
Abstract
Abstract
Objective
High Intensity Users (HIUs) of Urgent and Emergency Care (UEC) services account for disproportionately high numbers of Emergency Department (ED) attendances, ambulance journeys and non-elective admissions. This review aimed to assess the quality and completeness of evidence for understanding the characteristics of HIUs, how best to identify and differentiate them, the effectiveness of services to support them, and to identify areas for further research.
Design
Scoping review of UK-based peer-reviewed literature.
Setting
Four databases (January 2010 to October 2025) - additional grey literature identified through hand searching and Google searches.
Participants
Twenty-eight published articles (19 peer-reviewed papers, 9 grey literature).
Main outcome measures
HIU definitions, descriptions, effectiveness of care, characteristics of successful programmes and interventions.
Results
HIUs are generally defined by the frequency of UEC use rather than diagnosis or need, despite being highly heterogeneous. The national model of care adopted in England relies largely on individual Case Managers supporting small numbers of HIUs. Although most published evaluations report reductions in ED attendances and admissions, and positive impacts on individual well-being, they are generally small, uncontrolled, and short-term with poorly defined interventions and minimal evidence that they reduce overall demand on UEC services.
Conclusions
Further research is needed to better characterise HIUs, drivers of their behaviour and risk factors to determine which HIUs benefit from which interventions. Services need to operate at scale using near-real time data, be integrated with health as well as social care services, and use standardised, granular definitions of HIUs to guide appropriate interventions.
Introduction
Rationale
High intensity users (HIUs) access urgent and emergency care (UEC) services at a higher rate than the general population 1 with up to 2.1% of people who attend five or more times in one year accounting for over 10% of all Emergency Department (ED) visits.2,3 They have complex needs, high morbidity and mortality rates and generate significant demands on health services, accounting for 10% of NHS UEC costs, 26% of non-elective admissions to hospital and 29% of emergency ambulance conveyances. 3
HIUs are one of the complex cohorts prioritised in NHS England's Neighbourhood Health Guidelines for 2025/2026 4 and both its 10-year Health Plan 5 and UEC Recovery Plan for 2025/2026 6 set requirements for health systems to expand access to UEC services at home and in the community, with an expectation that HIU services are in place to reduce unnecessary hospital visits.
However, there is little consistency in how to define, identify and manage HIUs and weak evidence that services to support them reduce demand on overall UEC activity. We therefore undertook a scoping review to better understand where there are significant gaps in knowledge and what further work may be needed to address them.
Objectives
The aims of the review were to (a) assess the quality of existing evidence; (b) summarise current understanding of HIUs of UEC services; and (c) identify areas where further research is needed.
Although primary care providers face similar challenges, this review focuses solely on UEC services since it would be outside the scope of this study to examine differences between the groups and consider the dynamic interplay between attendance at different settings.
Methods
Protocol and registration
Our protocol was drafted using the Preferred Reporting Items for Systematic Reviews and Meta-analysis Protocols (PRISMA) extension for scoping reviews (https://www.prisma-statement.org/scoping) and registered with the PROSPERO Database on 20 June 2025 (https://www.crd.york.ac.uk/PROSPERO; ref CRD420251076465).
Eligibility criteria
To be included in the review, papers needed to be written in English and examine demographic, attendance and admission data for HIUs attending Urgent & Emergency Care services. Quantitative, qualitative and mixed-method studies were included.
Information sources
We searched PubMed, Ovid, MEDLINE, and the Cochrane Library to identify papers published between January 2010 and October 2025. Results were exported into Excel and duplicates removed by a member of the research team.
Search
The following search terms were agreed:
Emergency, emergency care, emergency healthcare, A&E, accident and emergency, urgent care, urgent care centre, UCC, urgent treatment, urgent treatment centre, UTC. (Combined with “OR”) Primary care, social care, GP, general practice. (Combined with “OR”) Secondary care, admission*, hospital admission*, hospital stay* (Combined with “OR”) Frequent attend*, high intensity use*, HIU, repeat attendance*, frequent caller. (Combined with “OR”)
“AND” 4) “AND” 4) “AND” 4)
Our search criteria did not include predetermined thresholds for UEC use since this was a key area for examination, although we only included relevant papers where such criteria were defined.
Inclusion and exclusion criteria for the review are presented in Figure 1 as per PRISMA guidelines.

Search strategy and results.
Only studies that used predominantly UK-based data were included in the initial search because it is widely recognised that high intensity use of the healthcare system has social as well as medical drivers 3 making this a highly context-specific issue and meaning that comparisons between different countries may not be valid.
Selection of sources of evidence
Three authors initially screened all article titles (II, CP, and SH). Remaining article title, abstracts and full texts were independently screened by four of the authors (CP, II, RW, and PG) for inclusion in the review. Discrepancies were discussed by the screeners until consensus was achieved. Reference lists of included articles were screened for additional relevant studies, and hand searching was also undertaken. Articles were included if they addressed the review aims.
Further relevant articles and grey literature were retrieved by searching Google and hand searching the referenced lists of studies identified through the electronic search. Some of these fell outside the strict criteria described above but were included if they provided additional context and background or highlighted limitations in existing literature.
Data charting process
Each member of the team was allocated a set of papers for potential inclusion in the scoping review. They extracted key findings into a data charting form using MS Word. Each paper was then discussed amongst the whole team to agree which to include and any inconsistencies.
Data items
We abstracted data on definitions, characteristics and risk factors, needs, scale of the issue, models of care and impact of interventions.
Synthesis of results
Given the limited data available, we used the narrative synthesis method to summarise the findings.
Results
Definition
We identified four studies that described approaches to defining HIUs.1,3,7,8 All are based on the number of contacts with UEC services within a set time period, most commonly using absolute numbers of attendances and arbitrary thresholds between three and ten attendances, or four inpatient admissions, within the previous 12 months.1,7,8 A commonly adopted definition is the same individual attending ED five or more times in one year, 3 based on the median of published studies. This approach is pragmatic since it can be applied in real time.
A minority of studies use a percentile of attendances to identify individuals but this approach only works retrospectively so its use in a clinical setting would delay identification of HIUs. 1
Characteristics
We identified eleven papers describing the characteristics of HIUs.3,8,9–17 They are a heterogeneous group of people with complex and often co-existing physical, mental health and social care needs. 9
Demography and social factors
A recent large-scale English study using national datasets identified a trimodal distribution of HIUs with three distinct age peaks centred around those aged 25, 48 and 79 years, each with different clinical and demographic profiles. 10 People aged over 80 years are six times as likely to be an HIU as those under 40 years, 11 with a much higher prevalence of HIUs as a proportion of all ED attenders amongst those aged 65+ years than in other groups. 10
Overall, similar proportions of men and women make up the HIU cohort but with a higher proportion of females (60%) in the youngest (18–34 years) age group. 10 HIUs are more likely to be White British (77%) than other ED attenders, with slightly higher proportions of Asian and Black ethnic groups. 22% live alone compared to 16% of the general population and 18.8% live in the most deprived areas. 3 Younger HIUs (18–34 years) are over 3 times, and those aged 65+ are 1.7 times more likely than other ED attenders of the same age to live in deprived areas.10,12
High proportions of HIUs experience health inequalities such as unemployment, criminality, homelessness, loneliness, anxiety, low quality of life and social isolation. 3 Those referred to Psychiatric Liaison Services are more likely to have previously been detained under the Mental Health Act, to have multiple care coordinators involved in their management, to live in residential care settings and to not be in a relationship. 13
Co-morbidities and presentations
HIUs generally have higher levels of morbidity and mortality than the general population except for those aged over 80 years. Over 70% have two or more pre-existing long-term conditions, with 40% having five or more conditions - more than twice the rate of other ED attenders. 12 HIUs aged over 60 years who attend particularly frequently (more than 15 times annually) also have lower mortality rates than other HIUs. 3
The trimodal age groups show different clinical profiles: elderly HIUs (65+ years) present most frequently with cardiovascular, urinary and respiratory conditions, with high rates of inclusion on palliative care registers (44.5%). Mental health diagnoses and substance misuse are more common in younger and middle-aged groups (18–64 years). 10
65% of HIUs have mental health symptoms, 15% substance misuse problems, and 45% present with medically unexplained symptoms.8,11,14 Specifically, they are much more likely than other patients to suffer from stress/mood disorders, psychoses, personality disorders and learning disabilities. 13 They are also much more likely to have experienced sexual, physical and other forms of abuse in childhood. 15 Reflecting these complex needs, 63% have been prescribed psychotropic drugs, 61% pain medications, and nearly 80% one or both. 10
Challenges for health services
Whilst only 0.67%–2.1% of the English population are HIUs of UEC services, they account for 10.7%–16% of all ED attendances, 29% of all ambulance journeys and 26% of all non-elective hospital admissions in England, with an estimated cost to the NHS of £2.5bn per year.2,3,10 Most (85%) attend ED between 5 and 10 times per year, with only 5% attending 20 or more times. 12 People who attend ED moderately frequently (less than 20 times per year) account for 97% of all HIU attendances. 16 Multisite attendance is uncommon, with over 80% of frequent attenders using only one ED site annually. 10 Over one-third of HIUs have sustained periods of frequent attendance lasting longer than 12 months and those who attend at least eight times in one year have a 56% chance of remaining an HIU for at least 2 years. 3
Local data for North-West London showed that, in 2018/2019, 6300 people who presented more than ten times at EDs accounted for 10% of non-elective and emergency care spending. 99% of them were already in contact with health services – on average three times more likely to be in frequent contact with their GP than other patients. 11
A qualitative study of ten HIUs in South West England suggested that frequent attendance at ED may be driven in part by high levels of anxiety and pain, as well as being influenced by the concerns of family and friends and the sense that ED may be the “best place to be.” 17 Demands on staff are high and lead to increased levels of stress and burnout, impacting on professional and patient satisfaction. 3
Effectiveness of HIU services
NHS England estimate that in March 2025, over 87% of EDs in England had access to a HIU service, based on the first service established in Blackpool, England in 2015 (NHSE HIU Support Pack accessed via NHS Futures). The model involves a dedicated Case Manager working as part of a multi-disciplinary team, regularly identifying the most frequent HIUs and aiming to understand individual drivers for each individual's frequent attendance to identify suitable, targeted interventions to address these. 6 The emphasis is on de-medicalisation, de-criminalisation and humanising needs whilst developing collaborative, integrated support across health and other agencies, aiming to dismantle barriers between physical and mental health care. 8
We identified seven papers that reported on the effectiveness of this model of care.18–24 A study of an ED-based service in Durham & Darlington over a two-and-a-half-year period 18 showed statistically significant reductions of 60% fewer HIUs presenting at ED each month (from a mean of 43 to 17 per month), accounting for 46% fewer attendances. Similarly, an evaluation of four HIU services in different areas of England demonstrated reductions in ED attendances (range: 37%–84%), non-elective admissions (24%–84%) and ambulance service calls (range: 15%–78%) by those HIUs who engaged with the programmes and reported that such services were highly valued by those involved. 19 However, numbers recruited were small (range: 13–79 people) and although each of the services had similar aims, each had been implemented in different ways reflecting local needs and available resources, the existing level of integration of other services and the maturity of data capture systems.
A pilot study of a Case Management service in West Kent also reported improvements in a wide range of measures of physical, social and mental health well-being, but again the study size was very small and unrepresentative of much of the wider UK population. 20
A study at an inner London ED demonstrated significant reductions in emergency admissions, ED attendances and investigations for those HIUs for whom multi-disciplinary care plans had been prepared in advance, but the numbers were small and selection of patients was decided in an ad-hoc fashion by ED staff. 21 A study in West England showed 33% reductions in mean monthly ED attendances and 67% in hospital admissions, although the duration of follow-up was short. 22
A service in Hertfordshire reported a statistically significant 70% reduction in ED attendances over a twelve-month period 23 but involved only 40 patients, mostly with mental health problems, medically unexplained symptoms and substance misuse issues.
The largest published study measured the impact of a social support programme provided across three EDs in the West of Scotland over six years, reporting 31% reductions in ED attendances and 33% in inpatient admission days over the course of one year's follow-up. 24
Table 1 summarises these findings.
Evaluations of HIU services (UK only).

Characteristics of successful programmes
Eleven papers described interventions used to support HIUs,18–20,23–30 broadly falling within the remit of case management, outreach and front-of-door streaming but often based on a variety of poorly defined multi-modal approaches including one-to-one coaching, the co-production of individualised care plans, patient education, counselling and problem solving, information sharing between agencies, help to address psychosocial needs and greater provision of routine community-based services outside ED itself.20,26–28 Whilst there is some evidence on effectiveness of these approaches, the use of mixed methods makes it difficult to analyse the effect of a single intervention and there is little knowledge on which to use in which circumstances, potentially wasting resources if deployed inappropriately.27,28 Complex systems analysis suggests that interventions focused solely on individual frequent attenders may have limited system-wide impact, as frequent attendance patterns remain stable at the population level even when individual patients reduce their use, with new frequent attenders potentially taking their place.25,29
In contrast to specific interventions, various operational factors are described as key to success (although not quantified per se). These include strong leadership; adequate staff training, coaching and support; early identification of HIUs (employing a variety of data sources including referrals from trusted sources); frequent, easy contact with Case Managers with a relatively small caseload of patients (fewer than 60) matched to both number of attendances and complexity of needs; being flexible about the duration of support offered; ensuring a continuum of care rather than discrete packages of support; and ensuring rapid access to person-centred, community-based support underpinned by strong inter-agency and MDT working.18,30
Key challenges include waning stakeholder enthusiasm, the intensity and volume of the workload, dilution of service aims if non-HIUs are referred into the service and the need for support to continue for extended periods. 19 In addition, it can be difficult to identify, recruit and engage HIUs19,20,23 although the use of referrals from trusted services rather than just ED attendance data is considered to help identify those most likely to benefit. 30
The findings are summarised in Figure 2.
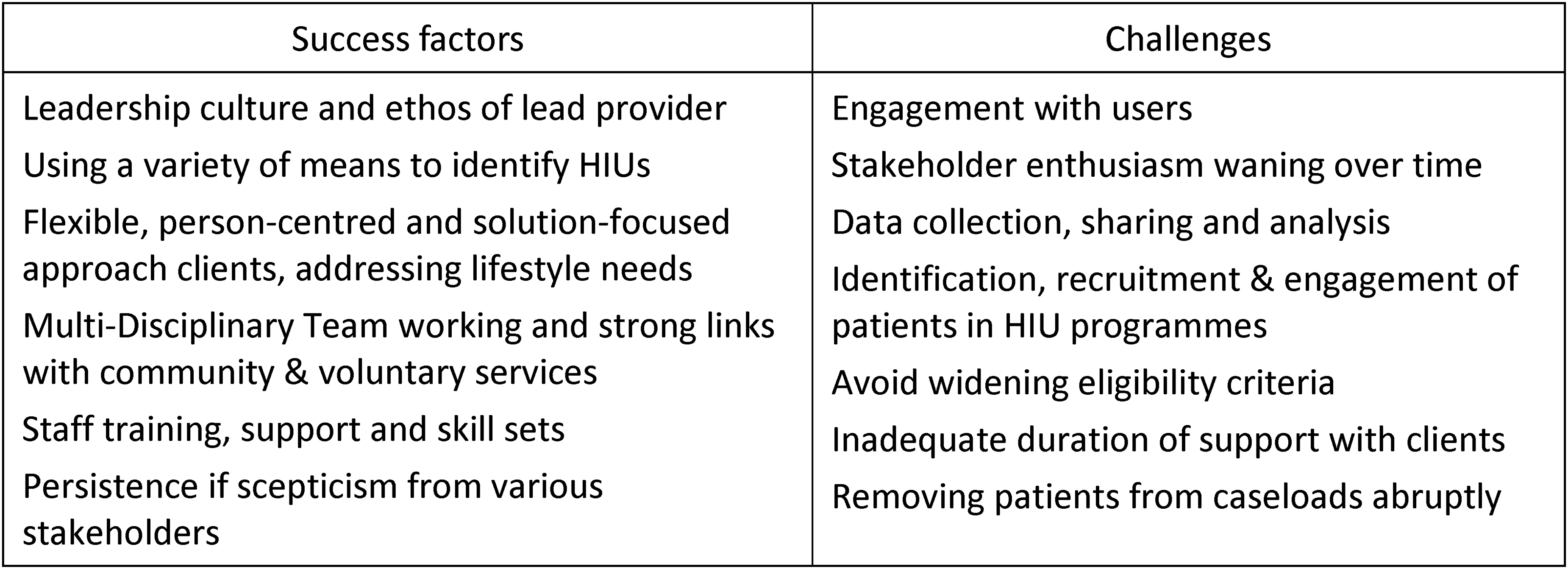
Key strengths and challenges, HIU services.
Discussion
Main findings
This review summarises what is known about the characteristics of HIUs, their impact on UEC systems, the effectiveness of interventions to support them and reported outcomes.
We found a lack of a common definition of or terminology for HIUs. Existing definitions based on the number of attendances fail to discriminate between subsets of HIUs that may have very different needs 16 and clinicians may lack sufficient training to identify specific presenting features that indicate that someone is, or is at high risk of becoming, a HIU. 26
There is evidence that HIU services benefit the individuals who engage with them. Key features appear to be the presence of strong leadership, ongoing staff training and support, effective links with other health and social care services, systems to identify, recruit and engage service users, and secure, long-term resourcing, a lack of which is a commonly reported issue for many services.19,20,23
Reported figures of 40%–80% reductions in UEC usage fail to account for the observation that 56%–63% of HIUs revert to typical patterns of UEC service use within one year3,12 with limited evidence for sustained, system-wide effects, particularly long-term reductions in demand.
This may be because High Intensity Use of UEC is an emergent rather than pre-planned behaviour, driven by the way in which the various parts of the health and social care system interact, rather than just individual choices and behaviour. 29 Attendances follow a power law distribution typical of complex systems, meaning that although an individual's use of UEC services may tail off, another person then occupies their place, overall activity remains unchanged and the health system is no better off.
Notably, this does not seem to apply to older HIUs, suggesting that frailty-related frequent attendance is driven largely by individual rather than system issues. In addition, older people appear to have more complex needs than other HIUs, requiring greater involvement of multi-disciplinary teams 10 and supporting the need to differentiate between different types of HIUs. 16
Quality of published studies
Most published studies of the effectiveness of HIU services are based on uncontrolled, small cohorts, often with specific conditions, with limited length of follow-up. Inclusion criteria vary widely with many subject to possible selection bias and with data drawn from individual hospitals rather than population datasets, meaning that attendances at other sites may have been missed.
Although most use a range of statistical methods to analyse outcomes (most frequently using univariate tests of significance), poorly defined study parameters and a lack of standardised outcomes makes comparison between studies and the use of statistical techniques such as meta-analysis difficult, limiting evaluation of strategies to tackle the issue.
Comparisons with other studies
Previous reviews in this area have focused on particular aspects of the wider problem, for example HIU characteristics, prevalence, or the effectiveness of specific interventions.1,7,15,27,28 This article takes a broader perspective, attempting to synthesise these findings in the context of national policy to attempt to determine whether and how services to support HIUs can be most effective.
Although this review is focused on the UK, similar findings have been reported elsewhere. Various systematic reviews of HIUs in the USA, Canada, Sweden, Singapore, Switzerland, Taiwan and Australia have shown that demographics, prevalence, acuity and attendance patterns reflect those in other industrialised countries with high levels of complex physical and mental health conditions, demonstrating genuine medical need. Insurance status does not appear to be a major determinant of HIU behaviour, suggesting that it is not a product of healthcare system structures or financing models but of the quality and accessibility of healthcare, albeit overlaid by the individual's specific psychosocial and medical needs.31–35 Similarly, there is some evidence internationally that case management interventions lead to reductions in both ED utilisation and costs36–40 but very few studies have rigorously examined the impact of individualised care plans or improved information sharing between providers. 40
Strengths and limitations
We undertook a comprehensive review of peer-reviewed papers published since 2010 examining different aspects of High Intensity Use of UEC services and compared our findings with current guidance on how services to support this group should be designed and delivered in England. We have identified a number of areas where further research is needed to understand the population better, to clarify how best to support them and how to deliver such interventions at scale.
However, there are limitations to our work. We restricted our search to studies of UK populations published since 2010 and, given the inconsistent definitions of HIUs, may have missed papers that looked at specific sub-groups who would otherwise meet our criteria.
Our analysis of studies that report outcomes may have been skewed by publication bias towards services that achieved positive results, and the lack of standardised recruitment criteria, settings, interventions and outcome measures means that our general findings may lack specificity.
Nonetheless, there appears to be considerable agreement across published reviews and studies about where there are gaps in research findings and where greater clarity on effectiveness is needed, both nationally and internationally, so we feel that our conclusions are likely to be valid and generalisable.
Implications (policy and practice)
The national model for HIU services is based on individual Case Managers providing direct 1:1 support to a caseload of up to 50 of the most frequent attenders at EDs at any one time, with a significant number needing support for many months. 19 The approach is difficult to scale and implicitly equates an individual's needs with their impact on the system (number of attendances) but HIUs are a highly heterogeneous group whose sub-cohorts may benefit from different interventions. Prioritising them for support based on service usage may not be the most effective, equitable or efficient use of resources. In addition, the focus of the national model on a demedicalised model of case management, whilst probably a key component of care for many HIUs, does not address system-wide issues such as redesigning how services can be better organised to facilitate access to essential medical care in an appropriate and timely fashion.
More research is needed to develop standardised, more granular definitions of HIUs, incorporating factors associated with HIU behaviour such as mental health, substance misuse and chronic diseases 16 and which interventions are best suited to which groups. 27 Machine Learning approaches can help identify HIUs and related risk-factors more accurately 41 which could underpin the development of more tailored services based on individual risk and benefit, enable cohorts to be streamed more effectively and ensure that interventions are targeted appropriately and effectively, adjusted to fit locally agreed service needs, local population characteristics and available community health and social care services.
Such population health management approaches to case finding, based on risk-stratified, proactive identification of patients, would enable earlier, more timely targeting of high-impact interventions.3,11 Technology such as population health dashboards, shared care records and business intelligence tools can facilitate this, but lengthy processes to obtain regulatory approval, the need for new governance arrangements and issues with missing data can hinder access to full datasets 8 although data anonymisation and data sharing agreements have been effectively used to mitigate some of these issues. 19
Based on the findings of such research, commissioners should ensure that HIU services are:
System-wide and fully integrated with established health as well as social care systems Delivered at scale, with sufficient capacity to handle the numbers of HIUs who can benefit; Equitable, based on individual as well as service needs; and Dynamic, underpinned by near real-time, continuously updated data systems
Given the high absolute numbers 11 and turnover 31 of HIUs, such evidence would also help to identify the scale and nature of resources needed to manage sub-groups of HIUs with different needs outside Urgent & Emergency care settings.
Conclusions
HIUs are a vulnerable group of people with widely varying health and social care needs who have a disproportionate impact on UEC services. Notwithstanding the need to provide HIUs with better support on grounds of need, equity and as a Public Good, effective services would have huge benefits for the wider health and social care system, releasing UEC capacity, making better use of existing resources and identifying opportunities to redesign systems with benefits to the whole population.
As such services are developed, they need to be evaluated through large-scale, randomised controlled trials for specific, well-defined cohorts of HIUs allied with system-wide evaluations of the impact on wider population health as well as reductions in attendances or admissions, whilst accounting for local and regional differences in service configuration and local population characteristics.
Footnotes
Acknowledgements
We are grateful to Professor Azeem Majeed, Dr Alex Thomson and Jason Scott for reviewing and commenting on various drafts of this paper. Imperial College London is grateful for support from the NIHR Applied Research Collaboration (ARC) NW London and the Imperial NIHR Biomedical Research Centre. The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study was a literature review of published research. No patients or staff were interviewed or approached during this study and no patient identifiable data was examined. The project was considered to be a service evaluation without the need for ethical review.
Guarantor
PG acted as guarantor for the study.
Contributorship
PG and II are joint first authors. The study concept was developed by PG and SH. The manuscript was drafted by PG and II, and critically revised by CP and RW. The search strategy was developed by and initial screening undertaken by CP, SH and II. Study selection, data extraction, and quality assessment were performed by PG, II, CP and RW. All authors read and approved the final version of the manuscript.
Provenance
Not commissioned: peer reviewed by Julie Morris and Peter Greengross.