
Abstract
Summary
Use of antipsychotic drugs has been associated with increased risk of venous thromboembolism in several observational studies with unclear mechanism. We present a case of a patient who experienced a significant event of venous thromboembolism after a few months exposure to atypical antipsychotic drug for his bipolar mood disorders.
Case description
A 58-year-old male with a history of hypertension, coronary artery disease and dilated cardiomyopathy was admitted with a picture of heart failure. The patient had also a longstanding history of bipolar mood disorder and anxiety disorder following up with psychiatric service. There were no symptoms or signs of ongoing ischemia on Electrocardiogram (ECG). His blood pressure was 115/60 mmHg, pulse was 80 beats per minute and oxygen saturation of 94%. Examination of the chest showed bilateral basal crepitation. There was mild bilateral lower limb edema. His chronic medications include Ramipril 5 mg once daily (OD), bisoprolol 2.5 mg OD, spironolactone 25 mg OD, furosemide 40 mg twice daily, aspirin 100 mg OD. For Bipolar mood disorder and anxiety he was on two mood- stabilizing drugs (Sodium valproate and clonazepam) and antidepressant (vortioxetine). He was started 3 months before on atypical antipsychotic drug (paliperidone) to control the symptoms of his bipolar disorder. His echocardiographic findings showed evidence of right ventricular strain and pulmonary hypertension and these findings were new as compared to his previous study. An evidence of dilated right ventricle (RV) and flatting of interventricular septum (IVS) causing D- Shape of the left ventricle (LV) indicating RV pressure overload (Figure 1). On the other hand, a mid systolic notch seen on the right ventricular outflow track (RVOT) pulse flow Doppler (Figure 2) indicating precapillary pulmonary hypertension. The combination of these new findings raised the suspicious of a vascular pulmonary event in particular pulmonary embolism. The Computed Tomography pulmonary angiogram (CTPA) showed a saddle embolus in the bifurcation of main pulmonary artery extending to both right and left branches of pulmonary artery (Figure 3). Although there were no clinical signs of deep venous thrombosis, the Doppler venous system of the lower limb revealed thrombosis of right popliteal vein (Figure 4). Based on the imaging information the diagnosis of extensive pulmonary embolism and right lower limb deep venous thrombosis established and patient started on therapeutic dose of anticoagulation. Our patient had several risk factors of venous stasis and venous thrombosis, however, the new exposure to another new risk factor like antipsychotic medication few months before this hospitalization may also contribute and increase the chance of having thromboembolic events. A consultation with psychiatric service confirmed the possible side effect of paliperidone and advice to discontinue the medication and to continue on mood stabilizing medications and antidepressant. The course of the hospital stay went smooth and the patient discharged on oral anticoagulation.

Transthoracic echocardiography. Short axis view of left ventricle – Flattening of interventricular septum (red arrow) and D shape of left ventricle. Dilated right ventricle. LV – left ventricle, RV – right ventricle.
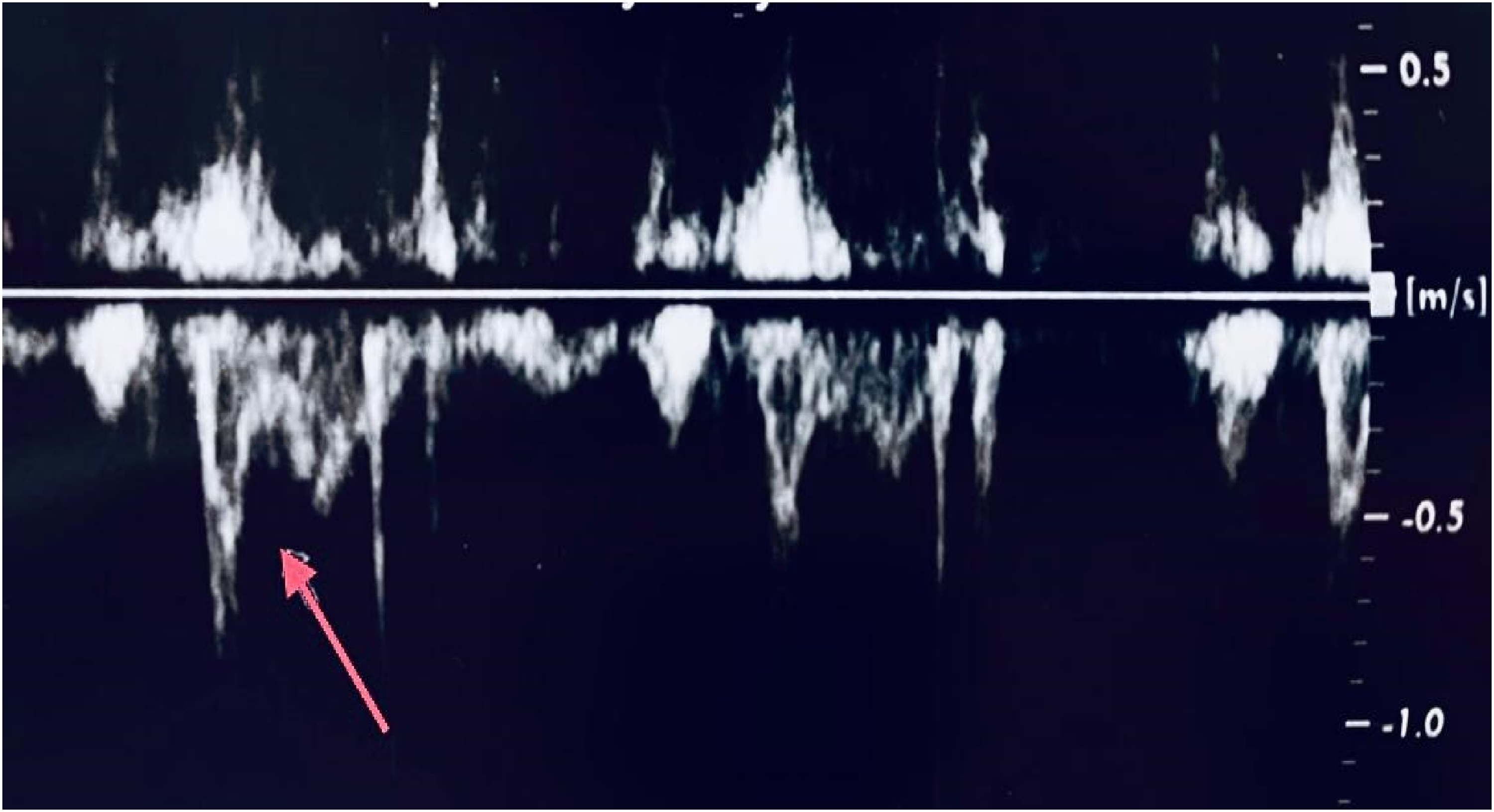
Right ventricular outflow (RVOT) pulse flow Doppler showed mid-systolic notch (red arrow) – a sign of precapillary pulmonary hypertension.

Computed tomography pulmonary angiogram (CTPA) demonstrating a saddle embolus. (Red arrows). Grey matter is a blood clot in the bifurcation of pulmonary artery extending to both right and left branches of pulmonary artery. MPA-main pulmonary artery.
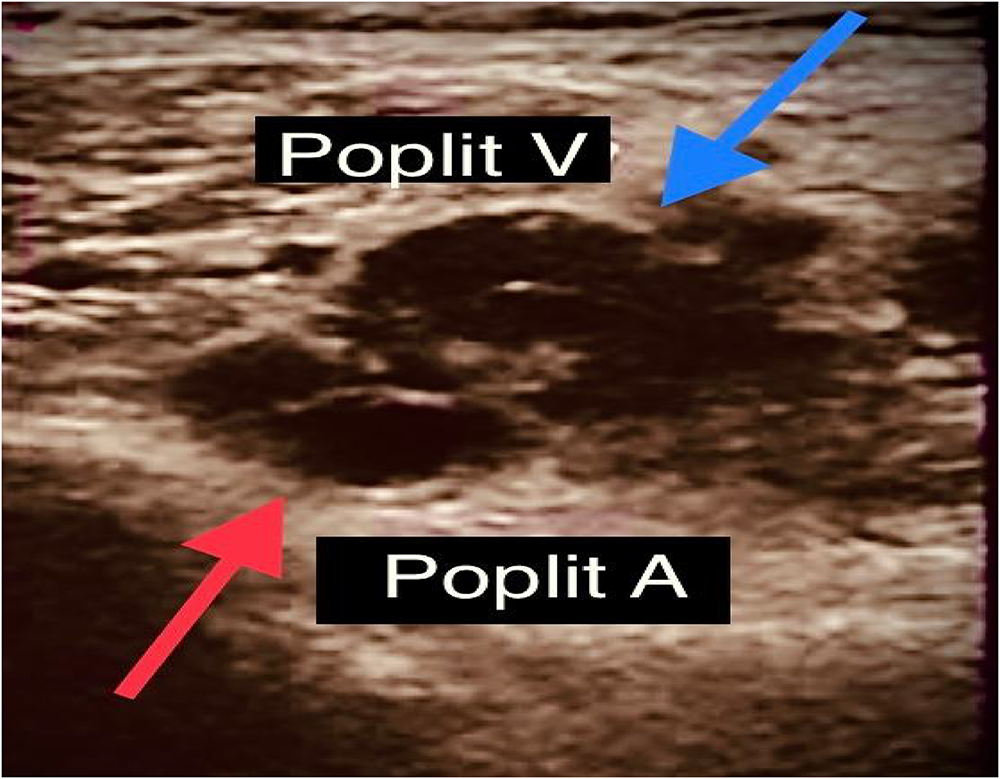
Transverse B mode image showing the non-compressible right popliteal vein (blue arrow). Poplit V- popliteal vein, Poplit A- Popliteal artery (red arrow).
Discussion
The term venous thromboembolism (VTE) consists of deep vein thrombosis (DVT) and pulmonary embolism (PE) that annually affects 1–1.8 per 1000 adult and can lead to a serious complication. 1 In some observational studies that took place in nineties of previous century and included patient with schizophrenia and related disorders the incidence of PE among these patients was relatively high, however the link association was not widely admitted. 2 Later in 2000, Zornberg et al. in a large case-control study demonstrated that the risk of VTE among patients treated with first-generation antipsychotic drug is seven times higher than non-users. 3 The relation between the use of antipsychotic drug and the increased risk of VTE was supported in several case–control studies, cohort studies and drug surveillance studies. A retrospective cohort study on residents of nursing home receiving atypical antipsychotic drugs concluded that the risk of hospitalization due to VTE among elderly patient is high, however, these events are rare. 4 A meta-analysis and systematic review in 2014 done by Barbui et al. looked at the occurrence of VTE in patients exposed to antipsychotic drugs in comparison with those unexposed to such agents and concluded that the use of antipsychotic agent associated with a 50% increase risk of VTE and it was similar between the first and second generation of antipsychotic drugs. 5 Another meta-analysis with 22 studies demonstrated clearly the increased risk of VTE in patient using antipsychotic drugs and the young people were at a higher risk of VTE than elderly. 6 In 2021 a meta-analysis included a 28 observational studies demonstrated a significant higher risk of VTE among users of antipsychotic drugs compared to non-user. A subgroups analysis in this review showed that a new users are more likely to develop VTE and the risk of VTE recurrence increased with the exposure of antipsychotic drugs, however, the conclusions drawn from this meta-analysis should be considered with caution due to heterogeneity among studies. 7 Based on the result of this meta-analysis the initial period of exposure to antipsychotic drugs carries more risk for VTE.
An interesting data was found in a recent systematic review where a 34 cases of pulmonary embolism documented after exposure to clozapine and almost 50% of these patients did not have significant risk factor or co-morbidities for VTE denoting that the use of clozapine significantly increases risk of pulmonary embolism. 8
The pathophysiologic mechanisms explaining the increased risk of VTE among patient receiving antipsychotic medication remains unclear. The factors that may contribute to the occurrence of VTE include the Psychotic disorders itself and the exposure to antipsychotic drugs. A specific psychiatric symptoms may have an increased risk of VTE which were described in a case series of 22 patients with pulmonary embolism related to catatonic syndrome. 9
Immobilization resulted from social withdrawal due to negative symptoms of schizophrenia and major depressive disorders in addition to the sedative side effect of antipsychotic drugs can cause significant venous stasis which considered a well-known risk factor contribute to VTE. Obesity is a known side effect of second generation antipsychotic drugs and in combination with metabolic syndrome can lead to increased platelet activity via the inflammation process. 10 Binding of atypical antipsychotic drugs to a serotonin receptor type 2A with high affinity may increase the platelet aggregation that can play a role in VTE. 11 An increased level of antiphospholipid antibodies found in the patient receiving antipsychotic drugs is an established risk for VTE, 12 however the clinical impact of such high level is uncertain. Hyperprolactinemia is an adverse effect for high-potency first generation antipsychotic and risperidone which may also play a role since Prolactin is a potent platelet aggregation co-activator. 13 In patients with schizophrenia, an elevated level of homocysteine has been observed and might play a role in VTE. 14 Individual risk factors assessment for VTE before commencing antipsychotic drugs should be considered especially in high risk situation where adding such agent will increase the risk of VTE. The individuals who are at high risk for VTE and using antipsychotic drugs should be informed and educated about the symptoms of DVT and PE in addition to the importance of seeking immediately medical care.The individuals who suffered DVT or PE should be managed according to current guidelines and the decision of discontinuing or switching the antipsychotic treatment should be considered. Our patient had several risk factors of venous stasis and venous thrombosis, however, the new exposure to another new risk factor like antipsychotic medication few months before his hospitalization may be a contributing factor that increase the chance of having thromboembolic events.
Conclusion
The use of antipsychotic drugs associated with an increased risk of venous thromboembolic events. Physician should be aware of such possible side effects in order to reach early diagnosis and subsequent treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author contributions
Consent
Informed consent was obtained from the patient for the publication of this case report.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.