conversely, patients in the FHN daily study were healthier and younger and clinical trial participants with an unusually low death rate of only 4% in the first year. 25 These studies therefore inform clearly different clinical effectiveness questions.
Our pooled results also indicated that intensive HD was associated with a lower mortality than PD (very low quality evidence due to risk of bias and inconsistency). All 3 studies included in the meta-analysis compared a home intensive HD regimen with PD, and used advanced modeling and matching techniques to account for measured between-group case-mix differences. Unmeasured potent prognostic factors such as self-efficacy or functional ability may have resulted in some residual confounding favoring home intensive HD.50,51 The available data did now enable a subgroup analysis evaluating the effects of a PD-first approach among patients who later switch to intensive home HD.
We identified only 1 RCT 42 examining hospitalization in intensive HD, which precluded pooling. Our meta-analysis of studies examining hospitalization outcomes found that intensive HD was associated with a lower number of hospitalization days per patient-year. This is in line with findings by Ting et al 8 (excluded for no comparator group), where 42 patients who were converted from conventional HD to short daily HD had a 34.4% reduction in hospitalization days. For intensive HD patients who dialyze at home, greater self-efficacy may have facilitated earlier discharge from hospital.
It is important to note that the intervention of intensive HD itself may confer complications beyond those included in our review. Increased access frequency has been associated with complications including need for thrombectomy and surgical revision. 52 Alternate needling methods, such as buttonhole cannulation, may be associated with increased risk of infection. 53 Long hours of nocturnal HD may lead to electrolyte imbalances (hypokalemia, hypophosphatemia), and fluid removal associated hypotension with organ ischemia. 54 More frequent or long hours of exposure of blood to the dialyzer membrane may be associated with increased inflammation 55 and decreased survival.56,57
Strengths of our study include the use of rigorous systematic review and quality appraisal methods, resulting in evidence summaries that are usable by a range of audiences. Our study’s limitations are primarily those of the included studies as described in our quality appraisal. Additional potential limitations include the following: (1) Our a priori definitions of eligible intensive dialysis prescriptions may have resulted in exclusion of some studies; (2) we identified some variability in dialysis technology, including the use of low-flow dialysate systems, which may have introduced clinical heterogeneity in our meta-analyses; and (3) our findings should not be extrapolated to patients outside of the inclusion criteria of the RCTs and observational studies in this review, which generally include nonpregnant, maintenance HD patients without mental incapacity, medical contraindications to intensive dialysis, or short lifespan (eg, less than 6 months). In addition, the FHN Short Daily study 25 excluded patients with residual kidney function of greater than 3 mL/min per 35 L. Finally, we did not study quality of life, transplantation, and vascular access outcomes, and cannot issue general guidance regarding modality choice and these critical outcomes.
Based on our findings, we recommend several future avenues of research and work. First, clinical practice guidelines and decision-aids addressing dialysis modality selection with an emphasis on shared-decision making are needed. While strong recommendations based on high-quality evidence are desirable, guidelines can be most useful when there is less certainty surrounding treatment effects. When confidence in treatment effect measures is low, guideline statements will typically be qualified or “conditional,” and provide direction not on a specific treatment option, but rather on how clinicians should engage patients in shared decision-making, including which values and preferences to elicit when considering a pair of treatment alternatives. 58 Second, our review findings challenge the notion that all dialysis modalities provide similar outcomes. Currently, the only modality selection guideline published to date endorses a “modality-neutral” approach, in which patients are advised to focus on preferences rather than outcomes. 59 However, our findings suggest that some fully informed and highly motivated patients may consider more intensive regimens. Patients who place a very high value on survival may choose an intensive HD regimen despite the increased effort and despite the uncertainty in the published evidence. Thus, comparative effectiveness research of dialysis modalities is needed to aid in reducing uncertainty around candidate treatment alternatives, and obtaining truly informed consent. Third, international standards for patient decision-aids have been established and the inclusion of up-to-date quality-appraised evidence summaries of dialysis modality selection in these knowledge products is considered essential to truly informed patient choice. 60 Finally, studies evaluating the effects of intensive dialysis for patients with specific clinical indications (frailty, severe heart disease, restoring fertility, improving obstetrical outcomes) would be of significant value.
Conclusion
Home and intensive HD therapies continue to proliferate globally, calling on more clinicians to engage patients in discussing increasingly complex treatment decisions. We found the quality of supporting evidence is low, and thus, patients who place a high value on survival must be adequately advised and counseled of risks and benefits when choosing intensive dialysis. Survival is but one among several critical outcomes that patients must weigh against their other needs, values, and preferences. Moving toward more transparent and evidence-informed decision making seems not only timely but essential.
Footnotes
Appendix A
Appendix B
Appendix C
Risk of Bias Assessment for Studies Included in Meta-Analysis.

| Author | Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 |
|---|---|---|---|---|---|---|---|---|---|
| Johansen | 2009 | Definitely yes | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Definitely yes |
| Lacson | 2010 | Probably yes | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Definitely yes |
| Lacson | 2012 | Definitely yes | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Nesrallah | 2012 | Probably no | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Definitely yes |
| OK | 2010 | Definitely yes | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Suri | 2012 | Probably yes | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Von Gersdorff | 2010 | Definitely yes | Definitely yes | Definitely yes | Mostly no | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Kjellstrand | 2008 | Probably no | Definitely yes | Definitely yes | Mostly yes | Mostly yes | Definitely yes | Definitely yes | Probably yes |
| Blagg | 2006 | Probably no | Definitely yes | Definitely yes | Mostly no | Probably no | Probably yes | Probably yes | Definitely no |
| Lindsay | 2003 | Definitely no | Definitely yes | Definitely yes | Mostly no | Mostly no | Definitely yes | Probably yes | Probably yes |
| Lockridge | 2011 | Definitely no | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Van Epps | 2010 | Probably no | Probably yes | Definitely yes | Mostly yes | Mostly yes | Definitely yes | Probably yes | Probably yes |
| Bergman | 2008 | Probably no | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Weinhandl | 2014 | Definitely yes | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Weinhandl | 2012 | Definitely yes | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Marshall | 2013 | Probably no | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Nesrallah | 2016 | Probably yes | Definitely yes | Probably yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Weinhandl | 2016 | Probably yes | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Kumar | 2008 | Definitely yes | Definitely yes | Definitely yes | Mostly yes | Probably yes | Definitely yes | Definitely yes | Probably yes |
| Zimbudzi | 2014 | Definitely yes | Definitely yes | Definitely yes | Mostly no | Definitely no | Definitely yes | Probably yes | Probably no |
Ethics Approval and Consent to Participate
Waived by the Northwell Health Feinstein Institute for Medical Research Instutional Review Board (IRB).
Consent for Publication
We have the authors consent for publication.
Availability of Data and Materials
All data available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.