
Abstract
Background:
Neutrophil-to-lymphocyte ratio (NLR) was widely studied as a prognostic marker in various medical and surgical specialties, but its significance in nephrology is not yet established.
Objective:
We evaluated its accuracy as an inflammation biomarker in a dialysis population.
Design setting:
Single-center retrospective study.
Patients:
The records of all 550 patients who were treated with hemodialysis (HD) or peritoneal dialysis (PD) from September 2008 to March 2011 were included.
Measurements:
NLR was calculated from the monthly complete blood count.
Methods:
Association between NLR and markers of inflammation (C-reactive protein [CRP], serum albumin, and erythropoietin resistance index [ERI]) was measured using Spearman coefficient.
Results:
In total, 120 patients were eligible for the correlation analyses. We found a positive correlation between NLR and CRP (all patients: r = 0.45, P < .001; HD: r = 0.47, P < .001; PD: r = 0.48, P = .13). NLR and albumin were inversely correlated (r = −0.51, P < .001). Finally, high NLR was associated with a nonsignificant increased ERI, but we have not demonstrated a direct correlation.
Limitations:
CRP and albumin are not measured routinely and were ordered for a specific clinical reason leading to an indication bias. Also, no relationship with clinical outcome was established.
Conclusions:
NLR seems to be a good inflammatory biomarker in dialysis in addition to being easily available. However, controlled studies should be conducted to properly assess and validate NLR levels that would be clinically significant and relevant, as well as its prognostic significance and utility in a clinical setting.
What was known before
Neutrophil-to-lymphocyte ratio (NLR) is a prognostic marker of morbidity and mortality for numerous conditions, and was recently associated with all-cause mortality in hemodialysis patients, but no study has ever evaluated the relationship between NLR and erythropoietin (EPO) resistance index (ERI), a measure of EPO resistance associated with inflammation. The aim of this study was to evaluate associations between NLR and inflammation biomarkers (C-reactive protein [CRP], serum albumin, and ERI) in a cohort of chronic dialysis patients.
What this adds
This study demonstrates that NLR correlates positively with CRP and inversely correlates with albumin in patients receiving chronic dialysis, 2 well-known biomarkers of inflammation. While we did not find a correlation between NLR and ERI, high NLR was associated with a nonsignificant increased ERI. This study suggests that NLR is a good biomarker of inflammation. As it can be calculated routinely without additional cost, from the complete blood count, NLR has the potential to be a convenient and inexpensive marker of inflammation in patients receiving chronic dialysis.
Introduction
Neutrophil-to-lymphocyte ratio (NLR) has been studied in medical and surgical populations. It is a prognostic marker of morbidity and mortality for numerous conditions, including cardiovascular disease,1,2 oncology,3,4 critical care medicine, 5 liver disease,6,7 general surgery, 8 and vascular surgery. 9 It was recently associated with all-cause mortality in hemodialysis (HD) patients. 10 Reddan et al were the first to mention its possible use as a biomarker in HD.11 -14 The relationship between NLR and increased inflammatory biomarkers in HD was observed in a cross-sectional study, 13 and another study showed an association between NLR and decreased serum albumin, a surrogate biomarker of inflammation. 14 Moreover, Kalantar-Zadeh et al demonstrated that a low lymphocyte count was associated with refractory anemia in end-stage renal disease (ESRD), another probable surrogate marker of inflammation, but no study has ever evaluated the relationship between NLR and erythropoietin resistance index (ERI), a measure of EPO resistance. 12 Findings from these small studies may be the result of specific populations and may not apply to all dialysis patients. The aim of this study was to evaluate associations between NLR and inflammation biomarkers (CRP, serum albumin, and ERI) in a cohort of chronic dialysis patients. Given that a high CRP and a low serum albumin are inflammatory biomarkers, our hypotheses were that NLR would be directly correlated with CRP and inversely related to serum albumin.
Methods
Study Setting, Population, and Design
We conducted a single-center retrospective study using chart reviews. We included patients older than 18 years who were treated with either HD or peritoneal dialysis (PD) for at least 3 months at our hospital-based outpatient dialysis center in Montreal (Canada) from September 2008 to March 2011. Patients receiving chemotherapy or immunosuppressant were excluded because of its myelosuppressive effect on white cells count. To calculate ERI, we excluded patients who were not treated with an erythropoiesis-stimulating agent (ESA), or had no weight available. Finally, only patients who had at least 1 set of NLR, CRP, and albumin values collected at the same time point were included in the correlation analysis between those markers; therefore, these results do not represent longitudinal changes.
Measurements
We calculated NLR for each patient using absolute neutrophils count (×109/L) divided by absolute lymphocytes count (×109/L) from the complete blood count. For each patient, CRP, serum albumin, and corresponding NLR were collected at each time point during follow-up when they were measured together; multiple observations within the patient were permitted. As a proxy for erythropoietin (EPO) resistance, ERI was calculated by dividing the weekly dose of ESA (U/kg/wk) by the hemoglobin value (g/dL). 15 ERI was calculated at each time point when the dose was modified. Two ESAs were available at our center: epoetin alfa and darbepoetin alfa. Darbepoetin doses were converted to equivalent epoetin dose using a conversion factor of 200:1 as suggested in the product monograph. The corresponding NLR was collected concurrently.
Statistical Analysis
Continuous variables were summarized by median and interquartile range, and categorical variables were summarized by frequency and percent. NLR and CRP, albumin, or ERI values were also presented in quartiles. Associations between NLR and CRP, albumin, or ERI were estimated by Spearman correlation (r) and multivariate linear mixed-effects models. In the correlation analysis, only the first measures of NLR, CRP, albumin, and ERI were included in the analysis. As mixed-effects models account for multiple measures for a single patient, all observed data could be included in the multivariate mixed model. Age, sex, and dialysis modality were also included in the model. We did not use imputation because using multiple imputations might not improve the analysis in this situation, given that data are acknowledged not to be missing at random. Differences between quartiles were analyzed using the Kruskal-Wallis statistic. Statistical significance level was set at .05. Statistical analysis was performed with SAS (SAS 9.2; SAS Institute Inc, Cary, North Carolina).
This project was approved by the Maisonneuve-Rosemont Hospital ethics committee, and informed consent was waived.
Results
Study Participants and Baseline Characteristics
We reviewed the charts of all 550 patients who were treated with dialysis for at least 3 months at our outpatient dialysis center during the observation period. Of these, 42 were excluded as illustrated in Figure 1, leaving 508 patients eligible for the study. Among those, 120 patients had NLR, CRP, and albumin measured at the same time and were included. For analysis, median age was 68 years (interquartile range: 59-76), 42.5% were men, and 90.8% were receiving HD (n = 109).

Flow diagram of the cohort.
NLR and Inflammation
The correlation analysis (Table 1) showed a positive correlation between CRP and NLR (r = 0.45, P < .001). Serum albumin and NLR were inversely correlated (r = −0.51, P < .001). CRP and albumin were also negatively correlated, but to a lesser extent than with NLR (r = −0.34, P < .001). The linear multivariate mixed-effects models were consistent with correlation results (Table 1). An increase in 1 unit of NLR was associated with a 4.64 mg/L increase in CRP and a 0.047 g/dL decrease in albumin (multiply by 10 to convert to g/L of albumin). These relationships are also demonstrated in Figures 2 and 3 where we can note that as NLR increases, CRP increases and albumin decreases (P < .0001).
Correlation and Multivariate Mixed-Effects Linear Regression Analysis for NLR, CRP, albumin, and ERI.

Note. NLR = neutrophil-to-lymphocyte ratio; CRP = C-reactive protein; ERI = erythropoietin resistance index.
Only the first collected specimen for a given patient is included.
All observed data are included (multiple measures per patients).

CRP values according to NLR quartiles (P < .0001).
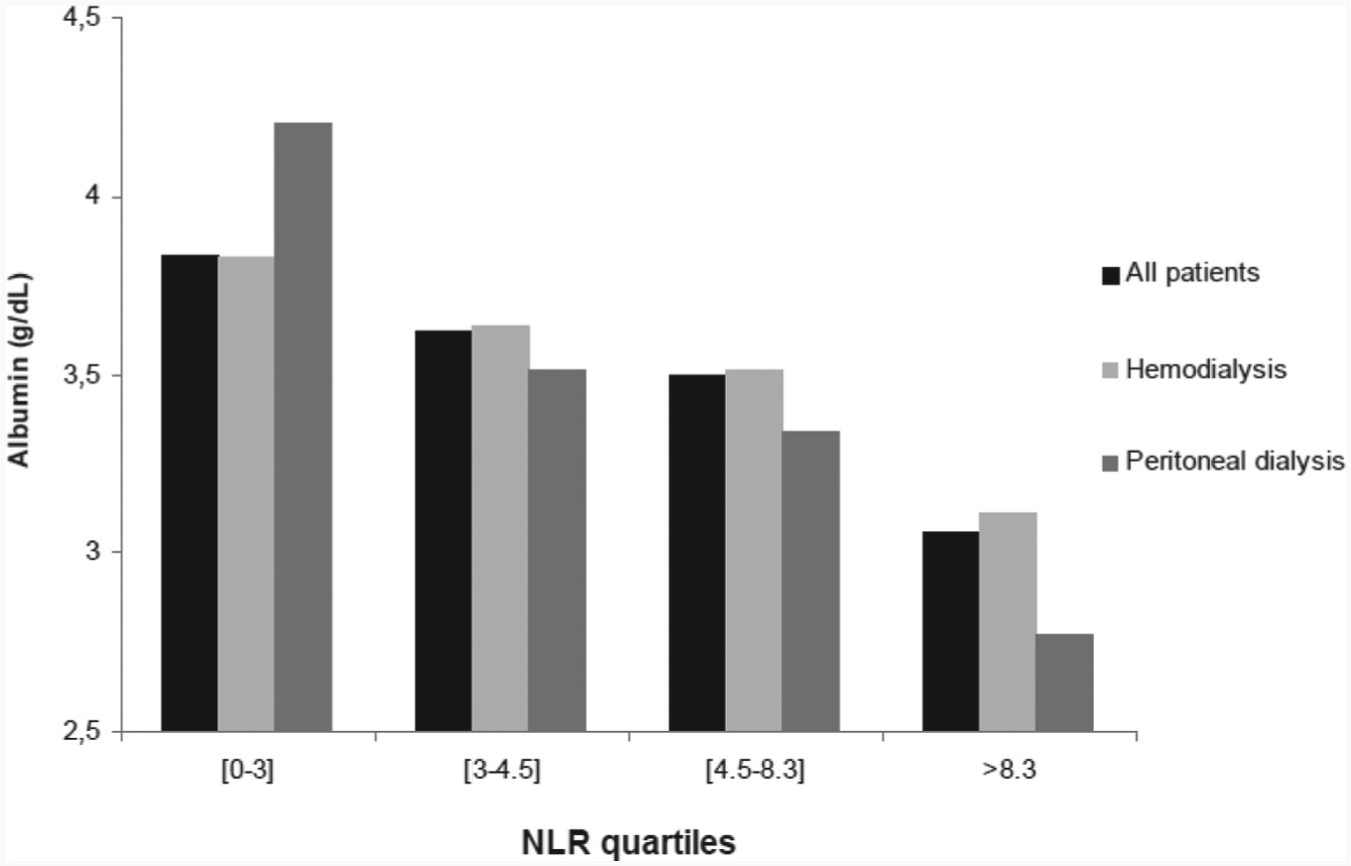
Albumin values according to NLR quartiles (P < .0001).
NLR and EPO Resistance
Correlation between NLR and ERI was negligible, as shown in Table 1 (r = 0.10, P = .27). Relation between ERI and NLR is shown in Figure 4. Mean ERI in all patients seems constant in the first 3 quartiles of NLR (between 24 and 25.5 of ERI). In contrast, at higher level of NLR (Q4 > 8.3), there is an increase in ERI value (29.8), but this was not statistically significant (P = .32).

ERI according to NLR quartiles (P = .32).
Discussion
This study demonstrates that NLR correlates with other biomarkers of inflammation in patients receiving chronic dialysis. Indeed, NLR was modestly positively correlated with CRP and inversely correlated with albumin, 2 well-known biomarkers of inflammation. Although we did not find a correlation between NLR and ERI, the highest quartile of NLR was associated with a nonsignificant higher ERI.
Our results are consistent with a previous study that established an association between NLR and various inflammatory biomarkers in HD. 14 The fact that NLR is simply calculated from easily available complete blood count makes it an interesting biomarker in assessing and detecting inflammatory conditions in dialysis patients. Other specific markers of inflammation (eg, interleukin 6 [IL-6], tumor necrosis factor α [TNF-α], etc) are more expensive and are not routinely used.
In addition, EPO hyporesponsiveness is an important problem in dialysis. Approximately 5% to 10% of chronic kidney disease patients have resistance to EPO to a different extent. 15 Risk factors associated with EPO resistance are not all well-defined, but relationship with inflammation is well established. 15 Using an inexpensive and easily available biomarker to identify patients who are prone to severe EPO resistance could be of interest in early treatment of ESRD-related anemia. NLR seems to be a good biomarker for this purpose. Our observed possible association between the highest NLR quartile and severe EPO hyporesponsiveness suggests that NLR is a biomarker of inflammation in dialysis patients. However, this was not statistically significant; the relation does not seem to be linear, and our results do not support a correlation between ERI and NLR. The fact that EPO resistance is a complex entity and is not only due to inflammation probably explains why we did not find a clear correlation. There are many confounding variables in EPO resistance not exclusively related to inflammation (diabetes, ARB/ACEi [angiotensin receptor blocker/angiotensin-converting enzyme inhibitor] use, dialysis adequacy, severe hyperparathyroidism.) that were not easily measurable in our retrospective study which explain the lack of correlation with NLR.
It is important to note that NLR is one biomarker among others and should not replace clinical judgment. In addition, its sensitivity and specificity for predicting inflammatory conditions remain unknown.
The strengths of our study were as follows. We had a greater statistical power compared with previous studies that observed similar results and, to our knowledge, this is the first study to describe the association between higher NLR and EPO resistance.
However, we recognize that our retrospective study has some limitations. CRP values are not routinely measured in our center and were therefore not available for all patients. Because a clinical condition probably explained why a CRP was sampled in a given patient, the relationship between the NLR and CRP may be different for patients for whom CRP was not measured. These data derive from patients in whom the 3 assessments were made on the same occasion. The decision to order these tests was based on clinical indications. Therefore, the sample is likely to overrepresent patients who are unwell or being investigated for clinical issues. Moreover, other well-known and interesting inflammatory biomarkers previously studied such as IL-6 and TNF-α were not available for the present study. Also, this study was not meant to establish a correlation with clinical outcomes, thus limiting its impact. Finally, the limited number of PD patients limits the generalizability of the results to these patients.
In summary, this study suggests that NLR is a good biomarker of inflammation as well as a potential predictor of EPO resistance, a condition also related to inflammation. As it can be calculated routinely without additional cost from the complete blood count, NLR have the potential to improve the detection of ongoing subclinical illnesses and thus investigate high-risk patients. However, further studies are needed to determine clinically significant thresholds for NLR and its clinical relevance and to validate its incorporation as a biomarker in the design of prognostic models.
Footnotes
Acknowledgements
The authors sincerely thank Mrs Mylène Antiglio, Valérie Bossé, and Naoual Elftouh from Hôpital Maisonneuve-Rosemont for their help in acquiring data and statistical analysis.
Ethics Approval and Consent to Participate
The Hôpital Maisonneuve-Rosemont Research Ethics Board has approved this research study.
Consent for Publication
All authors read and approved the final version of this manuscript.
Availability of Data and Materials
The original data from the chart review will not be made available, as we did not acquire ethics approval to do so.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.