
Abstract
People experiencing homelessness (PEH) face significant barriers to primary care, compounded by stigma from healthcare professionals. Health professions education offers a critical window of time to shape attitudes, yet research suggests these attitudes can worsen during training. A cross-sectional survey at a multi-professional graduate institution assessed attitudes toward PEH among students and educators across seven health professions colleges. Attitudes varied significantly by profession, with osteopathic medicine and graduate nursing reporting more favorable views than pharmacy, veterinary medicine, dental medicine, physician assistant studies, and physical therapy. More positive attitudes were associated with greater physical comfort, more frequent prior experiences with PEH, and higher interest in learning about homelessness. Respondents who expressed interest in receiving more information afterwards also scored significantly higher on attitude measures. Findings suggest that targeted, profession-specific educational interventions that emphasize meaningful exposure to PEH may improve attitudes. Integrating experiential learning alongside didactic content could foster more holistic, equitable care across disciplines.
Keywords
Introduction
People experiencing homelessness (PEH) are at increased risk for poor health outcomes. PEH demonstrates higher rates and complexity of illness, higher prevalence of multimorbidity, and a 12-year difference in life expectancy.1,2 PEH also experience higher rates of mental health disorders, including major depressive disorder and generalized anxiety disorder, higher risk for sexually transmitted diseases, and higher rates of chronic conditions, including tuberculosis, diabetes, and HIV/AIDS.1,3 With a higher burden of multimorbidity, PEH have a strong need for primary care services, yet are less likely to seek care due to a variety of barriers, including health insurance gaps, lack of transportation, negative previous experiences, lack of trust, perceived provider stigma, and competing priorities such as seeking employment, food, or shelter.4–6 PEH report being denied care for their mental illness, chronic pain, and addictions after clinicians became aware of their housing status. 7 Negative attitudes from health professionals create stigmatizing barriers to accessing healthcare, such as the assumption of drug-seeking behavior. 7 Barriers to primary care contribute to the increased rate of emergency department use by PEH, up to 2.5 times higher than use by housed persons. Super-utilization of healthcare services, leading to frequent hospitalizations, results in extremely high annual per-person costs.6,8,9
Attitudes of healthcare providers toward PEH may intersect with racial and ethnic biases, which have been shown to affect clinical decision-making and negatively impact health outcomes. 10 Fortunately, implicit and explicit biases are malleable during health professional education, making it an ideal time for intervention.11–16 However, this malleability can paradoxically result in negative attitudes toward PEH. In one study, medical students’ attitudes toward homelessness measured before starting medical school significantly worsened when measured after a 4-year medical education, but were still positive overall. 17 When compared directly in a single practice setting, physicians and residents also tend to demonstrate positive attitudes, but less positive relative to medical students.9,18,19 Moreover, medical students often believe that attending physicians view PEH as less worthy of medical care. 18 While medical students tend to demonstrate more favorable attitudes toward PEH, they still express anticipated discomfort with providing care to them.19–21 This suggests that there may be a process of bias creation in health profession education, which could potentially be modified if specific practices were identified. Because practices vary across specialties and professions, there is significant impetus to investigate differences in health education models and bias across specialties and professions, to determine which educational interventions would mitigate provider bias toward PEH. Previous studies have focused on individual specialties or on a single profession. To date, attitudes of multiple health professions have not been studied.
Our primary objective was to investigate differences in attitudes toward PEH among students and educators of different graduate health professions colleges. Our secondary objective was to contribute to the advancement of holistic interprofessional education by informing decision-makers on directed interventions designed to improve health outcomes for PEH. Therefore, we framed our study findings using the Holistic Learning Theory, which conceptualizes learning as a change in consciousness occurring as a result of instruction, experience, and reflection, as well as a progression toward performing intelligent acts that nurture oneself, others, and one’s environment. 22
Significance Statement
WHAT IS ALREADY KNOWN ON THIS TOPIC—Homelessness is associated with poor health outcomes and lower usage of primary care services, due in part to perceived stigma by healthcare providers. Interprofessional care is increasingly important due to the inherent complexity of health conditions that exist in people experiencing homelessness (PEH). Unfortunately, attitudes toward PEH may worsen during the education of health professionals.
WHAT THIS STUDY ADDS—This study found that attitudes toward PEH differ between health professions students and educators and that positive attitudes are associated with more frequent experiences with PEH, physical comfort with PEH, and interest in learning more about PEH.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE, OR POLICY—Profession-specific investigation and intervention should be facilitated during education with more direct experiences to increase physical comfort and interest in learning more about PEH.
Materials & methods
A survey-based, cross-sectional study was conducted at Western University of Health Sciences (WesternU), a multi-professional, graduate-level academic institution in Pomona, California, following approval from its Institutional Review Board for the Protection of Human Subjects (IRB) on August 7, 2023 (IRB #2020292-1).
Sample
Students and educators were recruited via convenience sampling from eight colleges at WesternU. The colleges included osteopathic medicine, graduate nursing, podiatric medicine, dental medicine, health sciences (physical therapy & physician assistant), optometry, pharmacy, and veterinary medicine. Inclusion criteria required participants were (a) enrolled as a student or employed as an educator at WesternU at the time of distribution and (b) aged 18–65 years at the time of distribution.
A power analysis using G*Power version 3.1.9.7 23 found that the required sample size to achieve 80% power to detect a small-to-medium effect (Cohen’s f = 0.15) at a significance criterion of α = 0.05 was N = 612 for one-way analysis of variances (ANOVA) comparing attitudes toward PEH across seven groups (professions).
Survey
The 19-item Health Professional’s Attitudes Toward the Homeless Inventory (HPATHI) 24 was used to measure attitudes toward PEH among health professionals (Appendix 1). Wording specific to physicians was changed to be applicable to all healthcare professions, including changing “doctors” to “Healthcare providers” in item 12 and “medicine” to “health care” in item 13. Participants rated the extent to which they agreed with each statement (e.g. “Homeless people are victims of circumstance.”) on a 5-point scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). HPATHI scores were formed by summing the responses to all items, with higher scores indicating more positive attitudes toward PEH. The HPATHI items have demonstrated good internal consistency reliability (e.g. Cronbach’s alpha = 0.88). 24 The HPATHI has also been adapted and validated for use with multiple health professionals (e.g. medical students, resident physicians, physicians, physician associate students, nursing students, and nursing staff) in the United States and in different languages (e.g. Spanish).20,21,24–27
Our survey included items that aimed to measure three dimensions of the Holistic Learning Theory as they pertain to attitudes toward PEH: (1) physical comfort; (2) frequency of past experiences; and (3) interest in learning more. Physical comfort providing care to PEH within one’s scope of practice was assessed with a single item (“I would feel just as comfortable physically touching and interacting with a patient experiencing homelessness as any other patient such as administering a physical exam, treatment, or similar service common to your profession.”), rated on a 5-point scale from 1 (“strongly disagree”) to 5 (“strongly agree”). Frequency of past experiences was assessed with a single item (“Over your lifetime, how often have you had significant personal or professional interaction with people experiencing homelessness?”), rated on a 5-point scale from 1 (“never”) to 5 (“always”). Participants’ interest in learning more was assessed with a single item (“How interested would you be in receiving a short document on best practices for caring for homeless patients?”) rated on a 5-point scale from 1 (“not interested at all”) to 5 (“extremely interested”). Demographic measures included age, gender, race and ethnicity, profession, student/educator status, and years of profession (calculated from the first year of graduate school). Age was categorized into groups (20–21, 22–23, 24–26, 27–29, 30–34, 35–39, 40–49, 50–64) based on the distribution of the study population to facilitate analysis and interpretation.
This study is reported in adherence to The Strengthening and Reporting of Observational Studies in Epidemiology Statement. 28
Implementation
The survey was distributed on a Qualtrics platform via flyers and emailed to all classes by the respective academic deans via listserv, with a total approximate reach of 3700 students and 1100 educators and staff during the Fall of 2023. Incentives were offered in the form of a raffle for one of three $50 Amazon gift cards. Study responses were anonymized before being stored and without human knowledge or intervention. Consent to participate was displayed, and participants were required to acknowledge it prior to beginning the survey. Information about resources available to individuals who may experience emotional distress when completing the survey was provided in the consent statement.
Analysis
The internal consistency reliability of the HPATHI items was assessed with Cronbach’s alpha. Though the HPATHI has validated sub-scales in addition to its composite score, only the composite score was used in this study because our primary interest was in general attitudes of health professionals toward PEH. One-way ANOVAs, or Welch’s ANOVAs where the assumption of homogeneity of variances was violated, were used to compare HPATHI scores across health professions and across racial/ethnic groups. If the ANOVA was significant, Tukey’s Honestly Significant Difference (HSD) or Games-Howell tests were used to identify specific group differences. An independent samples t-test was used to compare HPATHI scores between students and educators. Spearman’s rank order correlations were used to examine the associations between HPATHI scores and each of the following: physical comfort with PEH, frequency of experiences with PEH, interest in learning more about homelessness, and demographic variables, as well as the additional three items described above. Participants with missing responses were excluded only from analyses for which those specific data were required, rather than from the entire study. All analyses were conducted using IBM SPSS Statistics software version 29.0.2.0 (IBM Corp., Armonk, NY, USA), 29 and all statistical tests were conducted using a two-tailed alpha level of 0.05.
Results
Six hundred fifty-five individuals responded to at least one item of the survey (13.7% response rate), and 532 respondents completed the full survey (81.2% completion rate). The most common age of respondents was 24–26 (39.7%) and 27–29 (20.3%). The sample included 491 (92.3%) students and 41 (7.7%) educators. Two hundred (37.7%) respondents self-identified as Asian, 171 (32.3%) as White, 62 (11.7%) as Mixed Race, 52 (9.8%) as Hispanic or Latino, and 11 (2.1%) as Black or African American (Table 1).
Comparison of HPATHI scores across groups.
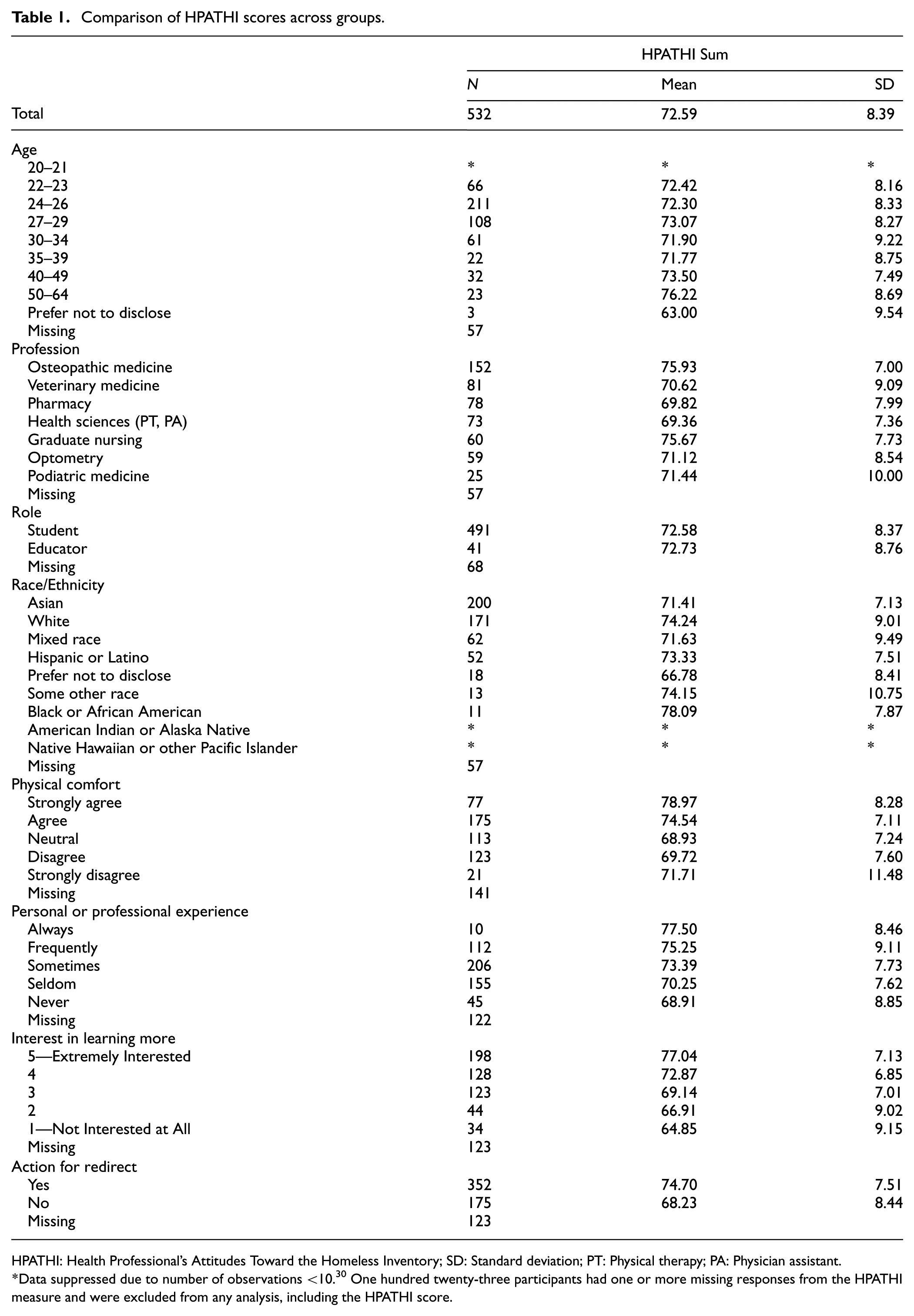
HPATHI: Health Professional’s Attitudes Toward the Homeless Inventory; SD: Standard deviation; PT: Physical therapy; PA: Physician assistant.
Data suppressed due to number of observations <10. 30 One hundred twenty-three participants had one or more missing responses from the HPATHI measure and were excluded from any analysis, including the HPATHI score.
HPATHI scores across health professions and educational roles
The HPATHI item set had a satisfactory level of internal consistency reliability with a Cronbach’s alpha of 0.844, indicating that the HPATHI remained reliable in the current study. The mean HPATHI score was 72.59, Standard deviation (SD) = 8.39 (Table 1). The one-way ANOVA revealed there was a statistically significant difference in HPATHI scores between the seven health professions colleges F (6,521) = 10.78, p < 0.001, ηp2 = 0.110, 95% CI [0.057, 0.153]. Tukey’s HSD tests indicated that students in Osteopathic Medicine (mean = 75.93) and Graduate Nursing (mean = 75.67) held significantly more positive attitudes toward PEH than students in Podiatric Medicine (mean = 71.44), Optometry (mean = 71.12), Veterinary Medicine (mean = 70.62), Pharmacy (mean = 69.82), and Health Sciences (mean = 69.36; Figure 1). The dental medicine college was excluded from this analysis for overall comparisons due to the limited number of respondents (n = 3). The independent samples t-test indicated no statistically significant difference in HPATHI scores between students versus educators, t (530) = −0.114, p = 0.455.
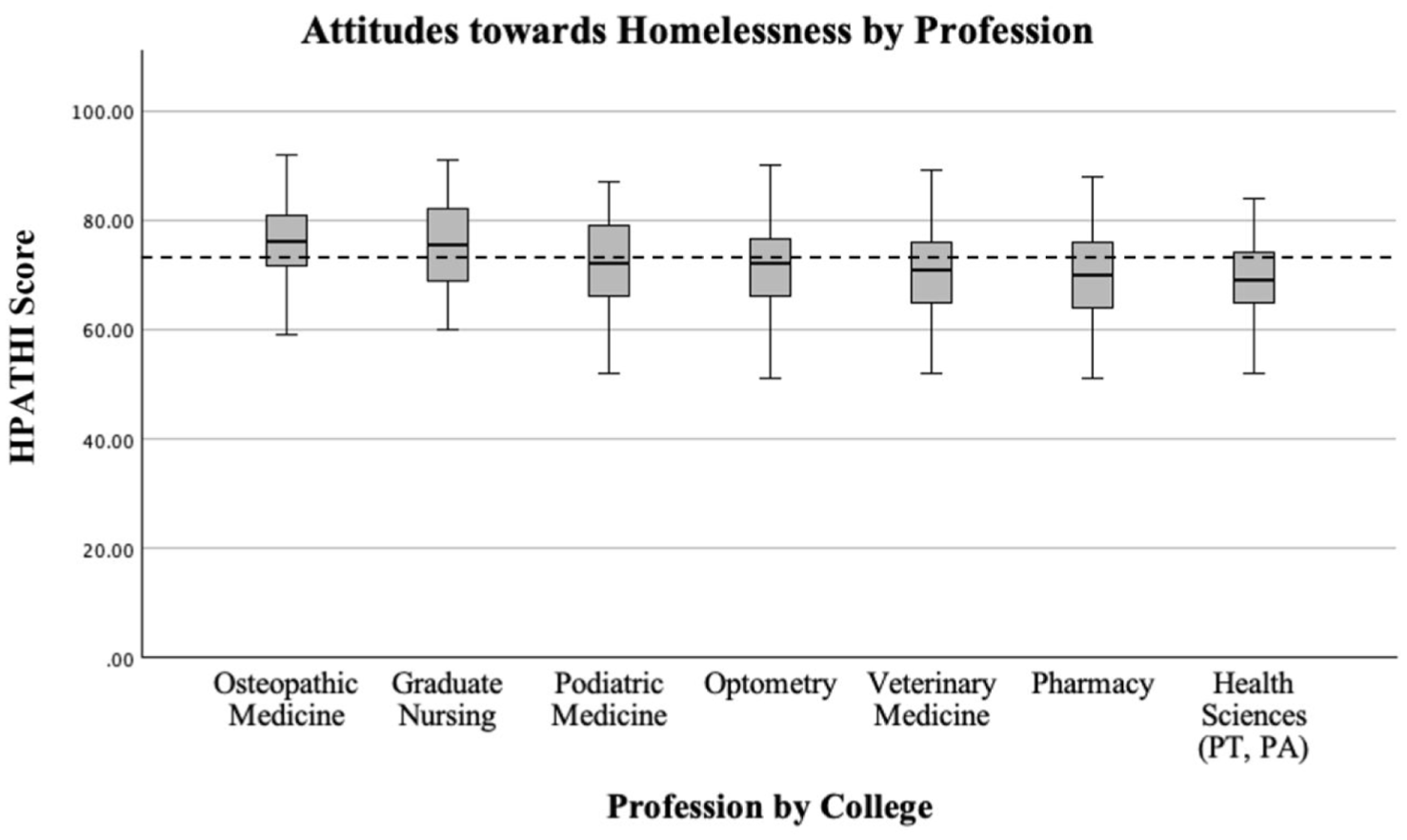
HPATHI scores and SDs by health profession college.
HPATHI scores by age and race
The one-way ANOVA showed no significant differences between age groups, F (8,522) = 1.24, p = 0.275, ηp2 = 0.019. A Welch’s ANOVA indicated that HPATHI scores were significantly different by race/ethnicity, F (3, 151.44) = 4.02, p = 0.009. The Games-Howell post hoc test found that the White group (mean = 74.24) held significantly more positive attitudes toward PEH than the Asian group (mean = 71.41, p = 0.006).
HPATHI scores by holistic learning theory dimensions
The HPATHI score was moderately positively correlated with physical comfort with PEH (ρ = 0.372, p < 0.001), frequency of interactions with PEH (ρ = 0.271, p < 0.001), and interest in learning more about homelessness (ρ = 0.482, p < 0.001), indicating that those who had more positive attitudes toward PEH tended to report greater physical comfort treating PEH, more frequent encounters with PEH, and greater interest in learning more about best practices when treating PEH (Table 2). Furthermore, responding “Yes” to being redirected to more information had a significantly higher HPATHI score than those who responded “No,”t (525) = 8.93, p < 0.001, Mean Difference = 6.47, 95% CI [5.04, 7.89], Cohen’s d = 0.83.
Bivariate correlations between HPATHI score and holistic learning theory dimensions.
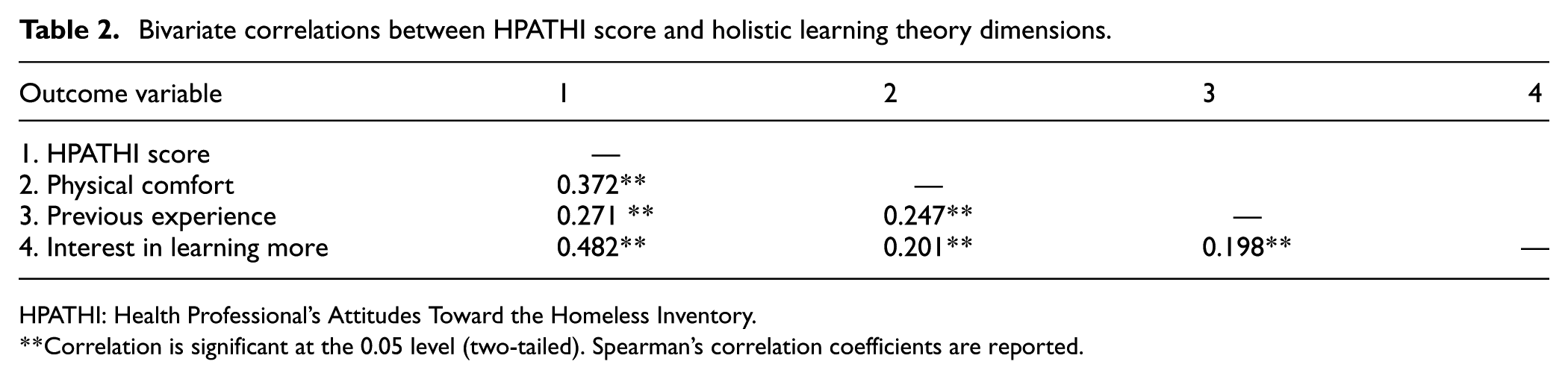
HPATHI: Health Professional’s Attitudes Toward the Homeless Inventory.
Correlation is significant at the 0.05 level (two-tailed). Spearman’s correlation coefficients are reported.
Holistic learning theory dimensions across professions
One-way ANOVA revealed significant differences between professions in physical comfort with providing care to PEH, F (6, 504) = 2.77, p = 0.012, ηp2 = 0.032, previous experience, F (6, 523) = 6.365, p < 0.001, ηp2 = 0.068, and interest in learning more, F (6, 522) = 11.83, p < 0.001, ηp2 = 0.120. Tukey’s HSD tests, detailed in Table 3, showed that Osteopathic Medicine reported significantly greater physical comfort than the College of Health Sciences (p = 0.039). Regarding previous experience, Graduate Nursing reported significantly more frequent experience than College of Health Sciences (p = 0.001), Optometry (p = 0.001), and Pharmacy (p = 0.001), while Osteopathic Medicine reported significantly more frequent experience than Pharmacy (p = 0.003). Regarding interest in learning more, Graduate Nursing expressed significantly greater interest than College of Health Sciences (p = 0.007), Optometry (p = 0.002), Pharmacy (p < 0.001), and Veterinary Medicine (p < 0.001). Similarly, Osteopathic Medicine reported significantly greater interest than College of Health Sciences (p < 0.001), Optometry (p < 0.001), Pharmacy (p < 0.001), and Veterinary Medicine (p < 0.001).
Tukey's Honestly Significant Difference (HSD) post hoc comparisons of holistic learning theory dimensions by profession.
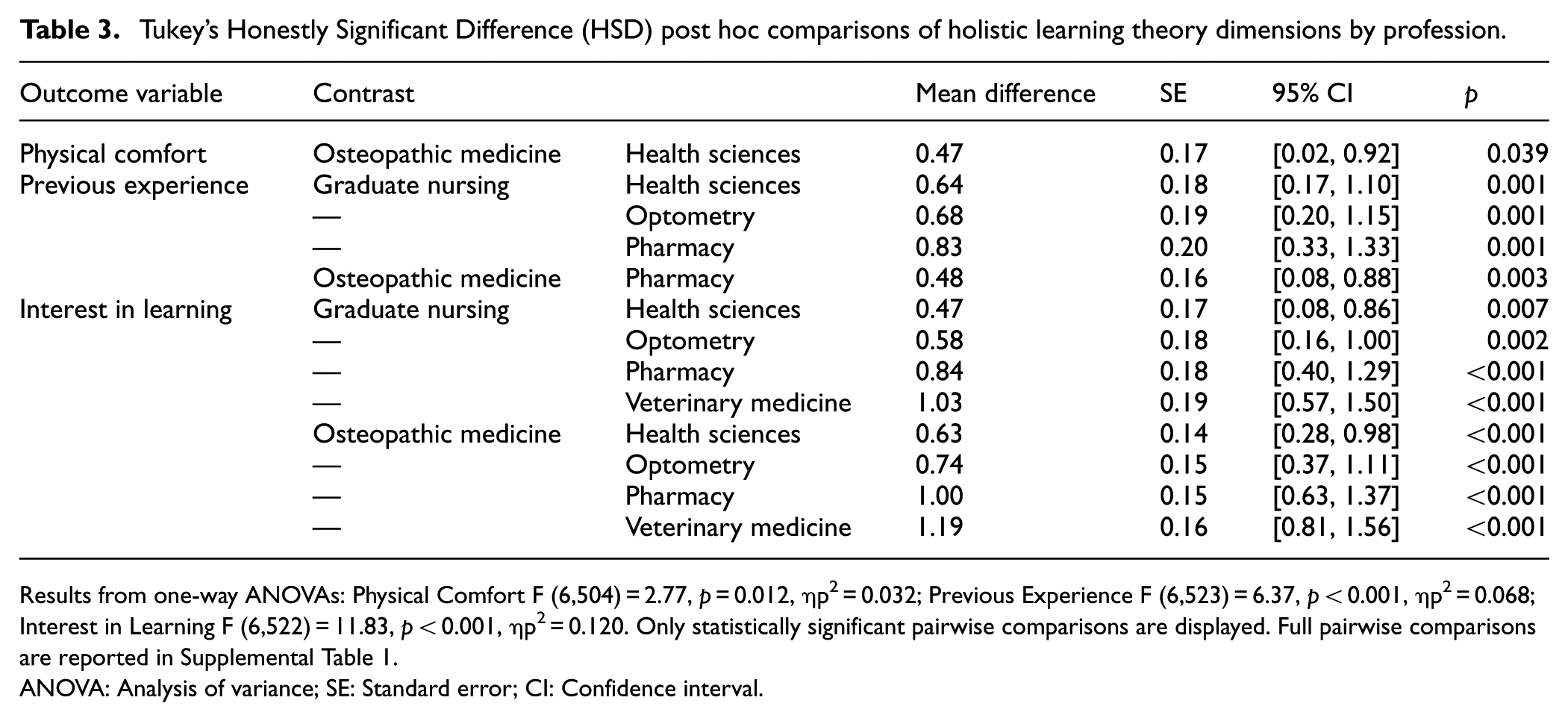
Results from one-way ANOVAs: Physical Comfort F (6,504) = 2.77, p = 0.012, ηp2 = 0.032; Previous Experience F (6,523) = 6.37, p < 0.001, ηp2 = 0.068; Interest in Learning F (6,522) = 11.83, p < 0.001, ηp2 = 0.120. Only statistically significant pairwise comparisons are displayed. Full pairwise comparisons are reported in Supplemental Table 1.
ANOVA: Analysis of variance; SE: Standard error; CI: Confidence interval.
Results remained consistent when educators, small age groups (20–21, 50–64, and Prefer not to disclose), and small race/ethnicity groups (Black or African American, Some Other Race, and Prefer not to disclose) were excluded from analysis.
Discussion
To our knowledge, this study is among the first to compare attitudes of students and educators from diverse health professional disciplines toward PEH. Overall, students and educators demonstrated positive attitudes toward PEH (Figure 1). Nevertheless, we found that attitudes differed between learning communities, and that individuals within the colleges of Osteopathic Medicine and Graduate Nursing held more favorable views than did those in the colleges of Veterinary Medicine, Health Science, and Pharmacy (Figure 1). Although all health professionals interact in some way with PEH, the role each professional plays in their care, as well as the volume of PEH they encounter, differs and may affect overall attitudes toward this population. Examining the curriculum and educational settings within each professional school may illuminate differences that could impact healthcare provider attitudes toward PEH. 26
Our study also measured three dimensions of the Holistic Learning Theory to conceptualize factors that further the process of learning and the effect they may have on attitudes toward PEH. We found that individuals with greater physical comfort, more experience with PEH, and an interest in learning tended to hold more favorable attitudes toward PEH (Table 2). Because more frequent experiences with PEH were associated with more positive attitudes, increased integration of PEH encounters into health professions education could lead to further improvements in attitudes and behaviors among practicing professionals. Indeed, several interventions, including experiential learning, seem to show effectiveness in improving attitudes toward PEH.31–33 However, exposure to PEH alone may be inadequate in garnering more positive attitudes. The quality of those experiences, coupled with didactic learning, may be more effective. 34 More positive attitudes toward PEH correlate with the likelihood to take action to learn more (Table 2). Harnessing this action into experiential learning could bridge the gap in which students have expressed a lack of self-efficacy in caring for PEH. 21 In one study of medical students, elective experiential learning following didactic educational events improved knowledge, self-efficacy, and social advocacy ratings. 35 Such holistic learning can be effective in promoting personal and social advocacy in students with initially favorable attitudes. However, given the diversity in attitudes found in our study, it would be pertinent to intervene with both didactic and experiential learning opportunities for all students, regardless of their initial attitudes. For example, six nursing students who completed a pilot shelter-based practicum also demonstrated improved knowledge and skills, as well as more favorable HPATHI scores, after treating and working with PEH. 27 At a multidisciplinary health professions school, Greenfield et al. employed an interprofessional, multimodal educational model that included didactics, street medicine rounds, and simulation. They found a post-intervention increase in HPATHI scores, especially for social and personal advocacy, as well as improved self-efficacy on a self-reported scale. 36
Our findings differ from prior studies that demonstrated less favorable attitudes toward homelessness among post-graduates, such as residents and attending physicians. Furthermore, we found no association between attitudes and age. These inconsistencies with prior studies may be due to our inclusion of non-clinical educators in the sampling. The relatively small sample size of educators compared to students may have also contributed to this difference. Clinical and non-clinical educators’ attitudes toward homelessness may differ due to variabilities in exposure to PEH over their careers. Though our study attempted to measure “time in profession,” the data collected from this question were invalid due to confusing wording. Future studies should investigate the relationship between time-in-practice and attitudes toward PEH. Another issue worthy of further consideration is how HPATHI scores are associated with relevant healthcare delivery outcomes (e.g. clinical practice and patient communication). Understanding such a relationship is essential to evaluating whether healthcare providers’ attitudes toward PEH are clinically relevant to the quality of healthcare provided. Relatedly, future studies may explore the discriminative validity of the HPATHI for clinical outcomes and possibly establish optimal cut-off scores that might effectively distinguish between healthcare providers’ attitudes toward PEH and the predictability of relevant health outcomes.
This study raises several areas for future investigation. Variations in curriculum and health profession-specific biases should be explored for contributions to differences in attitudes toward PEH. Future research may also explore whether increased experiential learning and frequency of physical interaction overall improve attitudes toward PEH.
There are several limitations and strengths to this study. First, we had a low response rate (13.7%) that may have contributed to underpowering, and pursuing a convenience sampling at a single institution limits the generalizability of the findings. Furthermore, the majority of respondents were students (92%), thus limiting comparisons with educators (8%). Second, the survey may suffer from selection and social desirability bias. Individuals with more favorable attitudes toward PEH may be more likely to complete the survey, which may inflate the mean attitude score and limit the external validity of the study. However, the demographic characteristics of our sample (Table 1) were comparable to those of the WesternU population, including race (43.50% Asian, 30.90% White, 17.30% Hispanic/Latino, 3.10% Black/African American, 1.8% Two or more) and age (mean age = 27.5 years, Table S2). Similarly, the distribution of student professions in our sample was comparable to that of the WesternU population. Gender was not available for comparison. These factors should be considered when interpreting the results. Third, the HPATHI was designed to measure attitudes of healthcare workers, and not non-clinical educators. Further investigation should also elucidate any differential attitudes toward PEH between clinician-educators and non-educator clinicians. Fourth, the cross-sectional nature of our study was not designed to assess whether attitudes toward PEH changed over time from entrance to the respective health professions program through graduation. Strengths of the study include a novel study design, a novel study subject, and one of the largest sample sizes surveyed with the HPATHI. Cross-sectional design at a large interprofessional institution serves to establish a powerful baseline understanding of attitudes overall in a group of future and current health professionals, as well as possible modifiers such as physical comfort, previous experience, and interest in learning more.
Health professions students’ attitudes toward PEH are shaped by prior exposure, physical comfort, and interest in learning more about homelessness, with osteopathic and graduate nursing students holding more positive attitudes compared to their peers in other disciplines. These patterns may reflect differences in student backgrounds, training, clinical exposure, or other factors. Prior experience with PEH—through volunteer work, clinical care, or lived experience—is consistently associated with more favorable attitudes. In addition, interest in learning more about homelessness correlates with greater empathy and clinical comfort. These results highlight the need for profession-specific educational interventions that build both didactic and experiential learning. Longitudinal and experiential holistic learning opportunities may be especially valuable in fields where students report lower baseline comfort. Embedding this content into core curricula can help ensure that all future clinicians are equipped to effectively and holistically care for individuals experiencing homelessness. By fostering empathy, awareness, and sustained contact, health professions educational programs can prepare students to better address the health needs of this marginalized population.
Supplemental Material
sj-docx-1-imj-10.1177_10815589251406146 – Supplemental material for Differences in attitudes among health professions students and educators toward people experiencing homelessness: Novel correlations with physical comfort, prior experiences, and interest in learning
Supplemental material, sj-docx-1-imj-10.1177_10815589251406146 for Differences in attitudes among health professions students and educators toward people experiencing homelessness: Novel correlations with physical comfort, prior experiences, and interest in learning by Elisabeth Gilmore, Clarice Szeto, Eli Spector, Yusuke Shono and Andrew Pumerantz in Journal of Investigative Medicine
Footnotes
Appendix 1
Acknowledgements
We would like to express our gratitude to Dr. Stephanie White, Dr. Sébastien Fuchs, and Corinne Feldman for providing invaluable mentorship and feedback in the early stages of this research.
Ethical considerations
This study received approval on August 7, 2023, from the Institutional Review Board for the Protection of Human Subjects (IRB) of Western University of Health Sciences (WesternU) (IRB #2020292-1).
Consent to participate
Study responses were anonymized before being stored and without human knowledge or intervention. Consent to participate was displayed and required to be acknowledged by participants prior to beginning the survey on the Qualtrics platform. Information about resources available to individuals who may experience emotional distress when filing this survey was provided in the consent statement.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 2023 Western University Student Research Fellowship.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.