
Abstract
Objectives
This study aims to quantitatively assess the baseline level of self-perceived cultural competency preparedness and skillfulness among medical and health professions students from 21 universities around the world utilizing a previously validated and standardized testing tool.
Design
Cross-sectional study.
Setting
The International Collaboration and Exchange Program (ICEP), a global exchange initiative for junior medical and health professions students spanning 21 universities across four continents.
Participants
A total of 753 students from the 2021 and 2022 ICEP cohorts.
Main Outcome Measures
Students self-evaluated their cultural competency skills on a 5-point Likert-type scale encompassing different areas of competency. Multiple linear regression was performed to identify contributors to cultural competency levels.
Results
Upon rating how skillful they are at interacting with culturally diverse patients, North American students reported the highest scores with a mean of 3.22, while Australian students showed the lowest score of 2.82. When analyzing students’ stages of study, those in clinical years of medical schools scored the highest at 3.29. Significant variations were observed in the cultural competency self-rating scores among students based on their respective regions (p < .005) and program types/stages (p < .05). Notably, students in their clinical years of school consistently rated themselves higher compared to their preclinical counterparts (p < .05). Furthermore, students from Europe displayed elevated self-ratings compared to the other regions (p < .005).
Conclusions
Though these participants represent a highly motivated subgroup of students, potentially limiting result generalizability, the findings emphasize that regional differences exist. Given the multifaceted nature of cultural competency, the results suggest that factors such as educational stage, age, and region may influence students’ perceived competency levels.
Keywords
Culture plays a large role in how healthcare operates and is experienced by various cultural groups. Because cultural factors can influence the recognition and communication of clinical symptoms, the threshold for seeking care, the understanding of prescribed management strategies, and the expectations of care, it can equally impact morbidity and mortality, as well as the outcomes of medical care.1,2 Studies have shown that minority populations in the USA tend to suffer disproportionately from healthcare disparities.3,4
While the evidence pointing towards the existence of these healthcare disparities is clear, it remains unclear how these problems should be solved. Within the last decade, there has been a growing emphasis on cultural competence as a way to improve care quality, patient outcomes, and satisfaction for minority populations. 1 In the context of healthcare, cultural competence refers to an individual's ability to deliver high-quality care to patients from diverse backgrounds.4,5 To reflect this evolving need in the USA, major organizations such as the US Institute of Medicine (now National Academy of Medicine), the Liaison Committee on Medical Education, and the Accreditation Council for Graduate Medical Education have emphasized cross-cultural education, in response to which medical schools incorporated a greater focus on cross-cultural care in their curricula.4–8
With the internationalization of higher medical education and the emphasis on producing globally competent physicians who deliver healthcare in a complex and interconnected world, the need for cross-cultural education becomes more apparent. Moreover, the proportion of foreign-born residents has steadily increased, with regions like the USA and Europe reporting approximately 15%, and Canada and Australia around 25% in 2015. 6 This has led to cultural competency training being incorporated within many medical school curricula worldwide. 1 This training differs vastly from region to region depending on local factors that inform such teaching. There is also variability in the timing of training, with many medical schools emphasizing cultural competency and cross-cultural care in the first or second year, without integration across the four-year continuum. 1 Further, the ‘hidden curriculum’ – the informal lessons learned by students through interactions with faculty, residents, patients, and staff – strongly influences students’ attitudes and perspectives, and likely plays a role in how they learn about cross-cultural care.1,9 Therefore, approaches and content vary widely, and there is a paucity of research evaluating the quality of such training.
Moreover, many medical students do not feel sufficiently prepared to treat and care for patients in a cross-cultural setting.10,11 Standard methods of cultural competency evaluation are lacking, making assessment of the quality of education challenging. 10 While studies from the USA 11 and other countries12–14 exist, little is known about the global comparison of baseline levels of cultural competency preparedness among students in various health professions.15,16 Obtaining these data is important to guide medical educators on how and to what extent cross-cultural care needs to be included in medical curricula around the world. This ensures the effective delivery of healthcare to culturally diverse populations by addressing challenges such as differing communication and explanatory styles, conceptions of health and illness, and linguistic barriers.17,18 Failure to overcome these barriers may result in reduced comprehension and adherence to medical instruction, ultimately leading to poorer health outcomes.
The aim of this study was to assess the baseline level of cultural competency in medical and health professions students at 21 universities worldwide, utilizing a previously validated and standardized testing tool (Cross-Cultural Care Survey). 19 The study examined the degree of concordance between medical and health professions students’ self-perceived cultural competency skills and levels of preparedness in different contexts. Results from this study could help medical educators assess the extent to which cultural competency training should be included in health professions education curricula, and aid in the standardization of shared medical curricula, globally. This is particularly important in a time of growing global mobility, both physical and virtual, which will increase cross-cultural interactions between healthcare workers and patients.
Materials and methods
Participants
Participants from the International Collaboration and Exchange Program, an international student networking and exchange program designed for health professions students, originated from within the context of the anatomy course, created to prepare students to be active leaders in global collaborative problem-solving in healthcare. 20 At the time of this study, International Collaboration and Exchange Program has partnered with 21 major leading medical universities on four continents: Asia, Australia, Europe, and North America. Following Institutional Review Board approval (Columbia University IRB # AAA0003715 plus ethical waivers from other participating schools), the online questionnaire collected 753 valid responses from participants of two cohorts in June 2021 and June 2022.
Details of the participant demographics are presented in Table 1. Although most schools were located in Australia, North America, or Western Europe, the student cohorts included some international, refugee, immigrant, and first-generation students from other parts of the world (Northern and Sub-Saharan Africa, Southeast Asia, the Middle East, South America, and Eastern Europe) and represented a very diverse student body. All students were fluent in the English language as part of the program participation requirements.
Demographic characteristics by global region..

Note: Some students did not answer all of the survey questions, resulting in variations in the total response counts. Global Region Codes: Australia (AUS), East Asia (EA), Europe (EUR), and North America (NA).
Questionnaire
This study utilized the Cross-Cultural Care Survey, a questionnaire by Weissman et al. that has previously been validated with medical residents and modified for undergraduate medical students. 19 This tool was most recently adapted by Green and colleagues from Harvard Medical School where they added items to assess students’ preparedness to care for patients who identify as (1) gay, lesbian, or bisexual, (2) transgender, and (3) persons with disabilities. The skillfulness scale was slightly modified by including an item on counseling patients on their use of complementary or alternative medicines and removing references to the ‘pediatric patient's family’. 11 The students were administered the survey before the start of the program as a regular component of their participation in International Collaboration and Exchange Program.21,22 The survey was conducted in English and was administered using the Qualtrics XM (Seattle, WA) online survey software. The final 59-item questionnaire collected broad experiences with cultural competence during clinical and training through multiple choice, rating, and open-ended questions. Two constructs related to cross-cultural care were examined: (1) preparedness to care for specific types of patients and (2) self-assessment of specific cross-cultural skills.4,11,23
The survey questions were grouped and analyzed into four distinct metrics. The first metric assessed students’ general preparedness to care for patients. The second metric assessed their preparedness to care for patients from diverse backgrounds, including those with cultures differing from their own, health beliefs at odds with Western medicine, distrust of their health care system, limited majority language proficiency, religious beliefs that affect treatment decisions, complementary or alternative medicine beliefs, racial and ethnic minority status, disabilities, and patients who are gay, lesbian, bisexual, or transgender. 24 For each question, students rated their level of preparedness on a scale ranging from 1 (very unprepared) to 5 (very well prepared).
The third metric asked students to assess their skill level in performing certain functions thought to be useful in caring for culturally diverse patients (1 = not at all skillful; 5 = very skillful). These included determining how a patient wants to be addressed and interacted with, taking a social history, assessing the patient's understanding of the cause of their illness, identifying whether a patient is mistrustful of the health care system or the physician, negotiating with the patient about key aspects of the treatment plan, identifying how well a patient can read or write in the majority language, identifying religious beliefs that might affect clinical care, identifying cultural (non-religious) customs that might affect clinical care, working effectively with a medical interpreter, and counseling patients about their use of alternative or complementary medicine. Skillfulness was also assessed as a composite score by summing respondents’ answers for each of the ten items, with higher scores indicating a higher level of skillfulness. 11
The fourth metric asked students to self-evaluate their cultural competency skills before participating in International Collaboration and Exchange Program on a 5-point Likert scale (1 = none; 5 = a lot).21,22 The question encompassed different areas of competency: Knowledge (self-knowledge, culture-specific knowledge, understanding others, etc.); Intrapersonal Skills (self-judgment inhibition, critical thinking, culture detection); Interpersonal Skills (interaction with others); Internal Outcomes (adaptability, empathy, frame of reference); External Outcomes (relations to others, interactions with others, integration, collaboration, prevention, non-discrimination); and Attitudes (respect, tolerance, equality of cultures, etc.).
The questionnaire also collected student demographic characteristics, including age, gender, type of student, and clinical years. The data were stratified by global region – Australia, East Asia, Europe, and North America. This was deemed necessary due to an uneven distribution of students from different countries and schools.
Statistical analysis
The data was analyzed using RStudio version 2023.03.0 + 386. To assess the relationship between cultural competency levels and various predictors, such as age, gender, region of origin, and educational stage, a multiple linear regression analysis was conducted. To further explore differences between specific groups within categorical variables, pairwise t-test comparisons were utilized. Adjustments for multiple comparisons were applied using the Benjamini-Hochberg procedure to control for the false discovery rate. A p-value of ≤ .05 was used as the threshold of statistical significance.
Results
Participant characteristics
All 774 students enrolled in International Collaboration and Exchange Program were required to participate in the study. This resulted in an overall 100.0% response rate, although not all students answered every single question, leading to only 753 valid responses. The majority (51.0%) of participants were between the ages of 20 and 25. Additionally, the majority (61.8%) of participants were female. In terms of the type of academic program students were enrolled in, 52.1% of participants were students in medical school. Lastly, students were categorized based on the stage of clinical training they were in, with 68.1% of students in their preclinical years of medical school.
Table 1 shows the distribution of demographics by global region. Table 2 shows the distribution of participants by university, country, and geographic region.
Distribution of participants by university, country, and geographic region.
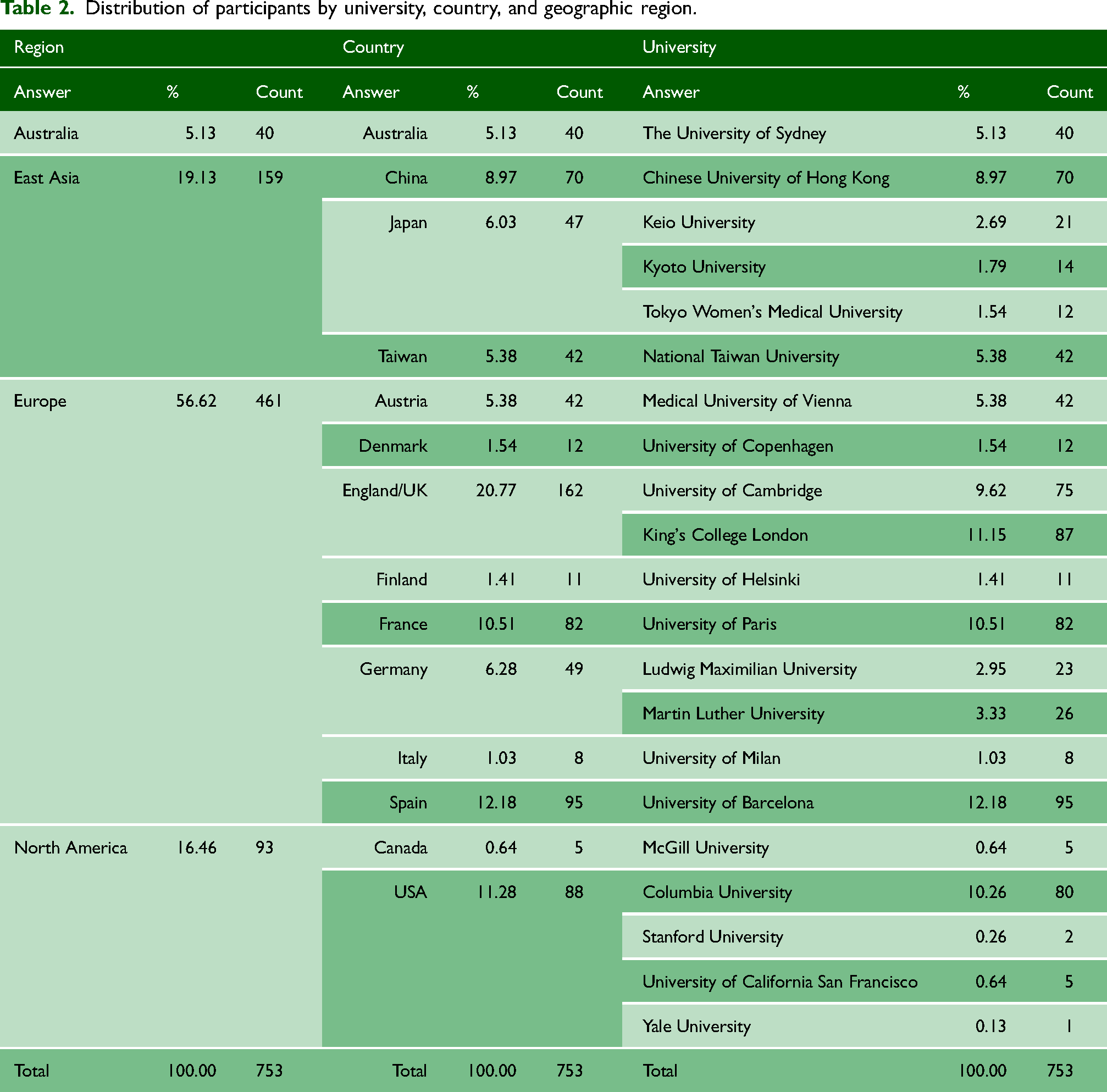
Table 3 shows the four measures of students’ self-reported ratings stratified by demographic data and program type/stage. Table 4 further displays the students’ self-reported ratings stratified by country. Regarding general preparedness, the average score across every region was 2.90 (SD = 1.01); 4.1% of students felt ‘very well prepared’, while 24.0% felt ‘well prepared’. The average score for preparedness to care for patients from diverse groups across every region was 2.88 (SD = 1.15); 29.9% of students felt either ‘very well prepared’ or ‘well prepared’. For skillfulness at interacting with patients from diverse groups, the average score across every region was 3.09 (SD = 1.10); 37.5% of students felt either ‘very skillful’ or ‘quite skillful’. For levels of cultural competency before the program, the average score across every region was 3.82 (SD = 0.87).
Average self-ratings by demographic information and program type/stage. Values are reported as mean and standard deviation.

Average self-ratings by country. Values are reported as mean and standard deviation.

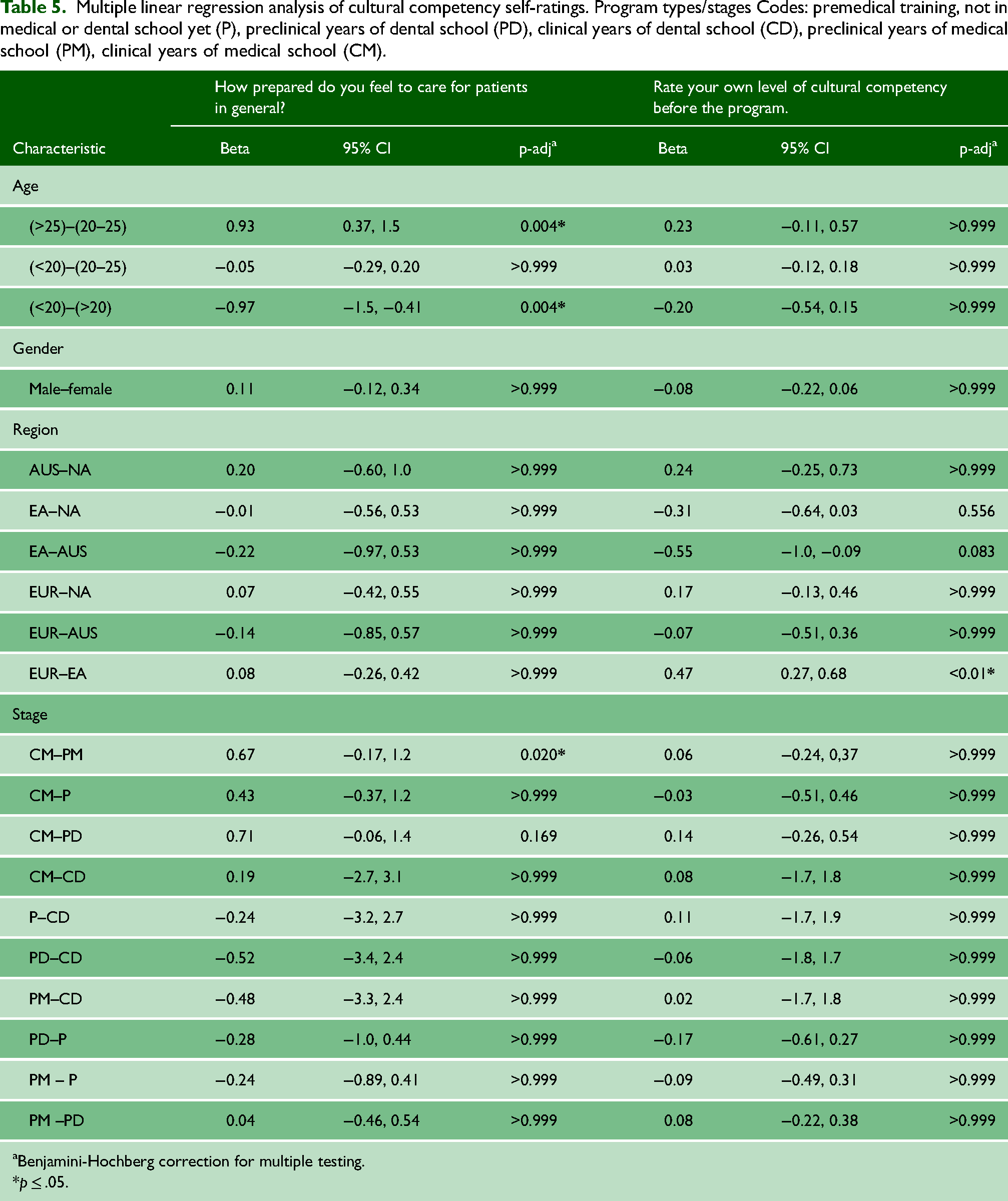
Table 5 displays the results from the multiple linear regression analysis, indicating the influence of age, gender, region, and clinical stage on self-reported cultural competency levels. The results revealed that age and clinical stage significantly influenced students’ perceived general preparedness to care for patients. Older students and those in the clinical years of medical school were found to have higher levels of general preparedness. Additionally, students from the EUR region self-reported higher levels of cultural competency, particularly when compared to their EA counterparts. None of the variables demonstrated a statistically significant impact on students’ self-rated preparedness and skillfulness when providing care or interacting with culturally diverse groups.
Multiple linear regression analysis of cultural competency self-ratings. Program types/stages Codes: premedical training, not in medical or dental school yet (P), preclinical years of dental school (PD), clinical years of dental school (CD), preclinical years of medical school (PM), clinical years of medical school (CM).
Benjamini-Hochberg correction for multiple testing.
p ≤ .05.
Discussion
Studies of cultural competencies are typically conducted with limited student populations, typically in only one region or country.4,11 This study is one of very few that capture a large global student population, though it may primarily reflect a highly motivated and engaged subgroup of students. Integrated skills such as cultural competency are harder to capture and compare between different regions of the world because of the unique contexts that exist in each. By using a validated questionnaire, 15 the present data can provide a valuable representation of a global snapshot on this topic. This snapshot is important, as with increasing globalization, medical professionals must be equipped with similar competencies. Moreover, global medical curricula that aim to provide equitable education will need to include training modules that are adapted to different regions’ needs. 25 Answering this question would help to develop more robust training programs in the future.
The findings revealed significant variations in self-reported ratings of cultural competency across global regions. Students in Europe generally reported higher levels of cultural competency compared to students from other global regions, particularly East Asia. These differences could be attributed to variations in educational philosophies, cultural backgrounds and values, exposure to diverse populations, and regional priorities. A similar study evaluating cultural competence across various global regions revealed findings consistent with this study. In their study, nurses from Anglo-Saxon countries (the USA, the UK, Australia, NZ, and Canada) achieved the highest mean cultural competence scores. They were followed by those born in other European countries, while nurses born in Asian countries reported the lowest scores. 17 These findings may be attributed to the larger multicultural communities in Anglo-Saxon countries compared to their Asian counterparts. 26 In some Asian countries, such as Japan, there is a noted lack of understanding and familiarity with the concept of cultural competence. 27
Navigating cultural differences and overcoming communication barriers are essential to ensuring that necessary care is optimally conveyed, leaving no room for misinterpretation. Challenges often arise due to linguistic differences, effectively utilizing interpreter services, and variations in verbal and nonverbal communication styles. 18 Additionally, patients’ cultural beliefs about health and illness can influence their acceptance of and adherence to medical advice. Evidently, traditional healing practices, such as the use of herbal remedies, can potentially conflict with Western treatments, leading to adverse interactions. 18 These challenges can only be effectively addressed when healthcare providers are aware of cultural nuances and take the time to explain treatment options and their benefits in a culturally sensitive manner.
Research indicates that the leading factor that contributes to students feeling culturally competent was their life experiences preceding medical school. 28 Moreover, individuals’ cultural contexts, encompassing familial upbringing, religion, educational background, social status, and nationality, play a profound role in shaping their perspectives and behaviors. 29 Intercultural interactions have also been instrumental in developing cultural competence, 28 and diverse classrooms have been shown to enhance the students’ learning experiences, which can vary across geographic regions. Additionally, studies have shown that students who study with students from different backgrounds and participated in a greater number of diversity-related extracurricular activities were associated with preparedness to work with patients from diverse backgrounds. 30
The results also displayed significant differences in self-ratings across program types and stages as well as age. Students in their clinical years of medical school consistently rated themselves higher in general preparedness compared to those in their preclinical years as expected. However, cultural competency levels showed no variation between students in the early and later stages of their education.
Contrastingly in previous studies, it has been indicated that older students had significantly higher levels of cultural competence compared to their younger counterparts. This observation is likely attributable to older students benefiting from greater exposure to their program's curricula as well as the opportunity to participate in intercultural learning experiences. 30 Additionally, students in their clinical years may have more exposure to diverse patient populations. These clinical experiences and multicultural teachings that more senior students partake in have been identified as contributing factors to the enhancement of cultural competency. 30
Limitations
This study has several limitations. First, the sample was drawn from only a few higher education institutions in each global region using a purposive sampling strategy. Therefore, the results cannot be considered wholly representative of specific countries or regions. Moreover, students who chose to participate in this program are likely more interested in this topic and thus may be more culturally competent than others at baseline.
Self-reported ratings of cross-cultural skills and preparedness may not be reflective of a student's skills and preparedness in practice. However, there is evidence correlating self-assessment with actual skills among medical students. 11 Also, short, written responses to an open-ended question or semi-structured interviews may offer a more effective approach to obtaining a more nuanced and holistic picture and should be considered for future research.
Another critical consideration is that the data collected in this study were cross-sectional, only taken at the beginning of International Collaboration and Exchange Program. The authors intend to resend the questionnaire post-program to detect the development of cultural competency in participants. These data will assess the curriculum of International Collaboration and Exchange Program as an intervention in medical and health professions’ students’ education and guide future enhancements.
Conclusion
In conclusion, the study found that most students do not feel comfortable tending to diverse patients by the pre-clinical or clinical stages, indicating that there is still room for improvement of cultural competency among junior health professions students. These data are specifically unique, in that this global comparison revealed that most global regions can benefit from cultural competency training for students as part of health professions school curricula. While this study is only a snapshot of one cohort of students at the point in time before they started International Collaboration and Exchange Program and does not follow students longitudinally, it offers valuable understanding of where students are in terms of cultural competency, globally. Health professions education researchers around the world should continue to evaluate these competencies in all students and settings. Institutions should also address the efficacy of current training programs and amend the current strategies in training cultural competency. As a result, patients across continents will benefit from culturally competent providers who consider the patient's personal context and acknowledge their lived experiences in the development of treatment plans and care.
Footnotes
Acknowledgements
The authors express gratitude to the participants of the ‘International Collaboration and Exchange Program – Preparing Global Leaders for Healthcare’. We would also like to thank the ICEP faculty members: Richard Wingate (King's College London, UK); Chung-Liang Chien (National Taiwan University, Taiwan); Hannes Traxler (Medical University of Vienna, Austria); Jens Waschke and Anna Sigmund (Ludwig Maximilians University, Germany); Takeshi Sakurai and Yukari Yamada (Kyoto University, Japan); Mina Zeroual (McGill University, Canada); Jorgen Olsen (University of Copenhagen, Denmark); Salma El-Batti (University of Paris, France); Suvi Viranta-Kovanen (University of Helsinki, Finland); Kevin Keay (The University of Sydney, Australia); Shuji Kitahara (Tokyo Women's Medical University, Japan); Nieves Martinez-Abadias, Alfons Navarro Ponz and Josep Maria de Anta Vinyals (University of Barcelona, Spain); Jill Helms (Stanford University, USA); Chiarella Sforza and Nicoletta Gagliano (University of Milan, Italy); Madeleine Norris and Derek Harmon (University of California San Francisco, USA); Yae Kanai (Keio University, Japan); Sammi Lee (The Chinese University of Hongkong, People's Republic of China); Dana Stearns and Sabine Hildebrandt (Harvard Medical School, USA); Ariella Lang and Michael Joseph (Columbia University, USA); Leo Buehler (University of Fribourg, Switzerland); Mark Hardy, Snehal Patel and Paulette Bernd (Columbia University, USA); and Heike Kielstein (Martin Luther University Halle-Wittenberg, Germany). Lastly, the authors would also like to thank AMEE, an International Association for Health Professions Education, for allowing a preliminary version of this work to be shared at the 2022 AMEE Conference in Lyon, France.
Declarations of conflicting interests
The authors declare that there is no conflict of interest.
Funding
No funding.
Ethical considerations/consent to participate
The Ethics Committee of Columbia University waived the need for ethics approval and patient consent for the collection, analysis and publication of the retrospectively obtained and anonymised data for this non-interventional study.
Contributorship
Anette Wu contributed to conceptualization; supervision; writing–review and editing. Radhika Patel contributed to data curation; formal analysis; visualization; writing–original draft; writing–review and editing. Jason Luong contributed to data curation; formal analysis; visualization; writing–original draft; writing–review and editing. Sean McWatt contributed to Conceptualization; supervision; writing–review and editing. Rahul Goel contributed to data curation; formal analysis. Cecilia Brassett contributed to conceptualization; writing–review and editing. Jane Dutton contributed to conceptualization; writing–review and editing. Mandeep Gill Sagoo contributed to conceptualization; writing–review and editing. Carol Kunzel contributed to Conceptualization; writing–review and editing. Alexander Green contributed to conceptualization; supervision; writing–review and editing. Geoffroy Noel contributed to conceptualization; supervision; writing–review and editing.
Guarantor
Anette Wu is the guarantor for this paper.
Provenance
Not commissioned; peer-reviewed by Julie Morris and Caroline Kamau-Mitchell.